
Abstract
Background:
Remnant tensioning (RT) anterior cruciate ligament (ACL) reconstruction has been reported to have excellent postoperative outcomes for femoral-side tears. However, the influence of remnant continuity (RC) on the postoperative results after RT ACL reconstruction remains unclear.
Purpose:
To investigate the effects of RC on the postoperative clinical, radiological, and second-look arthroscopic outcomes after RT ACL reconstruction for femoral-side ACL tears.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study included 94 patients who underwent RT ACL reconstruction using the hamstring tendon for femoral-side ACL tears between 2015 and 2020. The patients were divided into 2 groups according to the continuity of the remnant tissue: RC (n = 50) and remnant discontinuity (RD) (n = 44). Stability tests, including the Lachman and pivot-shift tests, side-to-side difference on Telos stress radiographs and KT-2000 arthrometer, patient-reported outcome measurements (PROMs), and graft status on postoperative magnetic resonance imaging (MRI) and second-look arthroscopy were evaluated.
Results:
Results of all stability tests and PROMs significantly improved postoperatively. The mean follow-up periods were 35.3 and 36.8 months in the RC and RD group, respectively. The 2 groups showed no statistically significant differences in stability outcomes or PROMs. Furthermore, the RC and RD groups showed comparable postoperative graft status on postoperative MRI and second-look arthroscopy.
Conclusion:
RT ACL reconstruction for RD between the femoral insertion site and ACL tissue showed comparable postoperative outcomes, including stability test, PROMs, postoperative MRI, and second-look arthroscopic data, to surgery for RC in femoral-side tears.
Dealing with anterior cruciate ligament (ACL) remnant tissue is still one of the concerns in treatment of ACL tear. Some surgeons have attempted to use proximal retensioning and fixation of the ACL remnant with augmentation using synthetic materials such as the InternalBrace (Arthrex) rather than reconstruction, especially in acute femoral-side tears.4,30 They reported that ACL repair with augmentation showed comparable results to ACL reconstruction. However, higher graft failure than ACL reconstruction was reported after ACL repair.7,44
When a surgeon decides to perform ACL reconstruction, remnant-preserving ACL reconstruction may be a good option. The remnant-preserving ACL reconstruction has been reported to improve mechanical stability, biological healing of the ACL graft, and knee function.39,40 Several studies have demonstrated excellent outcomes after remnant-preserving ACL reconstruction; however, the amount of remnant tissue preserved and the method of handling the preserved remnant slightly differed in previous studies.15,25,34 The importance of continuous remnant preservation has been emphasized in previous studies.34,43 However, preservation of noncontinuous remnant tissue had concerns of impingement and formation of cyclops lesions, and some studies have demonstrated little benefit of preserving noncontinuous remnant tissue.28,39,41
Combined ACL reconstruction and remnant tensioning (RT) with suture materials, among various remnant-preserving techniques, has demonstrated excellent postoperative outcomes with few cyclops lesions.32,38 One study had called this surgical technique of ACL reconstruction with remnant pullout suture in femoral-side tear as “ACL repair and reconstruction.” 14 With the tensioning of remnant ACL tissue, better healing of the grafted ACL is expected, and additional stability could be achieved.2,17 Therefore, the success of the repaired noncontinuous remnant tissue healing to the femoral attachment site is thought to lead to a similar postoperative function of continuous remnant ACL. The effect of the RT technique on postoperative outcomes after ACL reconstruction has been investigated; however, the influence of remnant continuity (RC) on postoperative results after RT ACL reconstruction remains unclear.
Therefore, the purpose of our study was to investigate the effects of RC on the postoperative clinical, radiological, and second-look arthroscopic outcomes after RT ACL reconstruction for femoral-side ACL tears. It was hypothesized that the noncontinuous remnant condition would show comparable postoperative outcomes to the continuous remnant status for femoral-side tears.
Methods
Patients
This study retrospectively included patients who underwent RT ACL reconstruction using the hamstring tendon for ACL tears between January 2015 and March 2020. The indications for RT ACL reconstruction included ACL rupture based on a clinical examination associated with proximal tears on magnetic resonance imaging (MRI) scans (including Sherman types 1 and 2). 9 The final decision on whether to perform RT ACL reconstruction was made after arthroscopic examination. The exclusion criteria were as follows: (1) skeletally immature patients, (2) follow-up of <1 year, (3) time between ACL tear and surgery of >1 year, and (4) multiligament or contralateral ACL injury. Overall, 133 patients were screened in this study. Among them, 4 patients were skeletally immature and underwent surgery, 14 were followed up for <1 year, time between ACL tear and surgery was >1 year for 6 patients, 12 patients were diagnosed with Sherman type 3 tears, and 3 patients underwent contralateral ACL surgery. Finally, 94 patients (94 knees) were enrolled (Figure 1). The demographic and intraoperative data are presented in Table 1.

Flowchart of patient enrollment in the study. ACL, anterior cruciate ligament; RC, remnant continuity; RD, remnant discontinuity.
Demographic and Intraoperative Data of Enrolled Patients a

Values are presented as mean ± SD (range) or n.
Patients were divided into 2 groups according to the continuity of the remnant tissue. Continuity was determined by arthroscopic examination. Based on arthroscopic probing, RC was defined as any continuity between the femoral insertion site and the remnant tissue. Contrastingly, remnant discontinuity (RD) was considered when no continuity existed between the femur and the remnant (Figure 2). 43 Among the enrolled patients, 50 and 44 were assigned to the RC and RD groups, respectively. This study was approved by the ethics committee of our institution.
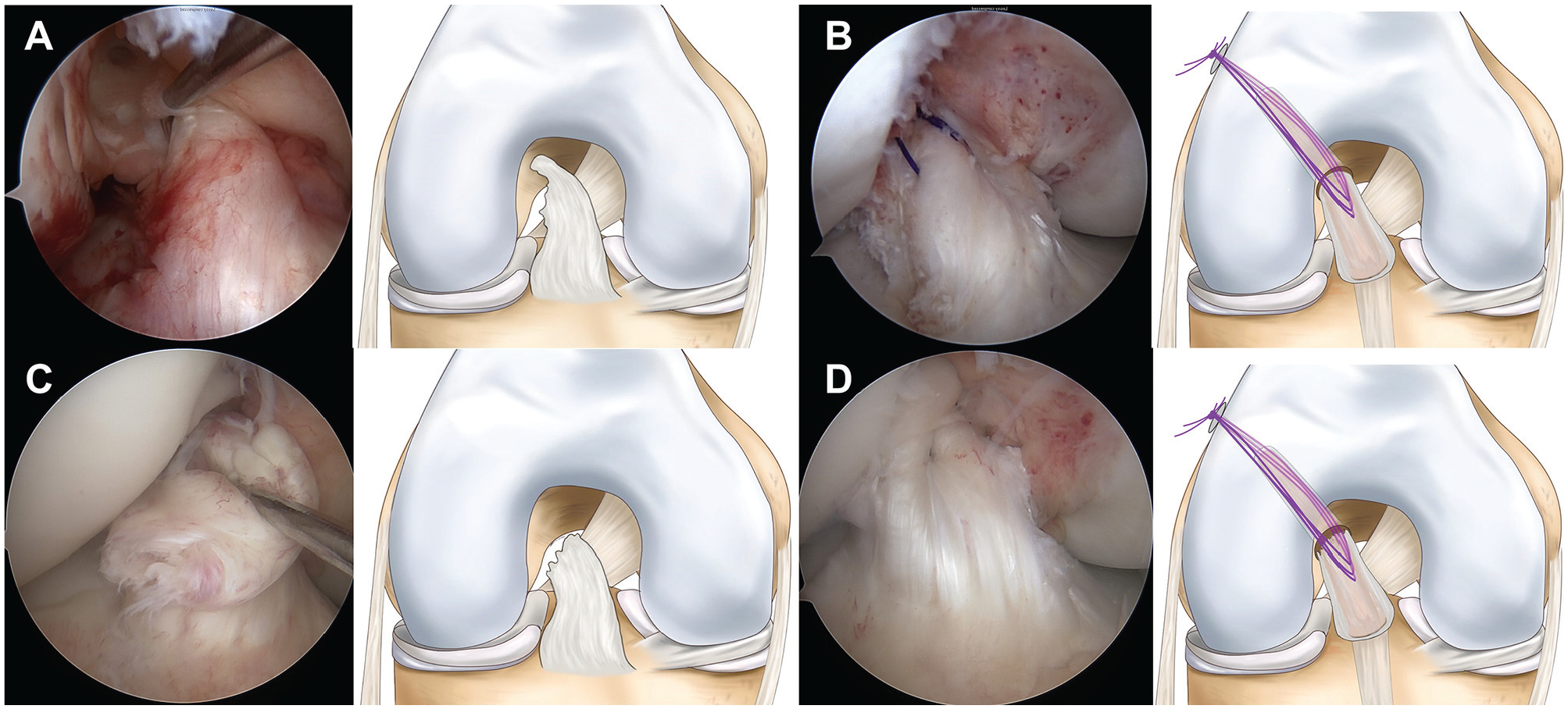
Arthroscopic examination of (A) remnant continuity (RC) group and (C) remnant discontinuity (RD) group. (B) Concomitant remnant anterior cruciate ligament retensioning was performed in the RC group to improve remnant tension. (D) Concomitant remnant anterior cruciate ligament repair and reconstruction with tendon graft was performed in the RD group with minimal damage to the proximal remnant.
Surgical Technique and Rehabilitation
All surgeries were performed by an experienced surgeon at a single institution (J.H.W.). Standard arthroscopic portals were routinely formed, and diagnostic arthroscopy was performed.
Appropriate meniscal procedures were performed depending on tear characteristics before RT ACL reconstruction to identify combined meniscal tears. Given the high healing potential of meniscal repair when performed alongside ACL reconstruction, and the association of meniscectomy with increased laxity, meniscal repair was preferred over meniscectomy for combined meniscal tears. 24 Hamstring tendon was harvested after confirming the ACL tear routinely. A 4-stranded double-loop hamstring tendon graft was routinely created. When the graft diameter was <7 mm, 5-stranded (triple-stranded semitendinosus tendon + double-stranded gracilis tendon) or 6-stranded (triple-stranded semitendinosus + gracilis tendon) grafts were used. The graft diameter was recorded. For the pullout suture of the remnant ACL tissue, No. 0 polydioxanone suture (PDS; Ethicon) was applied to the remnant ACL 3 times using a suture hook (Linvatec) (Figure 3A). The free end of the suture was brought to the accessory anteromedial portal. The outside-in technique via the posterolateral (PL) portal method was used to minimize damage to the RC or the proximal site of the remnant. 1 After making the PL portal by the transillumination technique, a 70° arthroscope was inserted through the PL portal and advanced to reach the posterior aspect of the intercondylar notch. Then, the ACL femoral guide (Arthrex) was advanced from the anterior portal (anterolateral or transpatellar tendon portal) 33 (Figure 3B). The femoral tunnel was created by the outside-in technique using a FlipCutter device (ACL RetroConstruction System).

Arthroscopic snapshot during surgical procedure for right-sided knee. (A) Three No. 0 polydioxanone suture (PDS) stitches were applied (viewing portal: anterolateral; working portal: anteromedial). (B) Anterior cruciate ligament (ACL) femoral guide was introduced via the transpatellar tendon portal. The viewing portal was posterolateral, using a 70° arthroscope. (C) Passage of the graft and 3 PDS stitches (viewing portal: posterolateral). (D) After graft fixation, the 3 PDS stitches were tied over a suspensory device (viewing portal: anterolateral). LFC, lateral femoral condyle; LMPH, lateral meniscus posterior horn.
Tibial tunnel formation was similar to routine tunnel formation. The arthroscope was advanced through the anterolateral portal, and a small incision was made at the center of the tibial stump. Subsequently, a 50°ACL tibial guide was used. Reaming was carefully performed to minimize damaging the tibial remnants. After tibial tunnel formation, the arthroscope was reinserted through the PL portal to show the graft and PDS passage (Figure 3C). When passing the ACL graft, 3 PDS stitches were pulled out via the femoral tunnel. Endobuttons (Smith & Nephew) were used for femoral-side graft fixation, and hybrid fixation that combined intratunnel aperture fixation (using a bioabsorbable screw) and extracortical suspensory fixation (using a cortical screw and spike washer) was applied for tibial-sided fixation. Grafts were tensioned according to the maximal surgeon-applied tension with a concomitant posterior tibial force, and grafts were fixed on the knee joint full extension. 5 After ACL graft fixation, 3 PDS stitches pulled out through the femoral tunnel were tied over the Endobutton on the knee joint full extension (Figure 3D).
Range of motion exercises were started 2 days postoperatively, and 120° of knee flexion was performed within 4 weeks postoperatively. Straight-leg raises, quadriceps sets, and ankle pump exercises were encouraged on postoperative day 1. Crutch-assisted weightbearing was initiated on postoperative day 1. Full weightbearing walking was permitted at 6 weeks postoperatively. When concomitant meniscal repair was performed, range of motion exercises and weightbearing walking were delayed for 2 weeks. Returning to sports was allowed 9 months postoperatively, depending on the patient's condition.
Graft Evaluation
Postoperative MRI was recommended to evaluate ACL grafts between 6 and 9 months postoperatively. This examination was performed for patients who agreed after an explanation. Nonroutine MRI was performed in patients who experienced knee trauma. When patients underwent postoperative MRI >1 time, the last one was analyzed. Graft continuity was classified as no, partial, or complete tear as previously described. 35 A partial tear was defined as a significant signal change with an intact graft. A complete tear was defined as the loss of graft continuity on MRI (Figure 4).

Magnetic resonance imaging classification of the anterior cruciate ligament graft. (A) No tear, (B) partial tear, and (C) complete tear. Partial tear showed significant signal change; however, graft continuity was maintained. Complete tear showed loss of graft continuity. (C) also showed cyclops lesion.
Second-look arthroscopy was performed when patients underwent hardware removal. Hardware removal was performed in patients who (1) had cortical screw or washer-related irritation or (2) wanted the cortical screw and washer to be removed. Graft continuity and synovial coverage were evaluated using second-look arthroscopy. Graft continuity was graded as no, superficial, or substantial tear. 42 Superficial tear was defined as a tear with superficial fibers, and a substantial tear was defined as a tear with graft rupture. The synovial coverage was graded as good (>80% coverage of the graft), fair (50%-80% coverage), or poor (<50% coverage). 21 The presence of cyclops lesions was also evaluated. A cyclops lesion was defined as a pedunculated or nonpedunculated nodule of fibrovascular tissue around the ACL graft that was >5 mm in diameter 13 (Figure 5). Graft failure was defined as revision ACL, complete tear on postoperative MRI, or substantial tear on second-look arthroscopy.

Second-look arthroscopic finding of the anterior cruciate ligament graft. Graft continuity was divided as (A) no tear, (B) superficial tear, or (C) substantial tear. Synovial coverage of the graft was graded as (D) good (>80%), (E) fair (50%-80%), or (F) poor (<50%). (G) Evaluation of cyclops lesions.
Stability Test and Clinical Assessment
Demographic data, including age, sex, height, weight, body mass index, follow-up period, operative time, and time between injury and surgery, were obtained. Knee stability tests were performed using a physical examination and testing devices. A postoperative knee stability test was performed at the final follow-up. A senior author (J.H.W.) performed physical examinations, including Lachman and pivot-shift tests, preoperatively and at the last follow-up. The Lachman test was graded as 0, 1 (<5 mm), 2 (5-10 mm), or 3 (>10 mm), and the pivot-shift test as 0 (absent), 1 (glide), 2 (clunk), or 3 (gross).11,48 A KT-2000 arthrometer device (MEDmetric Corp), was used in standard fashion and Telos stress radiography (Telos GmbH; Laubscher) were used to quantify the Lachman test. Preoperative and postoperative Telos stress radiography (150 N on the tibia at 20° knee flexion) were assessed.16,19,20 The reference line was drawn parallel to the medial tibial plateau. The distance between the perpendicular lines of most of the posterior contours of the femoral condyle and the tibial plateau was defined as the anterior tibial translation. A side-to-side difference (STSD) in anterior tibial translation between the injured and contralateral noninjured knees was measured to compare with the contralateral side.
Patient-reported outcome measurements (PROMs), including the Lysholm 37 and the International Knee Documentation Committee (IKDC) subjective scores,3,12 were obtained preoperatively and at the last follow-up. All outcomes were compared between both groups. Preoperative and postoperative outcomes were compared.
Statistical Analysis
The Shapiro-Wilk test was used to investigate the normality of the distribution. The Student t test was used for continuous variables, whereas the chi-square test was used for categorical variables to compare the group outcomes. The paired t test for continuous variables and the chi-square test for categorical variables were used to compare the pre- and postoperative outcomes. Statistical significance was set at P < .05. All data were analyzed using SPSS software (Version 27; IBM). A power analysis was performed to determine the sample size required to demonstrate statistical significance. STSDs on Telos stress radiographs were defined as the primary outcome. A total of 25 patients were required for each group to detect a difference of 1.7 mm with an SD of 2.2 mm with >80% power (α = .05). 10 As the number of patients participating in this study exceeded the number determined by power analysis, it would take 98% statistical power to detect a difference of ≥1.7 mm with an SD of 2.2 mm in STSD between the RC and RD groups.
Results
When comparing the demographic and intraoperative data between the RC and RD groups, only height was significantly greater in the RD group, whereas body mass index was not significantly different (Table 2).
Comparison of Demographic and Intraoperative Data Between Remnant Continuity and Discontinuity Groups a

Values are presented as mean ± SD or n unless otherwise indicated. Bold P value indicates statistical significance. RC, remnant continuity; RD, remnant discontinuity.
Postoperatively, 47 (94.0%) and 38 (86.4%) patients in the RC and RD groups underwent postoperative MRI, respectively. Graft continuity on postoperative MRI did not differ significantly between the 2 groups. One patient in the RD group had a complete tear (Table 3).
Comparison of Magnetic Resonance Imaging and Second-Look Arthroscopic Results Between the 2 Groups a

Values are presented as mean ± SD or n unless otherwise indicated. Bold P value indicates statistical significance. MRI, magnetic resonance imaging; RC, remnant continuity; RD, remnant discontinuity.
A total of 31 (62.0%) and 23 (52.3%) patients in the RC and RD groups underwent second-look arthroscopy, respectively. Among groups RC and RD, 10 and 8 patients, respectively, underwent screw removal and second-look arthroscopy due to tibial screw irritation. The remaining patients underwent surgery because they desired screw removal. None of the patients who underwent second-look arthroscopy showed cyclops-associated symptoms. The time from RT ACL reconstruction to the second-look examinations was significantly longer in the RC group. Graft continuity and synovial coverage on second-look arthroscopy were not significantly different between groups. One patient in the RC group showed a substantial tear on the second-look examination; other patients had no tears. Approximately 96% and 91% of the patients who underwent second-look arthroscopy showed good or fair synovial coverage in the RC and RD groups, respectively. However, 16% and 13% of patients in the RC and RD groups, respectively, had cyclops lesions on the second-look examination (Table 3). None of the 8 patients with cyclops lesions showed cyclops-associated symptoms.
Similar to physical examination, the postoperative KT-2000 arthrometer (4.3 mm ± 1.9 mm vs 1.6 mm ± 1.2 mm; P < .001) and STSD (5.2 mm ± 1.8 mm vs 1.0 mm ± 1.7 mm; P < .001) showed significantly lower laxity. Postoperatively, the Lysholm (64.5 ± 20.1 vs 87.0 ± 10.8; P < .001) and IKDC subjective scores (50.6 ± 16.0 vs 78.9 ± 16.7; P < .001) improved significantly. When comparing the preoperative data between the RC and RD groups, all data were not significantly different (Table 4).
Comparison of Preoperative Data Between Remnant Continuity and Discontinuity Groups a

Values are presented as mean ± SD or n. IKDC, International Knee Documentation Committee; RC, remnant continuity; RD, remnant discontinuity; STSD, side-to-side difference.
Postoperative STSD was not significantly different between the 2 groups. Other postoperative stability tests, including the Lachman test, pivot-shift test, and KT-2000, were also not significantly different. The postoperative Lysholm score, IKDC subjective score, and graft failure rate did not differ between the groups (Table 5).
Comparison of Postoperative Data Between Remnant Continuity and Discontinuity Groups a

Values are presented as mean ± SD or n unless otherwise indicated. IKDC, International Knee Documentation Committee; RC, remnant continuity; RD, remnant discontinuity; STSD, side-to-side difference.
Discussion
The most important finding of the present study was that patients with RD between the femoral insertion site and ACL tissue showed similar postoperative outcomes, including stability test, PROMs, postoperative MRI, and second-look arthroscopic data, compared with those who had RC after RT ACL reconstruction for femoral-site ACL tears.
Preservation of the ACL remnant tissue has several theoretical advantages, including preservation of vascularization and proprioceptive nerve fibers. 39 Decreased proprioception of the knee joint could induce the progression of osteoarthritis. 22 Disruption of the afferent component of protective neuromuscular reflexes due to impaired proprioception might induce poor spatial and temporal coordination of position sense, decreased muscle activity, and poor coordination of the quadriceps and hamstrings, which can result in a greater exposure of the knee joint to wear and tear. Several studies had reported that preservation of proprioceptive function was important for prevention of knee joint arthritis. 26 Previous studies have demonstrated that remnant-preserving reconstruction surgery is associated with improved joint position sense, less postoperative bone tunnel enlargement, and better synovial coverage.29,36 However, the improvement of stability after remnant-preserving surgery was inconsistent. Won et al 47 reported that remnant-preserving ACL reconstruction was associated with better anterior stability in a meta-analysis of 5 randomized controlled trials and 6 observational studies. Meanwhile, Tie et al 41 demonstrated that the outcome of single-bundle ACL reconstruction with the remnant preservation technique was similar to that with the remnant resection technique for anterior laxity and functional recovery from a meta-analysis of 6 randomized controlled trials. Because of the debate on the advantages of remnant tissue–preserving ACL reconstruction, it has not gained global adoption, and the remnant tissue is often resected or debrided to improve visualization. However, the amount of remnant tissue preserved and the method of handling the preserved remnants were slightly different in previous studies. We postulated that adequate surgery with good-quality remnant preservation could yield better postoperative stability. Although RT ACL reconstruction is a labor-intensive procedure, we think that performing it whenever possible may result in better patient outcomes. Therefore, RT ACL reconstruction is attempted for Sherman type 1 or 2 ACL tears as possible.
Crain et al 6 investigated the effect of resecting ACL remnant tissue on anteroposterior laxity intraoperatively. They enrolled 48 patients and reported that resection of remnant types 1 to 3 resulted in greater intraoperative anteroposterior laxity and that 14 (29%) of 48 participants showed >2-mm laxity increment after remnant ACL resection before the ACL reconstruction surgery. Van Keulen et al 43 compared postoperative outcomes between continuous remnant preservation and standard ACL reconstruction. They reported that ACL reconstruction with residual continuous remnant tissue preservation led to lower clinical failure and revision ACL surgery rates than standard ACL reconstruction. Franciozi et al 8 divided patients who underwent remnant-preserving ACL reconstruction into remnant tissue functional and nonfunctional groups and compared the outcomes. They reported that a functional remnant was correlated with less laxity. According to previous studies, continuous remnant ACL preservation was associated with better stability. In our study, the RD group showed comparable postoperative outcomes, including the stability tests. This finding suggests that repaired and retensioned discontinuous remnant tissue may function similarly to continuous remnant tissue in ACL reconstruction.
The occurrence of cyclops lesions, known as localized anterior arthrofibrosis, is one of the concerns of remnant-preserving ACL reconstruction. 31 The incidence of cyclops lesions has been reported to vary widely (1%-47%). 18 Interestingly, recent studies reported that remnant-preserving ACL reconstruction showed fewer cyclops formations without statistical significance at the second-look arthroscopic examination.13,23,45 Studies investigating ACL repair nearly did not report cyclops-related symptoms despite remnant tissue preservation.9,30,46 In our study, 5 and 3 patients had cyclops lesions in the second-look examination in RC and RD groups, respectively. None of the 8 patients showed cyclops-associated symptoms, including an extension deficit. We believe that concomitant ACL repair during reconstruction is not closely related to cyclops formation, unlike leaving remnant tissue unaltered. Further studies comparing the incidence of cyclops formation between RT ACL reconstruction and conventional ACL reconstruction are needed to clearly identify the influence of concomitant ACL repair on cyclops formation.
Numerous grafts were able to be grafted for ACL reconstruction. Among those, the commonly used autograft types are bone-patellar tendon-bone, hamstring, and quadriceps tendon. 27 Performing ACL reconstruction surgery while preserving the remnant tissue is a labor-intensive procedure compared with performing it without preservation. Moreover, the surgical time could be prolonged when using a thicker graft or implanting a bone plug, particularly when employing bone–patellar tendon–bone or quadriceps tendon grafts. In the present study, the RT ACL reconstruction was performed using hamstring tendon, so that applicability of these results might be limited when using different graft types or fixation devices. Further research is needed to elucidate the outcomes associated with different grafts or fixation devices.
Limitations
First, due to lack of comparative analysis between postoperative outcomes of ACL reconstruction without remnant preservation and those with RT in Sherman type 1 or 2 ACL tear, any potential advantages or disadvantages of remnant-preserving technique were unable to be identified in our study. Second, the time from RT ACL reconstruction to second-look arthroscopic examination was approximately 5 months later in group RC. However, the time interval for both groups was >18 months. Therefore, the influence of this time interval difference was unlikely to represent a major bias in interpreting the second-look arthroscopic results. Third, not all patients were evaluated using postoperative MRI or second-look arthroscopy, and patients who underwent second-look examination and those who underwent postoperative MRI were not the same. Therefore, a selection bias may exist when interpreting these results. Fourth, only patients of a single ethnicity were enrolled in our study. Therefore, applying our results to patients of other ethnicities could lead to bias. Fifth, the follow-up period was relatively short; therefore, osteoarthritic changes and revision rates could not be fully evaluated. Therefore, further long-term studies are required. Fifth, this study was retrospective and nonrandomized, and 39 patients were excluded after applying the exclusion criteria; therefore, selection or information biases may exist. Despite several limitations, RT ACL reconstruction could be a good option regardless of remnant tissue continuity when surgeons plan ACL reconstruction for femoral-side ACL tears.
Conclusion
RT ACL reconstruction for RD between the femoral insertion site and ACL tissue showed comparable postoperative outcomes, including stability test, PROMs, postoperative MRI, and second-look arthroscopic data, to surgery for RC in femoral-side tears.
Footnotes
Final revision submitted September 21, 2024; accepted November 12, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This research was supported by Korean Fund funded by Ministry of Science and Information and Communication Technology, as well as Ministry of Health and Welfare (RS-2024-00340610, RS-2024-00334810; Republic of Korea). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Samsung Medical Center (SMC2023-11-008).