
Abstract
Background:
Patella alta has been noted to be a risk factor for recurrent patellar instability.
Purpose:
We conducted a radiographic study to determine whether a patellar tendon imbrication technique normalizes patellar height as well as whether the shortened length is maintained at a minimum 2-year follow-up.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 54 consecutive patients were identified after a retrospective chart review was performed on patients who underwent patellar tendon imbrication between 2008 and 2013. Preoperative, 3 weeks postoperative, and minimum 2 years postoperative lateral radiographs were analyzed using Insall-Salvati (IS), Blackburne-Peel (BP), and Caton-Deschamps (CD) indices to determine the amount of shortening that was achieved after the procedure and to what degree that shortening was maintained at a minimum 2-year follow-up.
Results:
A total of 27 patients (32 knees) completed a minimum 2-year follow-up. The mean patellar tendon length preoperatively was 6.1 cm (range, 5-8 cm). At 3 weeks and 2 years, the mean tendon lengths were 5.1 and 5.2 cm, respectively. Thus, the mean ± SD change in patellar tendon length from preoperative to 3 weeks postoperative was 0.97 ± 0.67 cm. IS, BP, and CD ratios had minimal change (loss of correction) from 3-week to 2-year follow-up; the delta values were 0.04, –0.03, and 0.09, respectively. There were no complications directly related to the technique.
Conclusion:
Patellar tendon imbrication is a safe and effective procedure to correct patella alta in the setting of lateral patellar instability. On average, the technique allowed 1 cm of patellar tendon shortening and maintained the correction at a minimum 2-year follow-up. In the skeletally immature patient, this technique allows correction of patella alta by avoidance of a tibial tuberosity osteotomy.
Keywords
Recurrent dislocations of the patella are not uncommon. Fithian et al 12 demonstrated the incidence to be 30 to 43 per 100,000. Although the initial management of an acute patellar dislocation is typically nonoperative, the recurrence rate is reported to be 20% to 80%. 1,3,12,24
Numerous anatomic factors have been shown to contribute to patellar instability, including injury to the medial patellofemoral ligament (MPFL), trochlear dysplasia, increased tibial tuberosity–trochlear groove (TT-TG) distance, femoral and/or tibial rotational and/or angular malalignment, and patella alta. 9,10,13,14,16,22,29,35 Dejour et al 10 reported on radiographic findings that were associated with recurrent patellar dislocations and found that patella alta was 1 of the 4 most common associated pathoanatomic findings in patients experiencing recurrent dislocation of the patella, being present in nearly one-quarter of patients with patellar instability but in only 3% of controls. Additionally, patella alta has been noted to be a risk factor for recurrent patellar instability in patients treated with nonoperative treatment or isolated MPFL reconstruction. 19,33
The explanation for this association is found by understanding the kinematics of the extensor mechanism of the knee in addition to the anatomic factors that support patellar stability. 20,30,31,35 As the knee flexes, the MPFL assists in guiding the patella into the trochlear groove. Once engaged within the trochlea, the slope of the lateral wall of the trochlea becomes the primary restraint to lateral displacement. Normally, this engagement occurs at about 15° of knee flexion; in the state of patella alta, this engagement is delayed into deeper knee flexion. During a patellar dislocation, the MPFL is disrupted and may subsequently heal with increased laxity. The combination of an incompetent MPFL and the delayed engagement into the trochlea provides the vulnerability to redislocation.
Traditionally, the treatment of patella alta has included a distalization osteotomy of the tibial tuberosity. 21 Although this is effective, it cannot be performed in skeletally immature patients because of the open tibial tuberosity apophysis. Moreover, distalization of the tibial tuberosity can be complicated by delayed union and nonunion as well as hardware irritation or failure. In 2007, a novel surgical technique of patellar tendon imbrication was described. 2 Although the technique has been reported, it has not been radiographically reviewed to assess its ability to restore normal patellar height indices. The purpose of this radiographic study is to determine whether (1) the patellar tendon imbrication technique normalizes patellar height, (2) correction is maintained at a minimum 2-year follow-up, (3) the intended amount of patellar tendon shortening is the actual amount of shortening achieved, and (4) complications are associated with this procedure. Our hypothesis was that the surgical technique for patellar tendon imbrication would normalize patellar height and that the correction would be maintained at a minimum of 2 years postoperatively.
Methods
Patient Population
The patients for this study were identified from the senior author’s (J.A.’s) surgical database. The inclusion criteria for the study were (1) patients who underwent a patellar tendon imbrication procedure performed by the senior author between 2008 and 2013 with a minimum 2-year follow-up, (2) patients who had an established diagnosis of patella alta as defined by an abnormal patellar height index determined on a lateral radiograph, and (3) patients who had recurrent lateral patellar instability. The only exclusion criterion was that we eliminated the first 10 patients. We did not exclude patients with other associated pathoanatomic conditions such as trochlear dysplasia and elevated TT-TG distance because we were trying to strictly analyze the patellar tendon imbrication technique and not the clinical outcomes related to instability. We eliminated the first 10 patients because neither the developing surgical technique nor the developing postoperative rehabilitation regimen was uniform. Because some of the initial patients lost correction due to early weightbearing and lack of bracing, we adjusted portions of the technique and addressed the need for postoperative bracing and nonweightbearing. The remaining patients in our cohort benefited from the uniform surgical technique and postoperative protocol subsequently described in this paper. All the patients in the study group who were adults at the time of surgery were able to provide informed consent before being entered into the study. Minor patients had their legal representative provide informed consent. The study protocol and processes were reviewed and approved by our institutional review board.
Each patient’s medical record was reviewed, and data regarding age, sex, date of surgery, time of final follow-up, and complications were recorded. The primary goal of this study was to evaluate whether radiographic indices of patella alta were normalized. The intended amount of patellar tendon shortening was extracted from operative reports, and clinical notes were reviewed for complications. Lateral patellar instability was confirmed with a documented history of at least 1 lateral patellar dislocation. We did not collect patient-reported outcomes because of the many confounding variables of chondrosis, pathoanatomic conditions, and associated surgical techniques within the cohort that would affect outcomes. We were strictly focused on the patellar tendon imbrication component of the surgery. All patients had undergone a supervised physical therapy regimen for pelvifemoral rehabilitation before surgical consideration.
Radiographic Analysis
A musculoskeletal radiologist (J.P.) was blinded to the amount of imbrication performed at surgery. The inter- and intraobserver reliability for measurement of patellar height indices has been validated previously. 34 The following radiograph time points were analyzed: preoperative, 3 weeks postoperative, and a minimum 2 years postoperative.
We used 3 height indices: Insall-Salvati (IS), Blackburne-Peel (BP), and Caton-Deschamps (CD). Using these indices allowed for an objective measurement of patella alta as defined by an IS ratio >1.2, a BP index >1.0, or a CD index >1.3. 6,8,17,34
Surgical Technique
The surgical technique (Figure 1) was developed by the senior author and has previously been described. 2 The amount of shortening was determined by creating a patellar tendon length that would normalize the preferred patellar height index (ie, the IS index). Our intent was to obtain an IS ratio of 1.0.

Stepwise surgical technique for patellar tendon imbrication procedure. See text for details. Adapted from Andrish. 2 Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography © 2007-2019. All rights reserved.
Step 1: The amount of shortening of the patellar tendon is determined preoperatively through radiographic measurements and then outlined with a marking pen (a). A third line is made proximal to the level of dissection that is one-half the distance of the shortening (b = 1/2a).
Step 2: From the distal marking, a flap of tendon, the anterior half, is elevated by sharp dissection using a fresh No. 15 blade proximal to the predetermined level. It is important to stay uniform in thickness throughout the area of dissection.
Step 3: The first row of No. 1 absorbable sutures is placed and left untied by entering at the proximal marking of (b), passing deep to the tendon, and emerging at the middle of the intact posterior section of tendon. A locking stitch is made and the suture returned to the proximal marking. These sutures do not perform the shortening; rather, they secure the redundant flap created on the posterior side of the tendon after imbrication.
Step 4: Starting at the apex (proximal) of the flap created in step 2 and ending at the distal portion of where the flap originated, locking stitches are placed that will perform the imbrication. It is important to stay anterior to the posterior half of the dissected tendon. Specifically, using No. 2 FiberWire (Arthrex), 3 horizontal sutures with a locking stitch component distally are placed that will create and maintain the imbrication.
Step 5: The FiberWire sutures are tied. It is sometimes helpful to manually distract the patella distally, as the sutures are tied to accommodate the imbrication.
Step 6: The previously placed (step 3) but not tied absorbable sutures are tied, thus imbricating the redundant posterior section of tendon. In a pants-over-vest fashion, the distal end of the anterior section of isolated tendon is then repaired with No. 0 absorbable suture.
Step 7: The knee is flexed to 90° to assess competence of the suture lines as well as the possible need for quadriceps lengthening, which may be required to enable 90° of flexion when treating severe patella alta or fixed congenital lateral patellar dislocation. Typically, full flexion is ultimately obtained after rehabilitation.
Postoperative Protocol
The initial protection phase of the recovery is maintained with a motion-control brace and 6 weeks of touchdown nonweightbearing. By 6 weeks postoperatively, progressive weightbearing is allowed as tolerated with eventual weaning from crutches by 8 to 12 weeks.
Motion is gradually increased postoperatively. From 0 to 2 weeks, 0° to 30° of passive, active-assisted flexion and then active flexion are allowed. By 2 to 3 weeks postoperatively, the amount of allowable flexion is increased by 10° to 20° per week; the brace is discontinued by 6 weeks. If full weightbearing is necessary during this period, the brace can be locked in 0° of extension for ambulation and released when nonambulating. At 3 weeks, the brace can be removed for heel-slide range of motion exercises as tolerated, but otherwise, patients remain in the brace for ambulating and sleeping.
Hourly repetitions of quadriceps isometric exercises are encouraged immediately after surgery, along with the principles of “pelvifemoral” conditioning and core stability. Typically, closed-kinetic chain resistance training can be added by 6 weeks. Progressive weightbearing and weaning from crutches are initiated at 6 weeks. Open-kinetic chain resistance training is limited until week 16. Return to sport or full activity typically occurs around the 6- to 12-month mark but is dependent upon many variables, such as age, expectations, and the elimination of significant strength deficits.
Results
From a review of the aforementioned database, we identified 54 consecutive individuals who met the inclusion criteria and were treated operatively by the senior author. These 54 individuals had 61 knee surgeries; of these, 27 patients (32 knees) had a radiographic and clinical evaluation at a minimum 2-year follow-up. Although a few of our patients with severe patella alta required an associated quadriceps lengthening, none were involved in the cohort being studied. The mean follow-up was 4.1 years (range, 2-8.25 years).
The participants included 14 male and 13 female patients: The patients’ mean age at the time of surgery was 19.8 years (range, 12-35 years). In total, 11 patients were skeletally immature. The patellar height indices were obtained from a single nonweightbearing lateral radiograph of the knee at 30° of flexion.
The mean patellar tendon length preoperatively was 6.1 cm (range, 5.0-8.0 cm). At 3 weeks and minimum 2 years, the mean tendon length was 5.1 cm (range, 3.4-8.0 cm) and 5.2 cm (range, 3.7-7.1 cm), respectively.
On average, the planned or perceived amount of patellar tendon shortening was 1.8 cm (range, 1-3 cm). However, the actual mean ± SD change in patellar tendon length from preoperative to 3 weeks immediately postoperative was 0.97 ± 0.67 cm. The mean change in patellar tendon length from preoperative to final evaluation was 0.86 ± 0.69 cm. Although the actual amount of shortening was only 54% of the planned amount, this was not a consistent finding. Twenty of our patients remained classified as alta with an IS index >1.2. The imbrication does result in thickening of the tendon, which can be noticeable when the knee is in flexion.
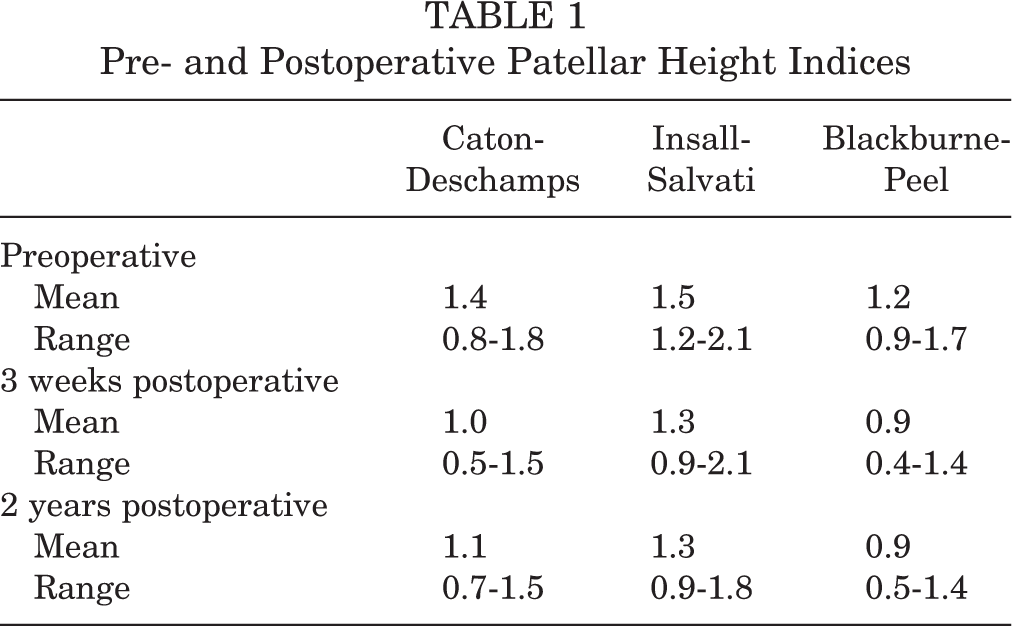
Pre- and postoperative patellar height indices are listed in Table 1. The mean CD ratio changed by 0.04 ± 0.20 from 3-week to 2-year follow-up; the changes for the IS and BP ratios were –0.03 ± 0.17 and 0.09 ± 0.29, respectively.
Pre- and Postoperative Patellar Height Indices
There were 8 complications (Table 2). Two (2/32; 6%) of these 8 complications led to failure of the imbrication and loss of correction. Both patients underwent a successful revision patellar tendon imbrication procedure, and the measurements included in this study were obtained after the revisions. Both patients were skeletally mature. The first complication was secondary to noncompliance as a patient removed his hinged knee brace by 3 weeks after surgery and was fully weightbearing. The second complication was secondary to multiple injuries as this patient fell down stairs multiple times during the initial 4 weeks after surgery (secondary to spontaneous patellar dislocations of his contralateral knee).
Complications a
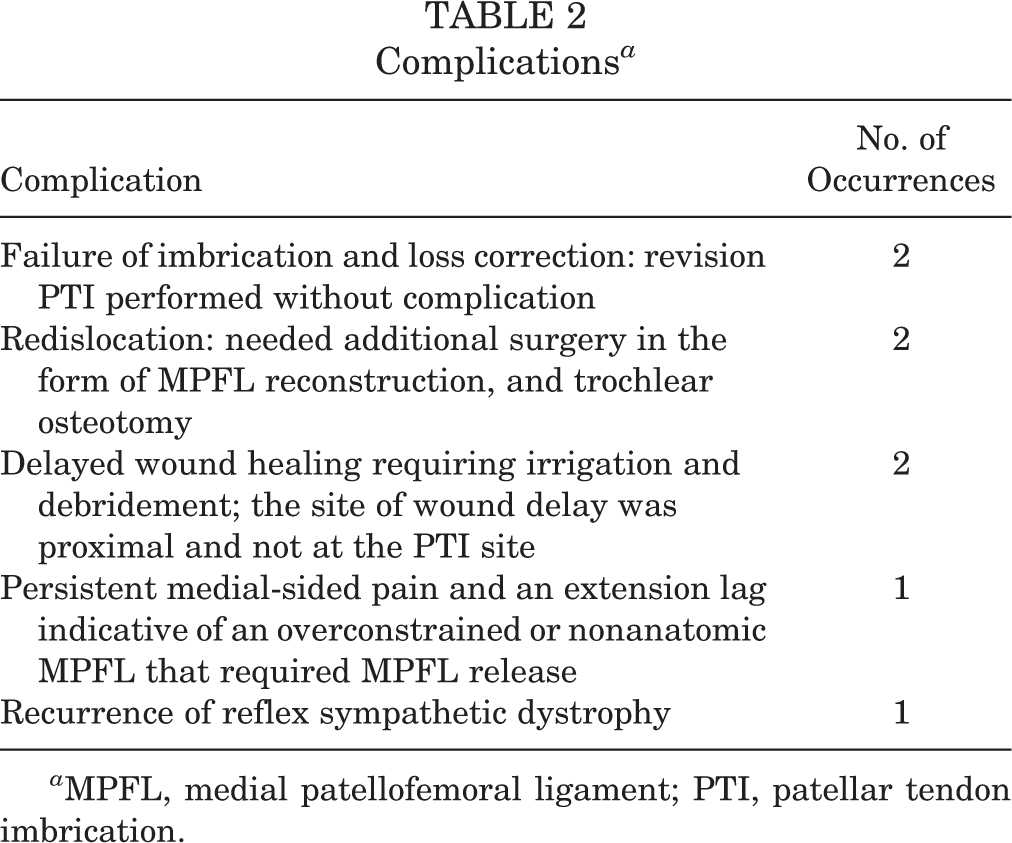
a MPFL, medial patellofemoral ligament; PTI, patellar tendon imbrication.
Discussion
The rate of patellar dislocation is estimated to be highest in the age group of 10 to 17 years, with reported rates of 29% to 43%. 3,12,24 Given the high proportion of patellar instability cases in skeletally immature patients and the common association with patella alta, the patellar imbrication technique was initially devised to address this condition in skeletally immature patients. Over time, however, the senior author extended the use of this technique to adults. The most important finding in this radiographic study is that patellar tendon imbrication can safely shorten the tendon and maintain the results at a minimum of 2-year follow-up.
Although this technique was initially described in 2007, 2 to our knowledge, this is the first clinical review of the patellar tendon imbrication technique for the management of patients with recurrent patellar dislocations. In 2014, Servien and Archbold 27 referred to our surgical technique for patellar tendon shortening. This group has also reported additional procedures to address patella alta including a patellar tendon tenodesis in conjunction with a distalization tibial tubercle osteotomy. 21 The normal range of patellar tendon length is 40 to 50 mm. 11,15,18,22,25,26,36 In our study, the mean preoperative length was 61 mm, and in the study by Mayer et al, 21 the mean preoperative patellar length was 56 mm. Neyret et al 22 hypothesized that an abnormally long patellar tendon may increase coronal plane mobility of the patella. Furthermore, increased patellar mobility of only 4 mm has been associated with subjective feelings of patellar instability. 32 Finally, although patella alta can lead to recurrent patellar instability despite MPFL repair or reconstruction, a long patellar tendon has also been associated with amplification of the effects of MPFL insufficiency. 25 Further kinematic research involving long patellar tendon lengths and patellar instability is needed, as our colleagues managing cerebral palsy have noted that patellar tendon shortening can improve extensor lag and flexed knee gait. 7,37
In the current study, the intended amount of shortening was nearly twice that of the actual shortening achieved. The exact cause of this discrepancy has not been determined. We used 3 patellar height indices in this study: BP, CD, and IS. Consensus is lacking as to which index is most accurate in measuring patellar height. 4,5 It is interesting that the IS ratio, which references patellar tendon length, stayed minimally elevated postoperatively in our cohort, but the BP and CD ratios normalized. The IS ratio has been criticized for possible error from enthesopathic elongation of the patellar nose, but no patients in our cohort had an abnormally elongated patellar nose.
Although there were complications in this study, only 2 complications led to failure of the imbrication. One complication was due to repeatedly falling down stairs, and 1 complication was from noncompliance with the recommended initial nonweightbearing. Thus, neither patient was worse than before the imbrication surgery. Nevertheless, these complications should be weighed against the complications related to a tibial tuberosity osteotomy in a skeletally immature patient as well as in the adult, which can include nonunion, delayed union, proximal tibial fracture, hardware irritation or failure, and difficulties with revision surgery (ie, bone grafting). In a recent systematic review, the overall complication rate with tibial tuberosity osteotomies was found to be 4.6%, with a risk of 10.7% when the osteotomy was completely detached as in a distalization procedure. 23 Furthermore, removal of hardware is more common (48.3%) when the tuberosity has been completely detached compared with maintaining a hinge (36.7%). Recently, it has been noted the reoperation rate is higher in the subset of patients undergoing distalization (21.2%) for patella alta compared with anteromedialization alone (10.5%). 28
There are limitations to this study, with the primary limitation being follow-up of only 27 of the 54 patients (50%). The senior author’s practice serves as a tertiary referral center for complex patellofemoral problems, and radiographic follow-up outside of our home institution was not permitted by our institutional review board for patients who resided remotely. The second limitation is the lack of an intraoperative radiograph. This restricted our ability to know what the “time-zero” measurements were. The third limitation is the lack of documentation of range of motion and of patient-reported outcomes, although none of this cohort required manipulation under anesthesia. Fourth, radiographs can have a variable degree of magnification error, which can result in measurement inaccuracies. This could be corrected on radiographs with a magnification correction marker, which was not used on all of our radiographs.
In conclusion, patellar tendon imbrication is a safe and efficient technique to address patella alta in patients of all ages with recurrent patellar instability.
Footnotes
Final revision submitted April 22, 2020; accepted May 11, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.M.P. has received research support from Smith & Nephew and consulting fees from Ceterix and Trice Medical. M.G. has received educational support from Arthrex and Smith & Nephew and hospitality payments from Arthrosurface, DePuy, and DJO. J.P. is a member of the NBA/GE Healthcare Advisory Board. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Cleveland Clinic.