
Abstract
Background:
The International Knee Documentation Committee Subjective Knee Form (IKDC-SKF) is a knee-specific patient-reported outcome (PRO) measure that is commonly used to evaluate patients with various knee disorders. The Thai version of the IKDC-SKF (Thai IKDC-SKF) was shown to have good validity and reliability; nonetheless, no data regarding its responsiveness are available.
Purpose:
To evaluate the responsiveness of the Thai IKDC-SKF for assessing patients with anterior cruciate ligament (ACL) injury and determine the minimal clinically important difference (MCID) for this PRO measure.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
This prospective study included ACL-injured patients who were scheduled for ACL reconstruction (ACLR) at a single institution. The patients completed the Thai IKDC-SKF at the baseline and the 6-month postoperative follow-up. The global rating of change scale was an anchor question that evaluated patients’ overall perception of a clinical change compared with their preoperative condition. The effect size and standardized response mean were calculated. The MCID was identified with an anchor-based approach by plotting a receiver operating characteristic curve and calculating the value that maximized the Youden index.
Results:
Of 59 enrolled patients, 53 patients (89.8%) completed the preoperative and 6-month postoperative Thai IKDC-SKF. The mean (±SD) age of the participants was 32.3 ± 10.3 years, and 86.8% were men. The mean Thai IKDC-SKF score improved significantly from preoperatively to the 6-month follow-up (from 56.3 ± 14.9 to 70.8 ± 14.1, respectively; P < .001), with an effect size of 0.975 and a standardized response mean of 0.977. A receiver operating characteristic curve was generated to determine the ability of the Thai IKDC-SKF to distinguish between improved patients and unimproved patients, and the area under the curve was 0.80 (95% CI, 0.68-0.92), which was considered excellent. The MCID was 15.5, which yielded a sensitivity and specificity of 0.55 and 1, respectively.
Conclusion:
This study confirmed the responsiveness of the Thai IKDC-SKF for detecting a clinical change in ACL-injured patients after ACLR. The identified MCID of 15.5 can be used to calculate the significant clinical change and sample size in future studies.
Keywords
Patient-reported outcome (PRO) measures assess the patient’s perspective of their health status without interpretation of the patient’s response by the physician or others. 21 PRO measures have been used to determine the impact of medical conditions and the results of treatment. They can be categorized as general or disease-specific. PRO assessment is an important component of a comprehensive assessment of patients with anterior cruciate ligament (ACL) injury, in addition to a clinical evaluation of the knee and incidence of adverse events and ACL graft failure. 25
The International Knee Documentation Committee Subjective Knee Form (IKDC-SKF) is a knee-specific PRO measure that assesses the patient’s perception of symptoms, function during daily activity, and the level of symptom-free sports activity. 11 The original version of the IKDC-SKF has demonstrated good test-retest reliability, validity, and responsiveness in the evaluation of patients with a variety of knee conditions.11,12 The IKDC-SKF has been recommended as an effective knee-related outcome tool after ACL reconstruction (ACLR).25,29,30
The IKDC-SKF has been translated into several languages, including Thai. 16 The Thai version of the IKDC-SKF (Thai IKDC-SKF) has demonstrated good construct validity and excellent test-retest reliability 16 ; however, there are no data regarding its responsiveness. Responsiveness is defined as the ability of a questionnaire to detect a clinical change over time in the measured construct.5,19 The minimal clinically important difference (MCID) is a calculated threshold value in a PRO measure that reflects what patients perceive as a clinically meaningful change in their condition.5,6 This value is required for power calculation and sample size estimation in future studies that use the Thai IKDC-SKF questionnaire to evaluate the outcomes of treatment.
The aims of this study were to evaluate the responsiveness of the Thai IKDC-SKF for assessing patients undergoing primary ACLR and determine the MCID for this PRO measure. It was hypothesized that the Thai IKDC-SKF would be found to be a responsive PRO measurement tool that can detect a change in a patient’s health status after undergoing ACLR.
Methods
This prospective cohort study was conducted at a single institution between June 2020 and August 2022. Patients aged >18 years who were diagnosed with ACL injury and scheduled to undergo ACLR were eligible for inclusion. The exclusion criteria were as follows: multiligament knee injury; bilateral knee injury; psychological disorder; neurocognitive disorder; insufficient knowledge of the Thai language; or refusal to participate. The protocol for this study received institutional review board approval, and written informed consent was obtained from all participants.
Surgical Procedure
All patients underwent anatomic single-bundle ACLR using either a bone–patellar tendon–bone autograft or a hamstring tendon autograft. The autograft decision was made by the patient after a discussion with the surgeon about the risks and benefits of each autograft type. The patients underwent surgery in a hemilithotomy position. Initial assessment of the knee and treatment of meniscal lesions were performed with a 30° arthroscope. A 70° arthroscope was then used for visualization of the ACL footprint. The femoral tunnel was drilled at the center of the ACL footprint using the transportal technique. Later, the tibial tunnel was created at the center of the tibial ACL footprint. Graft fixation was performed in the full extension position of the knee. Intraoperative data and findings—including the autograft type, associated intra-articular lesions, and concomitant procedures—were recorded.
Data Collection
Included patients were asked to complete the Thai IKDC-SKF at the baseline and provide demographic and clinical data—including age, sex, weight, height, injured side, and their preinjury Tegner activity level. At the 6-month postoperative follow-up visit, each patient completed the Thai IKDC-SKF again and completed the global rating of change (GRoC) scale.
The Thai IKDC-SKF consists of 18 items, with a total score ranging from 0 to 100. A higher total score indicates less symptoms, better function, and a higher level of sports activity.11,16 The 7-level GRoC scale was an anchor question (“How would you rate the overall condition of the affected knee compared with the preoperative condition?”), which was used to evaluate patients’ overall perception of a clinical change compared with their preoperative condition. The 7 response levels of the GRoC scale were as follows: greatly worse (–3); somewhat worse (–2); slightly worse (–1); no change (0); slightly better (+1); somewhat better (+2); and greatly better (+3).
Statistical Analysis
All statistical analyses were performed using PASW Statistics for Windows Version 18.0 (SPSS Inc), and P < .05 was regarded as statistically significant for all tests. Descriptive statistics were used to summarize patient demographic and clinical characteristics. Categorical data are reported as frequency and percentage. Normally and nonnormally distributed continuous data are presented as mean with standard deviation and median with range, respectively. The change score for each patient was calculated by subtracting the baseline Thai IKDC-SKF score from the 6-month follow-up Thai IKDC-SKF score, with a positive change score reflecting clinical improvement.
Three constructs of change were used to evaluate the responsiveness of the Thai IKDC-SKF. The first construct of change was a group-level analysis of the within-patient observed change from before to after treatment. The 6-month change score was used to calculate the effect size and standardized response mean (SRM). The effect size was defined as the mean change score divided by the standard deviation of the baseline scores, and the SRM was defined as the mean change score divided by the standard deviation of the change scores. 24 It was hypothesized that patients would improve after ACLR surgery, and this would result in a relatively large effect size and SRM.
The second construct of change was a group-level analysis of the between-group difference in change scores. The 7-level GRoC scale was used to classify patients into 3 groups. The improved group included patients who had a GRoC of greatly better or somewhat better. The unchanged group consisted of patients with a GRoC of slightly better, no change, or slightly worse. The worse group included patients with a GRoC of somewhat worse or greatly worse. The Thai IKDC-SKF change score was compared using the Mann-Whitney U test between the improved group and the unchanged group because there were no patients in the worse group in this study. It was hypothesized that the magnitude of the change scores would be related to the patient’s perceived global change after treatment and that the improved group would have a higher mean change score than the unchanged group.
The third construct of change was an individual-level analysis of between-group difference. To perform this analysis, a dichotomous variable (improved vs unimproved), which was derived from the GRoC scale data, was used to generate a receiver operating characteristic (ROC) curve to evaluate the ability of the Thai IKDC-SKF change score to distinguish between an improved patient and an unimproved patient. The improved group included patients who perceived their change as greatly better or somewhat better. The unimproved group consisted of patients who perceived their change as slightly better, no change, or slightly worse. Using the dichotomized criterion measure of change, the sensitivity and specificity were calculated for each observed Thai IKDC-SKF change score. To determine the MCID or the optimal change score cutoff between the improved and unimproved groups, a ROC curve was plotted with 1-specificity on the x-axis and sensitivity on the y-axis. The area under the curve (AUC) reflects the ability of a PRO measure to correctly categorize a patient as either improved or unimproved. An AUC >0.70 is considered to be acceptable. 8 The MCID was determined with the Youden index to identify the cutoff value having the maximum sum of sensitivity and specificity. 32
The minimal detectable change (MDC) is the smallest change score that can distinguish a true health change from variability resulting from measurement error. The MDC was calculated using a distribution-based approach and the standard error of measurement (SEM). The SEM was calculated with the formula SD×√ (1 –ICC) and using the standard deviation of baseline scores from the present study and the intraclass correlation coefficient (ICC) from a previous study of the Thai IKDC-SKF. 16 The SEM was converted to the MDC using the formula SEM× 1.96 ×√2. If the MCID is larger than the MDC, change scores as large as the MCID can be considered statistically significant and important to patients. In contrast, if the MCID is smaller than the MDC, change scores as large as the MCID may be important to patients, but they cannot be distinguished from measurement error. 7
Results
A total of 59 patients with ACL injury who were scheduled to undergo primary ACLR were originally enrolled in this study. However, 6 of those patients were lost to follow-up because of the COVID-19 pandemic (Figure 1). The remaining 53 patients (89.8%) completed the preoperative and 6-month postoperative Thai IKDC-SKF and were included in the final analysis. The mean age of those 53 patients was 32.3 ± 10.3 years, and 46 (86.8%) were men. Patient characteristics and clinical data are shown in Table 1, and patient surgical data are shown in Table 2.

Flow diagram describing patient enrollment and the flow of patients in this study. ACLR, anterior cruciate ligament reconstruction; GRoC, global rating of change; Thai IKDC-SKF, Thai version of the International Knee Documentation Committee Subjective Knee Form.
Patient Characteristics and Clinical Characteristics (N = 53) a
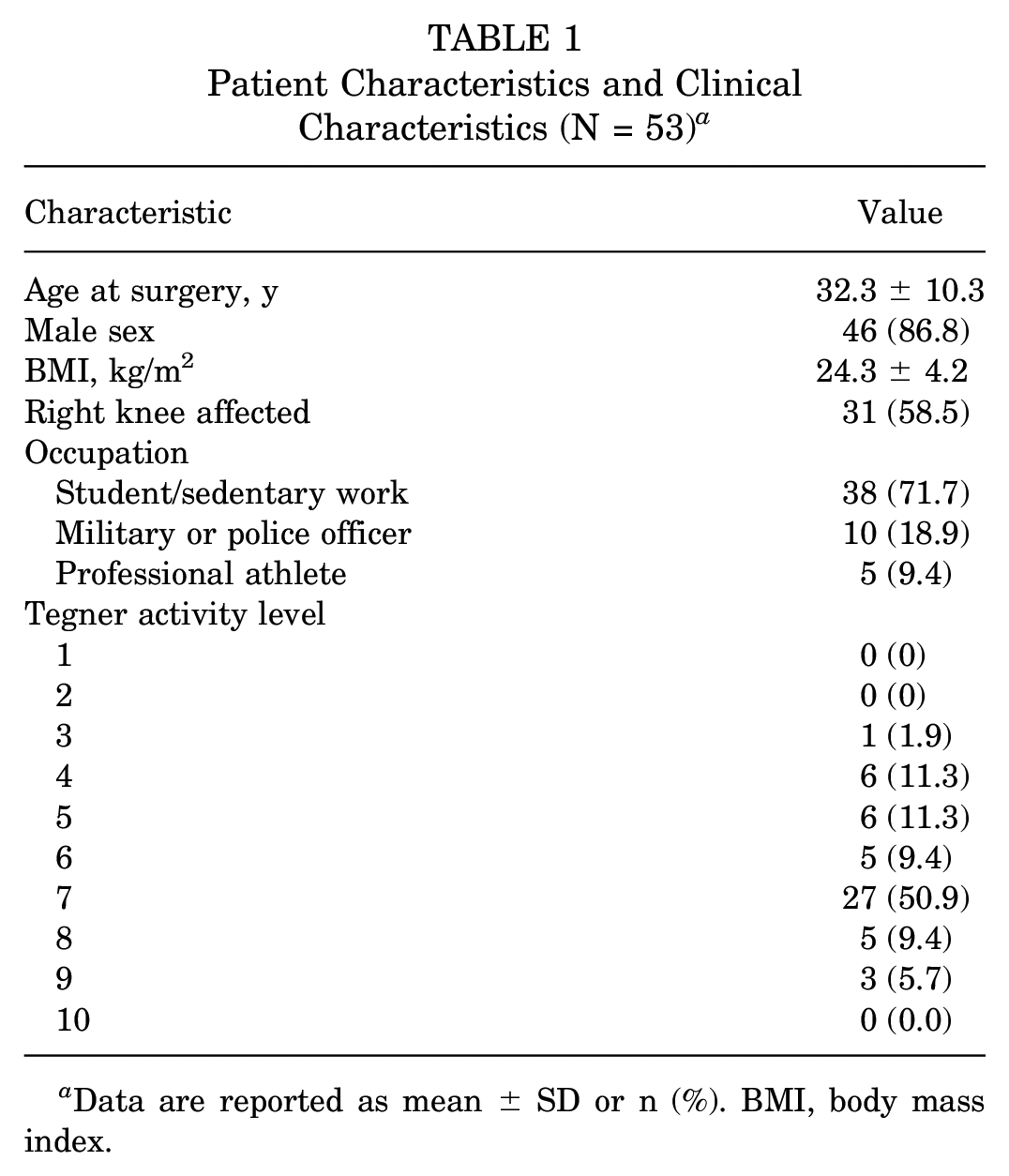
Data are reported as mean ± SD or n (%). BMI, body mass index.
Patient Surgical Data (N = 53) a
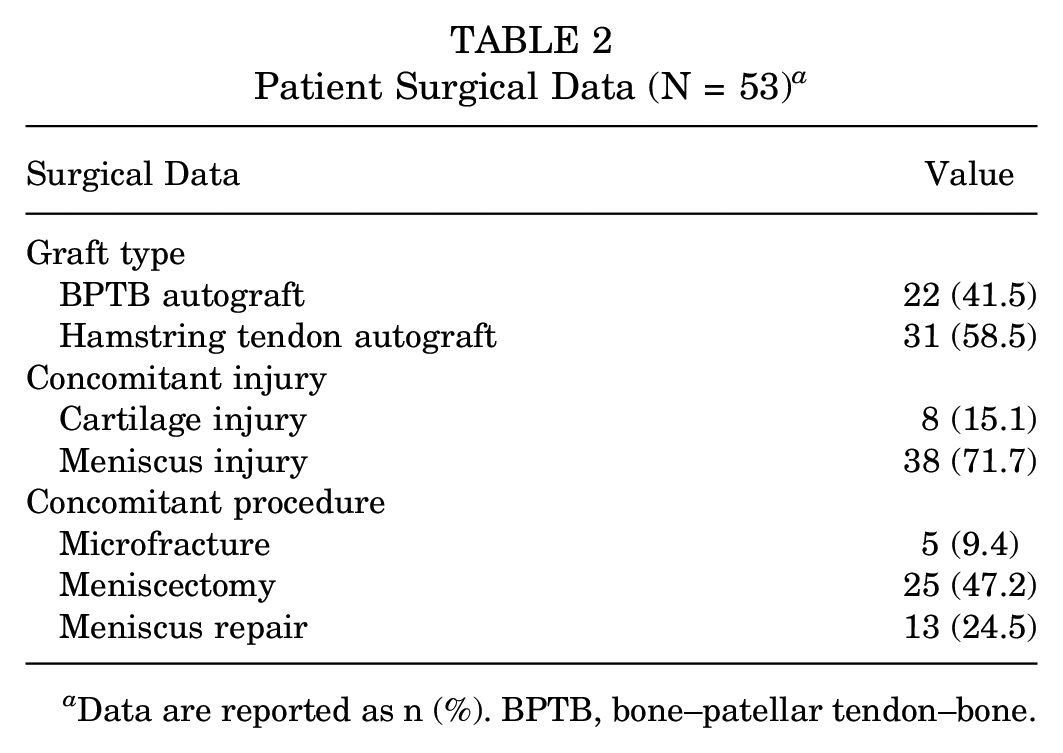
Data are reported as n (%). BPTB, bone–patellar tendon–bone.
The mean baseline and 6-month postoperative Thai IKDC-SKF scores are shown in Table 3. The scores improved significantly from the baseline to postoperatively, from 56.3 ± 14.9 to 70.8 ± 14.1, respectively (P < .001). The overall mean change in the Thai IKDC-SKF score was 14.6 ± 14.9. The calculated effect size was 0.975, and the SRM was 0.977, indicating large effect 4 and large responsiveness. 17
Thai IKDC-SKF Baseline, Postoperative, and Change Scores for 5 of 7 Levels of the GRoC Scale a

GRoC, global rating of change; Thai IKDC-SKF, Thai version of the International Knee Documentation Committee Subjective Knee Form.
No patient perceived/reported greatly worse or somewhat worse.
SD not applicable (n = 1).
The mean Thai IKDC-SKF scores for 5 of the 7 levels of the GRoC scale (no patients reported somewhat worse or greatly worse in this study) are also shown in Table 3. There were 40 patients in the improved group and 13 in the unchanged group. The median Thai IKDC-SKF change score in the improved group was significantly larger than in the unchanged group (17.6 vs 4, respectively; P = .001).
The ROC curve to determine the specificity and sensitivity of the Thai IKDC-SKF change score for distinguishing improved from unimproved patients after ACLR is shown in Figure 2. The AUC was 0.80 (95% CI, 0.68-0.92), which is considered excellent. The MCID value calculated using the Youden index was 15.5. This cutoff value yielded a sensitivity of 0.55 and a specificity of 1 for distinguishing improved patients from unimproved patients after ACLR. The calculated MDC of the Thai IKDC-SKF score was 11.7.

A ROC curve to determine the specificity and sensitivity of the Thai IKDC-SKF score for distinguishing improved from unimproved patients after ACLR. The AUC was 0.80, which is considered excellent. ACLR, anterior cruciate ligament reconstruction; AUC, area under the curve; ROC curve, receiver operating characteristic curve; Thai IKDC-SKF, Thai version of the International Knee Documentation Committee Subjective Knee Form.
Discussion
The results of this study demonstrate that the Thai IKDC-SKF is a responsive PRO measure that can successfully detect a change in a patient’s health status after undergoing ACLR. Responsiveness of the Thai IKDC-SKF was demonstrated by analysis of 3 constructs of change, as follows.
The first construct of change was a group-level analysis of the within-patient observed change from before to after treatment. This analysis confirmed that patients’ mean Thai IKDC-SKF score significantly improved after ACLR surgery. The effect size and SRM values calculated in the present study were large. 4 Table 4 summarizes the results from previous studies that investigated the responsiveness of the IKDC-SKF.3,10,12-15,27 The effect size ranged from 0.80 to 2.09, and the SRM ranged from 0.69 to 2.39. In the studies specific to patients undergoing ACLR, the effect size and SRM ranged from 0.80 to 2.093,10,27 and from 0.69 to 1.90,14,27 respectively.
Results From Previous Studies Concerning the Responsiveness of the IKDC-SKF a

ACL, anterior cruciate ligament; AUC, area under the receiver operating characteristic curve; ES, effect size; IKDC-SKF, International Knee Documentation Committee Subjective Knee Form; MCID, minimal clinically important differences; MDC, minimum detectable change; NA, not applicable; SEM, standard error of measurement; SRM, standardized response mean.
The second construct of change was a group-level analysis of the between-group difference in change scores. It was confirmed that the magnitude of the change scores was related to the patient’s perceived global change after treatment. No patient perceived/reported “somewhat worse” or “greatly worse.” For the remaining groups, the median change was significantly higher in the improved group than in the unchanged group. Huang et al 10 demonstrated that the correlation between the change scores of the Japanese IKDC-SKF and the 7-level GRoC scale at 3 months after ACLR was 0.46.
The last construct of change was an individual-level analysis of between-group differences. The ROC curve demonstrated the ability of Thai IKDC-SKF change scores to distinguish between improved and unimproved patients. The ability of a measurement tool to discriminate between 2 states is considered acceptable when the AUC is >0.70. In the present study, the AUC was 0.80, which corresponds with the results of previous studies in ACL-injured patients who reported an AUC ranging from 0.79 to 0.81 (Table 4).10,27
The MCID is a value that indicates whether the patient perceives a given change in a PRO measure to be clinically significant. 5 Various analytic methods have been used to calculate the MCID, which can be categorized as anchor-based or distribution-based.9,18,20 In the present study, an anchor-based approach was applied. Using the Youden index, the MCID of the Thai IKDC-SKF in patients undergoing primary ACLR was 15.5. This value was larger than the MDC; thus, this change was considered a true health change. Previous studies reported that MCID values for the IKDC-SKF in patients undergoing ACLR ranged2,10,27 from 10.7 to 18.9. There are some factors that can influence the variability of the MCID scores for any PRO measures.9,31 Franceschini et al 9 demonstrated that using 17 MCID calculation methods for the IKDC-SKF in a database of 312 patients with knee osteoarthritis who were treated with intra-articular platelet-rich plasma injection could lead to highly heterogeneous values ranging from 1.8 to 25.9. Moreover, patients’ characteristics—including age, disease group, disease severity, type of treatment, and follow-up period—can also influence the MCID score.26,31
When using the IKDC-SKF to evaluate treatment results in patients with ACL injury, the treatment is considered effective if the change scores are higher than the MCID. Another parameter that can be used to determine meaningful clinical improvement is the Patient Acceptable Symptom State (PASS). The PASS is the level of the PRO score in which patients report satisfaction with their symptoms. 28 Piamthipmanas et al 22 reported the PASS cutoff for the Thai IKDC-SKF among patients who underwent primary ACLR to be 74.2 (sensitivity, 0.72; specificity, 0.82). It was reported that a higher baseline score was positively associated with the achievement of the PASS but inversely associated with the achievement of the MCID. 23 Therefore, using both the MCID and the PASS would improve the interpretation of the IKDC-SKF for assessing the treatment results.
Limitations
This study has some limitations that should be mentioned. First, the vast majority of patients in this study were men. Barenius et al 1 reported male sex as a significant positive predictor of functional recovery after ACLR. Second, using the 7-level GRoC scale as 1 anchor question to calculate the MCID may not comprehensively capture all aspects of the change in a patient’s condition after ACLR. In addition, recall bias should be considered when using an anchor question to compare the 6-month postoperative health status with the baseline.
Conclusion
This study confirmed the responsiveness of the Thai IKDC-SKF for detecting a clinical change in ACL-injured patients after ACLR. The identified MCID of 15.5 can be used to evaluate significant clinical change and sample size calculations in future studies.
Footnotes
Acknowledgements
The authors gratefully acknowledge the patients who generously agreed to participate in this study and Suchitphon Chanchoo and Narumol Sudjai for their assistance with data collection and statistical analysis.
Final revision submitted May 14, 2023; accepted June 2, 2023.
The authors have declared no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Siriraj Hospital (ref No. Si 398/2020).