
Abstract
Background:
Degenerative tendon changes are common as people age, which can increase the likelihood of tendinous injuries. The outcomes of repairing hamstring tendon avulsions in patients >40 years after a rehabilitation protocol without postoperative bracing are relatively unknown.
Purpose:
To assess the functional outcomes of patients >40 years and determine the rerupture rate after surgical repair of complete proximal hamstring tendon avulsions while following a nonbracing rehabilitation protocol.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 27 patients >40 years with acute, complete proximal hamstring avulsions underwent surgical repair between 2012 and 2022 and completed follow-up assessments. Postoperative patient-reported outcome measures (PROMs) included the Single Assessment Numeric Evaluation (SANE), Physical (PCS) and Mental (MCS) Short Form 12 (SF-12), Marx Activity Rating Scale (Marx), Lower Extremity Functional Score (LEFS), Perth Hamstring Assessment Tool (PHAT), patient satisfaction (0-10 scale), and return to sports (RTS). Surgical repair integrity was assessed with physical and ultrasound examinations.
Results:
A total of 27 patients—including 10 men and 17 women—and 28 hips—including 10 right-leg and 18 left-leg hamstring avulsions—were included in this study. The mean age was 55.9 ± 8.3 years, and the mean body mass index was 27.1 ± 6.5 kg/m2 at the time of surgery. All 28 injuries were complete avulsions involving 3 hamstring tendons. The mean time from injury to surgery was 17.9 ± 12.4 days; 25 avulsions were repaired early (time to surgery <6 weeks), and 3 hamstrings were repaired delayed (6 to 8 weeks). All 28 avulsions were retracted at a mean distance of 4.9 ± 2.9 cm from the ischial tuberosity. The mean follow-up time was 67 ± 28.5 months. The mean follow-up PROMs included a SANE of 85.9 ± 18.1, SF-12 PCS of 49 ± 8.3, and SF-12 MCS of 54.7 ± 7.1, Marx of 6.3 ± 5.6, LEFS of 69.9 ± 12.7 (completed for 27 hips), PHAT of 82.1 ± 16.3 (completed for 26 hips), patient satisfaction of 9.1 ± 2, and 22 patients returned to sports (78.6%). At the last follow-up, all tendon repairs appeared intact and reinserted at the ischial tuberosity after ultrasound and physical examinations, and there were no signs of rerupture.
Conclusion:
Surgical repair of complete proximal hamstring tendon avulsions with a nonbracing rehabilitation protocol for patients >40 years demonstrated intact repairs with no reruptures. Some patients reported pain during follow-up functional testing, but the overall results highlighted positive functional and patient-reported outcomes, high levels of satisfaction, and a high RTS rate.
Keywords
Sports participation can offer a variety of mental, physical, and psychosocial benefits that increase overall quality of life.16,17,27 Participation in sports also presents the risk of injury, with hamstring injuries constituting between 12% and 29% of all injuries to athletes. 18 Although hamstring injuries also occur in other nonsporting settings, such as during slips, falls, and traffic accidents, there is a lack of reported incidence rates of nonsporting-related hamstring injuries. 24 Among hamstring injuries, avulsions of the proximal hamstring tendons from the ischial tuberosity are rare and occur in the context of “forceful eccentric muscle contraction or excessive passive lengthening”4,8 as a result of hip hyperflexion and knee hyperextension.4,8,14,30 Proximal hamstring tendon avulsions have also been shown to occur as a result of significant hip abduction. 36
With regard to the management of proximal hamstring tendon avulsion injuries, nonoperative treatment options with positive outcomes have been reported. 37 However, because of the debilitating nature of proximal hamstring tendon avulsion injuries, surgical intervention has been recommended for complete tendon avulsions in active populations, avulsions involving ≥2 hamstring tendons, and acute avulsions with retraction lengths of >2 cm. 5 Surgical repair of proximal hamstring tendon avulsions has demonstrated superior functional outcomes, return to sports (RTS) rates, and patient satisfaction compared with nonoperative treatment options.2,7,10,21,32,33 While several studies have demonstrated positive outcomes of surgically repaired proximal hamstring tendon avulsions, there is a paucity of information on surgical intervention, specifically in populations >40 years while following a nonbracing rehabilitation protocol. This is notable because there remains no current consensus regarding the need for postoperative bracing after proximal hamstring avulsion repair.
Some studies have described rehabilitation programs—including postoperative bracing1,11,13—whereas some recent studies have demonstrated that postoperative bracing immobilization is unnecessary, uncomfortable, and may still lead to unwanted hamstring muscle activation, which could hinder healing and functional outcomes.3,25,26 It is also important to study how populations respond to proximal hamstring avulsion repair as degenerative tendon changes are common in those >35 years, 41 which can increase the likelihood of tendinous injuries. This study aimed to assess the functional outcomes and rerupture rates of patients >40 years after surgical repair of acute, complete proximal hamstring tendon avulsions while following a nonbracing rehabilitation protocol.
Methods
Study Design and Patient Selection
This retrospective study was approved by an institutional review board, and written informed consent was obtained from all participating patients before enrollment. Medical records between December 2012 and November 2022 were reviewed to identify patients with surgically repaired complete proximal hamstring tendon avulsions who were aged >40 years at the time of surgery. All identified patients were invited for a one-time follow-up assessment. All one-time follow-up assessments were performed between September 2023 and September 2024. Patient study participation was based on the following inclusion criteria: confirmation on magnetic resonance imaging (MRI) of complete avulsions of all hamstring tendons at the proximal insertion site on the ischial tuberosity, age >40 years at the time of surgery, and surgical repair of the proximal hamstring tendons. The exclusion criteria included patients with partial hamstring avulsions and patients unwilling or unable to complete a follow-up assessment. A total of 27 patients (28 proximal hamstring repairs) were included in this study. All surgical procedures were performed by 3 board-certified orthopaedic sports medicine surgeons (J.E.Z., K.S.H., J.W.U.) at 1 surgical center.
Surgical Technique
After the administration of general anesthesia, patients were placed in the prone position. The buttocks and thigh regions were prepared and draped in a sterile fashion. Either a transverse gluteal incision or a longitudinal incision was made through the gluteal fascia, and great care was taken to prevent injury to cutaneous nerves. The gluteus maximus was retracted proximally, and the hamstring tendon sheath was opened longitudinally. The sciatic nerve was identified and retracted during the surgical intervention. A sciatic nerve neurolysis was performed in the event of sciatic nerve scarring. The serosanguineous fluid in the hamstring sheath was evacuated if present. The hamstring tendons were mobilized, brought through the incision, and debrided to healthy-appearing tissue edges. The ischial tuberosity was prepared with curettes to punctuate bleeding bone. Two suture anchors were placed in the ischial tuberosity. Each anchor had 2 sets of sutures with 2 needle limbs each for a total of 4 limbs: for each suture, 1 limb was passed through the avulsed hamstring tendon with a modified Krackow locking stitch while the second limb of each suture was utilized in a single through-and-through stitch to allow the reduction of the tendon back to the normal anatomic position on the ischial tuberosity. After tensioning, sutures were tied, and the edges were oversewn with nonabsorbable sutures in an interrupted fashion to aid in repair. The incision was then irrigated, and the tendon sheath was closed with absorbable sutures. The wound was reirrigated, and the skin was closed with absorbable sutures.
Postoperative Rehabilitation Protocol
None of the patients used a brace after surgery and were instructed to ambulate with flat-foot weightbearing on crutches for 6 weeks as soon as the symptoms allowed, switching from a stiff-leg gait to a body-neutral “wedding march” manner. Patients were instructed to avoid isolated isotonic and end range isometric hamstring stretching during this time. Patients performed a 7-phase rehabilitation protocol as follows:
Phase 1, days 1 to 14: Perform home exercises only; maintain flat-foot weightbearing.
Phase 2, weeks 2 to 4: Start formal physical therapy; maintain flat-foot weightbearing; and initiate quad sets and straight leg raises.
Phase 3, weeks 4 to 6: Begin progressing weightbearing to a normal gait.
Phase 4, weeks 6 to 8: Perform end range isometric hamstring stretching exercises; progress full lower extremity stretching program; and complete proprioceptive activities.
Phase 5, weeks 8 to 12: Perform hamstring and quad strengthening exercises.
Phase 6, weeks 12 to 16: Progress to plyometric activities; complete sport-specific exercises.
Phase 7, weeks 16 to 20: RTS/activity.
Study Variables and Outcomes
Patient Characteristics
Patient characteristics included sex, laterality, injury diagnosis type (acute or chronic), age at the time of surgery, body mass index (BMI) at the time of surgery, and sport-related injury type.
Surgical Details
Surgical and intraoperative details were as follows: time from injury to surgery; surgical intervention acuity (time from injury to surgery: <6 weeks was defined as early, 6-8 weeks as delayed, and >8 weeks as late); retraction amount (cm); surgical incision type (transverse or longitudinal); estimated blood loss (mL); number of tendons involved; whether sciatic neurolysis was performed; surgical and postoperative complications; and the presence of postoperative sitting pain. The time from surgery to the follow-up assessment was reported.
Physical Examination
The physical examinations were performed by a fellowship-trained orthopaedic sports medicine surgeon (LAV) or a fellowship-trained primary care sports medicine physician (M.Y.). Palpation over the ischial tuberosity was performed with patients in the prone position to assess pain and integrity of the surgical repair. Passive hip range of motion was assessed for hip flexion, abduction, adduction, and extension. Passive hip flexion was assessed with patients in the supine position while their hips and knees were flexed toward their chests. Passive hip flexion between 110° and 120° was defined as normal. Passive hip abduction and adduction were assessed with patients in the supine position while their hips and knees were placed in 90° of flexion. Passive hip abduction between 30° and 50° and passive hip adduction between 20° and 30° were considered normal. Passive hip extension was assessed with patients in the lateral decubitus position. Full passive hip extension between 10° and 15° was considered normal. The number of patients achieving normal range of motion for hip flexion, abduction, adduction, and extension was reported.
Hamstring muscle eccentric strength was assessed with patients in the kneeling position with an upright body posture, hips in the neutral position, and knees placed in 90° of flexion. Testers applied a stabilizing force by pushing down on the back of the lower legs as patients were instructed to eccentrically lower their trunks toward the ground as far as possible while maintaining an upright posture and hips in the neutral position. Patients were allowed to catch themselves as they eccentrically lowered toward the ground. Hamstring muscle concentric strength was assessed in the prone position with the knee placed in 15° of flexion. Testers applied a pull force to the back of the leg, and patients were instructed to contract against the applied force. Muscle strength was assessed using the Medical Research Council Manual Testing scale (0-5 scale) 29 used with permission of the Medical Research Council (https://www.nationalarchives.gov.uk/doc/open-government-licence/version/2/), and associated pain was recorded.
The Puranen-Orava test, bent-knee stretch test, fast hamstring-stretch test, standing hamstring drag test, and take-off-the-shoe test (TOST) were performed to assess the presence of hamstring tendinopathy with posterior thigh pain, indicating a positive result.1,12,15,23,31 Load assessments were performed with the single-leg bent-knee bridge (low load), long-lever bridge (moderate load), and arabesque (high load), with associated pain recorded. 19 Patient gaits were evaluated, and the presence of “stiff-legged” gaits to avoid hip flexion and knee extension and subsequent hamstring muscle activation were recorded. 1
Ultrasound Examination
The ultrasound examinations were performed by a fellowship-trained orthopaedic sports medicine surgeon (LAV) or a fellowship-trained primary care sports medicine physician (M.Y.). An ultrasound evaluation was performed at the last follow-up using a 12-mHz linear array transducer to assess the integrity of the repaired hamstring tendon insertion at the ischial tuberosity, the musculotendinous junction of the semimembranosus, the conjoint tendon, and the sciatic nerve, and any signs of rerupture were recorded.
Patient-Reported Outcome Measures
Patient-reported outcome measures (PROMs) included the Single Assessment Numeric Evaluation (SANE) (0-100 scale), 40 Physical (PCS) and Mental (MCS) Short Form 12 (SF-12) Version 1.0 components, 39 Marx Activity Rating Scale (Marx) (0-16 scale), 28 Lower Extremity Functional Score (LEFS) (0-80 scale), 6 Perth Hamstring Assessment Tool (PHAT) (0-100 scale), 9 patient satisfaction (0-10 scale), and RTS.
Statistical Analysis
Outcome measures were presented as either summations of categorical values or numerical values with means and associated standard deviations. All analyses were performed using Microsoft Excel (Microsoft Corp).
Results
Patient Characteristics
The 27-patient cohort included 10 men and 17 women. One male patient underwent separate repairs of both proximal hamstrings, resulting in 28 repairs being included in this study, with 10 right-leg hamstring avulsions and 18 left-leg hamstring avulsions. All injuries were acutely diagnosed. The mean age at the time of surgery was 55.9 ± 8.3 years, and the mean BMI was 27.1 ± 6.5 kg/m2. Also, 17 avulsions resulted from sports-related activities: 5 from waterskiing, 3 from tennis, 2 from racquetball, 2 from running, 1 from football, 1 from cycling, 1 from bowling, 1 from rollerblading, and 1 from ballroom dancing. All other injuries were from slips and falls. A summary of patient characteristics is detailed in Table 1.
Patient Characteristics a

Data are presented as mean + SD or n. BMI, body mass index.
Surgical & Intraoperative Details
The mean time from injury to surgery was 17.9 ± 12.4 days; 25 avulsions were repaired early, 3 hamstrings were repaired delayed, and 0 hamstrings were repaired at a late stage. All avulsed hamstring tendons were retracted at a mean distance of 4.9 ± 2.9 cm from the insertion point on the ischial tuberosity. Surgical incision types included 24 transverse incisions and 4 longitudinal incisions, the mean estimated blood loss was 13 ± 20.7 mL, and all 28 injuries were complete avulsions involving all 3 hamstring tendons. Sciatic neurolysis was performed in 2 hamstring repairs. There were no intraoperative complications. One patient developed a deep vein thrombosis and pulmonary embolism (DVT/PE) after surgery, which were successfully treated by a hematologist with oral anticoagulants for 6 months. Two patients experienced postoperative sitting pain after repair. Surgical and intraoperative details are summarized in Table 2.
Surgical and Intraoperative Details a

Data are presented as mean ± SD or n.
Follow-up Assessment
The mean follow-up time was 67 ± 28.5 months. Palpation of the ischial tuberosity revealed an intact tendon in all repairs, with 3 patients reporting pain. Normal passive hip flexion (between 110° and 120°) was observed in 27 hips, with 2 patients experiencing pain. Normal passive hip abduction (between 30° and 50°) was observed in 28 hips, with 2 patients experiencing pain. Normal passive hip adduction (between 20° and 30°) was observed in 28 hips, with no patients experiencing pain. Normal passive hip extension (between 10° and 15°) was observed in 27 hips, with 3 patients experiencing pain. The mean eccentric strength was 4.8 ± 0.4, with 2 patients experiencing pain, and the mean concentric strength was 4.8 ± 0.4, with 2 patients experiencing pain. There were 2 positive Puranen-Orava tests, 2 positive bent-knee stretch tests, 3 positive fast hamstring-stretch tests, 1 positive standing hamstring drag test, and no positive TOSTs. Two patients reported pain during a single-leg bent-knee bridge, 2 patients during a long-lever bridge, and 4 patients during an arabesque. The presence of a “stiff-legged” gait was observed in 1 patient. Across all functional testing assessments, 8 patients reported some level of pain during at least 1 assessment, while 20 patients did not report experiencing pain during any assessment. Upon ultrasound examination, all surgically repaired hamstring tendons appeared intact and inserted at the ischial tuberosity, and there were no signs of rerupture in any patients. A representative postoperative ultrasound completed in this study demonstrating successful healing with an intact repair can be seen in Figure 1.
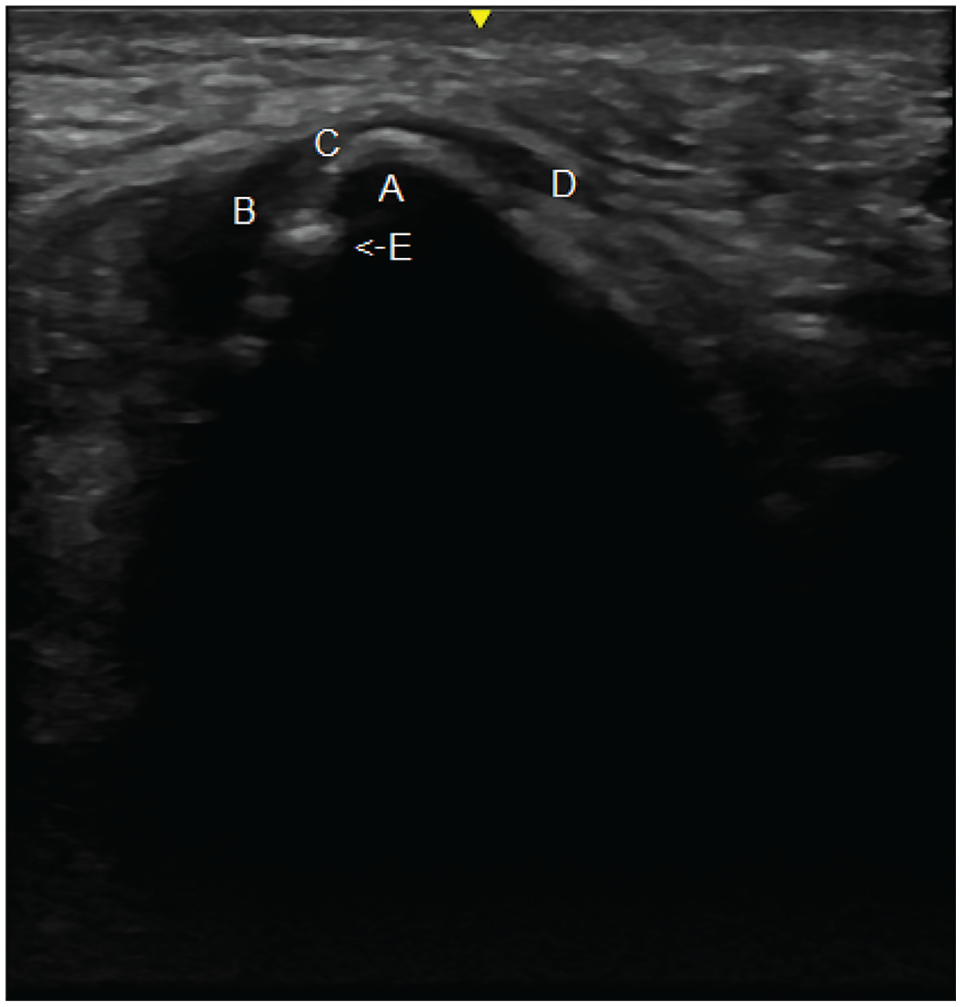
Proximal hamstring avulsion repair ultrasound. (A) Ischial tuberosity. (B) Semimembranosus tendon. (C) Conjoint tendon. (D) Adductor magnus tendon. (E) Inserted surgical anchor.
The mean follow-up PROMs are as follows: SANE: 85.9 ± 18.1; SF-12 PCS: 49 ± 8.3; SF-12 MCS: 54.7 ± 7.1; Marx: 6.3 ± 5.6; LEFS: 69.9 ± 12.7 (complete for 27 hips); PHAT: 82.1 ± 16.3 (completed for 26 hips); patient satisfaction: 9.1 ± 2; and 22 repairs resulted in RTS (78.6%). A summary of PROMs is listed in Table 3.
Postoperative PROMs a

Data are presented as mean ± SD or n (%). LEFS, lower extremity functional score; Marx, Marx Activity Rating Scale; MCS, mental component score; PCS, physical component score; PHAT, Perth Hamstring Assessment Tool; PROMs, patient-reported outcomes measures; RTS, return to sports; SANE, Single Assessment Numeric Evaluation; SF-12, 12-item Short Form Survey.
Discussion
This study aimed to assess the functional outcomes and the rerupture rate in patients >40 years after surgical repair of complete proximal hamstring tendon avulsions with a nonbracing rehabilitation protocol. In this 27-patient and 28 hamstring study, with a mean follow-up of 67 ± 28.5 months, high levels of postoperative function were observed as 27 (96.4%) hips demonstrated normal range of motion, 21 (75%) hamstrings displayed both 5/5 eccentric and concentric muscle strength, and 24 (85.7%) hips were able to successfully bear a high load (arabesque) without pain. In addition, patients reported lower extremity and hamstring-specific PROM mean scores of 69.9 ± 12.7 (out of 80) on the LEFS and 82.1 ± 16.3 (out of 100) on the PHAT. However, 4 (14.3%) hips tested positive for signs of hamstring tendinopathy, 1 (3.6%) hip displayed a “stiff-legged” gait, 2 (7.1%) patients reported experiencing postoperative sitting pain, and 8 (28.6%) patients reported some form of pain during extensive functional testing at the last follow-up. Surgery was well tolerated, with 24 patients reporting being “very satisfied” with their surgical procedures (85.7%).
The study population was active, with 17 (60.7%) injuries occurring during sports participation, and patients returning to sports participation after 22 repairs (78.6%). Seven patients reported a Marx score of 0, as these patients perform “running, “cutting, “deceleration,” and “pivoting” movements “less than one time a month” as part of their postoperative exercise routine. The surgical repairs were all found to be stable and intact, and there were no signs of reruptures upon physical and ultrasound examinations. Coupled with only 1 (3.6%) postoperative complication and no reoperations, this >40-year-old population experienced durable and long-lasting surgical repairs. Consequently, the results of this study support the conclusion that patients >40 years at the time of surgery respond well to surgical repair of complete proximal hamstring tendon avulsions while following a nonbracing rehabilitation protocol, as most patients in this study were able to return to active and healthy lifestyles without the occurrence of reruptures.
In a 2022 systematic review of surgically managed proximal hamstring avulsions, Hillier-Smith et al 20 included 1530 surgical repairs across 35 studies with a mean age at the time of surgery of 44.7 years (range, 12-78 years) and described a mean LEFS of 74.7 ± 1.7, a mean satisfaction rate of 92.6%, and an RTS at any level of 84.5% among all repairs, and a mean LEFS of 73.3 ± 1, a mean satisfaction rate of 94.1%, and an RTS rate of 85.7% among surgically repaired complete avulsions. In a similar proximal hamstring avulsion systematic review, Bodendorfer et al 10 included 767 surgical repairs across 23 studies, with a mean age of 41.4 years at the time of surgery and reported a mean LEFS of 72.77 ± 6.55, a mean satisfaction rate of 90.81 ± 9.72%, and an RTS rate of 79.75% among all repairs, and a mean satisfaction rate of 89.64 ± 9.72% and an RTS rate of 81.43% among surgically repaired complete avulsions. The results of our surgically repaired complete avulsion study compare similarly, with a mean LEFS of 69.9 ± 12.7, a mean satisfaction of 9.1 ± 2 (out of 10), and an RTS rate of 78.6%. However, the mean age at the time of surgery in our study was 55.9 ± 8.3 years, and all patients were >40 years at the time of surgery. The results of our study are also similarly favorable compared with a study of nonbraced proximal hamstring avulsion repairs in which Lazaro and Banffy 25 reported excellent subjective and functional hip outcomes, a high RTS rate, and a low failure and revision rate. In terms of complications, Bodendorfer et al 10 reported that, among surgically repaired complete avulsions, 29.38% of patients developed complications, with 0.63% experiencing a DVT/PE and 2.50% experiencing a rerupture. Our complication rate compares favorably, with just 1 repair (3.6%) experiencing a DVT/PE as the only complication and no reruptures occurring at a mean follow-up time of 67 months. The Bodendorfer et al 10 systematic review also reported a postoperative sitting pain rate of 7.05% among all repairs and 9.38% among repairs of complete avulsions. 10 In our study, 2 (7.1%) patients experienced postoperative sitting pain. The present study also expands the scope of assessing proximal hamstring surgical repair healing by providing novel ultrasound evidence of successful healing and intact repairs in all patients.
In the process of comparing our findings to systematic reviews of proximal hamstring tendon avulsion repairs, we observed a lack of studies specifically following nonbracing rehabilitation protocols for the repair of acute, complete avulsions with age minimums and mean ages at the time of surgery as high as this study.10,20,22,38 Given the paucity of the data in the published literature, our homogeneous cohort of 28 acute, complete proximal tendon hamstring avulsions can provide further evidence for the safety and efficacy of postoperative rehabilitation without a brace. Moreover, as our study only included patients >40 years at the time of surgery and a mean age at the time of surgery of 55.9 ± 8.3 years, we were able to demonstrate positive outcomes for populations >40 years while following a nonbracing rehabilitation protocol.
Specifically, studying patients >40 years at the time of surgery is important, as degenerative changes in tendons have been shown to occur in people >35 years. 41 A normal healthy tendon “is a fibrous type of tissue with a highly organized type I collagen-based extracellular matrix (ECM), and a minimal number of cells and neurovascular structures.” 34 As tendons age, imbalanced turnover of the ECM caused by “insufficient synthesis and increased degradation” 41 has been proposed as a contributing factor for tendon degeneration.35,41 Given the possibility of tendon degeneration potentially affecting surgical repair and recovery, we hope to conduct future studies comparing the outcomes of proximal hamstring avulsion repair in younger and older patient populations. We hope that future proximal hamstring tendon avulsion repair studies will consider and evaluate the role of aging and potential tendon degeneration in repair and recovery.
Limitations
There were several limitations in this study. First, the patients in this study were identified retrospectively and assessed with a single prospective follow-up assessment. Without preoperative data, we had no comparison baseline for postoperative outcomes, and we were unable to quantify functional and patient-reported improvements after surgery. Future prospective studies can address this limitation with preoperatively collected data, allowing for the determination of patient improvement and quantification of the effect of surgery. This study was also a report of complete proximal hamstring avulsions that were surgically repaired. As a result, we lacked comparison groups to add statistical power to our findings. This limitation can be addressed by conducting larger multicohort studies—including comparison data from other similar cohorts to allow for a more complete evaluation of the effect of surgical repair in acute, complete proximal hamstring avulsions. This is especially important in patients with chronic injuries, as degenerative tendinous changes may also manifest themselves in chronic injuries. Another limitation of the study was the use of a subjective postoperative hamstring muscle strength assessment. In future studies, objective measures of hamstring muscle strength can add further clinical relevance to the results. Finally, in this study, tendon integrity was evaluated with ultrasound examination for efficiency and cost savings purposes. However, a follow-up MRI evaluation could increase the accuracy of the tendon integrity assessment.
Conclusion
Surgical repair of complete proximal hamstring tendon avulsions with a nonbracing rehabilitation protocol for patients >40 years demonstrated intact repairs with no reruptures in an active patient population. Some patients reported pain during follow-up functional testing, but the overall results demonstrated positive functional and patient-reported outcomes, high levels of patient satisfaction, and a high RTS rate.
Footnotes
Final revision submitted October 24, 2024; accepted November 14, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.E.Z. has received consulting fees from Arthrex, DePuy Synthes Products, Anika Therapeutics, and Arthrosurface; education payments from Southern Edge Orthopaedics and Zimmer Biomet Holdings; and holds current or prospective ownership or investment interest in Anika Therapeutics. T.P. has received a grant from Arthrex; hospitality payments from Coastal Medical Technologies, Zimmer Biomet Holdings, and Medical Device Business Services; and education payments from Smith & Nephew, Elite Orthopedics, Arthrex, and Southern Edge Orthopaedics. G.P.Y. has received consulting fees and royalties or a license from Arthrex. J.W.U. has received consulting fees and acquisitions from Anika Therapeutics; royalties or a license from Linvatec Corporation; acquisitions from MedShape Inc; and support for education from Zimmer Biomet Holdings. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Baptist Health South Florida (1229705-29).