
Abstract
Background:
Graft selection is an important part of preoperative planning for anterior cruciate ligament reconstruction (ACLR). In addition, ACLR with the remnant preservation technique has recently gained attention due to potential benefit in bone-tendon healing, graft revascularization, and proprioceptive nerve remodeling. However, the ideal graft choice remains controversial, and there is limited research comparing autograft and allograft in ACLR with remnant preservation.
Purpose:
To compare knee muscle strength, neuromuscular control, and patient-reported outcomes between hamstring (HS) tendon autografts and tibialis anterior (TA) allografts in patients undergoing ACLR with remnant preservation through posterior transseptal portal for >1 year.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 70 patients who underwent ACLR with remnant preservation between 2018 and 2021 using HS tendon autograft (n = 35) or TA allograft (n = 35) were analyzed at 3 different time points (preoperative, 6 months, and 12 months). Quadriceps and HS muscle strengths were measured with an isokinetic device. Proprioception was evaluated with reproduction of passive positioning for joint position sense and overall stability index (OSI) for dynamic postural stability. Patient-reported outcomes included the Lysholm score and the International Knee Documentation Committee score.
Results:
There were no significant differences in demographic information including age, body mass index, concomitant meniscal injuries, and sports activities (P > .05) between HS tendon autograft and TA allograft groups. Quadriceps and HS strength in both groups, HS strength in deep knee flexion in both groups, and OSI in the HS tendon autograft group significantly improved at 12 months (P < .05). Repeated-measures analysis of variance revealed significant interactions between time and grafts for OSI (F[2, 136] = 5.08; P = .007). The subsequent independent t test demonstrated that the OSI was significantly higher in the TA allograft group (2.7 ± 1.0) than that of the HS tendon autograft group (2.1 ± 0.8) at 12 months (P = .009), indicating better dynamic postural stability in the HS tendon autograft group.
Conclusion:
No significant differences were found in knee muscle strength or patient-reported outcomes between HS tendon autograft and TA allograft after ACLR with remnant preservation for up to 1 year except for dynamic postural stability favoring HS tendon autograft.
Keywords
Anterior cruciate ligament (ACL) rupture accounts for nearly 50% of all sports-related knee injuries, 23 and ACL reconstruction (ACLR) is one of the most common surgeries performed by orthopaedic surgeons. 20 Graft selection is a crucial part of the preoperative planning for ACLR and may depend on several factors such as age, 8 sports participation, 40 and surgeon preference. 35
The most widely used graft types include bone–patellar tendon–bone (BPTB), hamstring (HS) tendon, and quadriceps tendon autografts as well as various allograft options. 44 Although BPTB autografts have historically been considered the gold standard owing to the ease of harvesting and opportunity for bone-to-bone healing, 14 the disadvantages of BPTB autografts include anterior knee pain and donor-site morbidity. On the other hand, HS tendon autografts have gained popularity due to satisfactory clinical outcomes with a recent meta-analysis reporting superior knee functional outcomes compared with BPTB, 19 reduced anterior knee pain and kneeling discomfort, and less donor-site morbidity.2,6,18 Further, allografts have also been commonly used owing to a shorter surgical time, improved cosmesis, and diverse graft options and sizes.12,39
ACLR graft has been widely studied; however, it remains a highly debated topic, and the ideal graft choice remains controversial, as evidenced by multiple systematic reviews with different conclusions. Some systematic reviews showed similar functional and patient-reported outcomes between autografts and nonirradiated allografts,30,48 although autografts may have more advantages than irradiated allografts in terms of function and stability.43,48 Recently, a systematic review with network meta-analysis revealed that different graft types resulted in superior outcomes in different situations, 32 and patellar tendon autografts may be the most appropriate graft based on the International Knee Documentation Committee (IKDC) scores and Lachman tests.
Despite these findings, some of the less explored yet important clinical considerations for graft selection are knee muscle strength and neuromuscular control. Knee muscle strength has been commonly compared between BPTB and HS tendon autografts25,45 but not between HS tendon autografts and tibialis anterior (TA) allografts. Neuromuscular control, which is crucial for maintaining knee stability, is affected in patients undergoing ACLR17,28; however, little is known regarding any difference in the recovery of neuromuscular control between autografts and allografts. Furthermore, several recent studies have demonstrated that ACLR with the remnant preservation technique could enhance bone-tendon healing, graft revascularization, proprioceptive nerve remodeling, muscle strength, and joint function.3,11,21,29,36,42 Efforts are made to preserve as much ACL stump as possible. However, there is a lack of research comparing postoperative outcomes between autografts and allografts in ACLR using the remnant preservation technique.
Therefore, this study aimed to compare knee muscle strength, neuromuscular control, and patient-reported outcomes between HS tendon autografts and TA allografts in patients undergoing ACLR with remnant preservation for >1 year. We hypothesized that there would be differences in functional and patient-reported outcomes between HS tendon autografts and TA allografts.
Methods
Study Design and Population
The institutional review board (2018AN0261) affiliated with the senior author (K.-M.J.) approved this prospective comparative study. We enrolled 321 patients who underwent primary ACLR with remnant preservation using HS tendon autografts or irradiated TA allografts between August 2018 and December 2021. Informed consent was acquired from all patients and/or their legal guardians. The exclusion criteria were as follows: (1) concomitant ligament rupture; (2) revision ACLR; (3) knee osteoarthritis (Kellgren-Lawrence grade >1); (4) inability to undergo isokinetic and postural stability tests owing to pain or restricted motion of the knee joint; (5) vestibular and visual impairment or neurological dysfunction; (6) lack of functional and patient-reported outcome data; (7) pain, dysfunction, or history of previous surgery in the nonoperated knee; and (8) loss to follow-up. After excluding patients based on these criteria, 70 patients (HS tendon autografts = 35 and TA allografts = 35) were analyzed at 3 different time points (preoperative, 6 months, and 12 months) (Figure 1).

CONSORT (Consolidated Standards of Reporting Trials) flowchart of patient inclusion and exclusion criteria. ACLR, anterior cruciate ligament reconstruction; ROM, range of motion.
Operative Procedure
All surgeries were performed using the anatomical single-bundle ACLR with the remnant preservation technique by the senior author, a single knee arthroscopy specialist. The graft selection was decided through in-depth discussions with patients after detailed explanation about advantages and disadvantages with each graft type. Routine arthroscopic examinations were performed using the anterolateral (AL) and anteromedial (AM) portals. Any concomitant pathology of the menisci or cartilage was treated before ACLR. Most of the ACL tears occurred at the femoral attachment site and midsubstance. Efforts were made to preserve as much of the ACL remnant stump as possible, regardless of the amount of remaining tissue. In the HS tendon autograft group, the semitendinosus and gracilis tendons were harvested using a standard tendon stripper and prepared on a back table. All operations were performed using graft diameter of 8 mm to 10 mm regardless of the graft type. To preserve as much of the remnant ACL tissue as possible, a femoral tunnel was created under direct observation through the posterior transseptal (PTS) portal. An arthroscope was inserted through the AL portal and reached the posteromedial (PM) compartment. A PM portal was created using the transillumination technique, and a posterolateral (PL) portal was created similarly. The PM and PL compartments were connected through the PTS portal using an electric shaver. After establishing the PTS portal, the ACL femoral footprint was directly observed through the PTS portal while preserving remnant ACL tissue. Subsequently, we created a femoral tunnel using FlipCutter drill (Arthrex) and ACL RetroConstruction System (Arthrex) using the outside-in retrograde-reaming technique. The tibial tunnel was created using a 55° tibial guide, which was inserted into the knee joint through the AM portal. The guide tip was located at the ACL tibial footprint. A guide pin was inserted into the AM aspect of the proximal tibia. A tibial tunnel was created along the guide pin using a reamer of the same size as the femoral tunnel diameter. Finally, the prepared graft was passed and secured using a TightRope RT (Arthrex) on the femoral side and a bioabsorbable interference screw (Smith+Nephew) with a post tie (fixation of distal ends of the tendon graft using a post tie washer screw) on the tibial side.
Rehabilitation Protocol
The rehabilitation protocol was divided into 4 phases and implemented equally in both groups. The first phase was the recovery period following the operation (< postoperative 6 weeks), with the goal of controlling pain, reducing swelling, recovering the range of motion and flexibility, and normalizing gait. The second phase was the recovery period of general function (postoperative 6 to 12 weeks), and the goal was to strengthen muscle and begin proprioception training. The third phase was the recovery period of functional performance (postoperative 13 to 24 weeks) to progressively enhance muscle strength, proprioception, and neuromuscular control, including plyometric and agility. The final phase was the preparation period for returning to sports (> postoperative 24 weeks) including sports-specific technical movement training.
Outcome Measures
Outcome measures consisted of knee muscle strength, joint position sense (JPS), dynamic postural stability, and patient-reported outcomes. Quadriceps and HS muscle strength were measured using an isokinetic device (Biodex Multi-Joint System 4, Biodex Medical Systems, Inc). 41 All measurements were conducted in an upright sitting position. All patients performed a maximum of 15 repetitions of flexion and extension on each leg at 180 deg/s. The HS and quadriceps muscles were measured at 100° to 0° in the concentric/concentric action mode, and the peak torque value was recorded (N·m/kg). 34
The JPS test was performed to evaluate knee joint proprioception by measuring the reproduction of passive positioning (RPP). 27 Patients sat in an isokinetic device with their eyes closed and knees bent at 90°. The patients were then instructed to perform a predetermined extension of the knee (45° of knee flexion in our study) and hold it for 5 seconds with instructions to remember the exact position. The Biodex system then passively moved the knee, and when the patients thought that the angle of the knee joint had arrived at the previous target angle (45° of knee flexion), they were asked to press the switch. The deviation between the angles indicated by the patient and target angle was documented. Patients underwent RPP tests twice on both legs, with a 30-second rest period between tests. A negative value suggested that the patients pressed the switch before reaching the target angle (45° of knee flexion).
The overall stability index (OSI) was assessed using the Biodex Stability System (Biodex Medical Systems) to assess dynamic postural stability. The foot platform of the Biodex Stability System was able to move from a 0° to 20° tilt in any direction, whereas the stability level automatically dropped from level 12 (most stable) to level 1 (most unstable) by 1 level every 1.66 seconds. The dynamic postural stability test was performed while standing barefoot on 1 leg. The patients completed 2 tests, each lasting 20 seconds, with 10 seconds of rest between the tests. A high stability index implied poor dynamic postural stability. 41
Patient-reported outcomes included Lysholm and IKDC scores. The Lysholm and IKDC scores consisted of 8 items (limping, support, restraining, instability, pain, swelling, climbing stairs, and squatting) and 3 items (symptoms, function, and sports activities), respectively. Lower scores indicated more severe symptoms and poorer functioning level. 13
Statistical Analysis
Independent t tests and chi-square tests were used for continuous and categorical variables, respectively, to compare demographic information between the 2 groups. Repeated-measures analysis of variance (ANOVA) with 1 between-patient factor (HS tendon autograft vs TA allograft) and 1 within-patient factor (preoperative, 6 months, and 12 months) was used to investigate group differences in outcomes across the time points. An advantage of ANOVA was its robustness to violations of normality, particularly with a sample size >20. When sphericity could not be assumed, Greenhouse-Geisser corrections were applied. Post hoc independent-samples t tests were performed to compare the groups at preoperative, 6 months, and 12 months when repeated-measures ANOVA was significant for interaction between time and group. Alpha level was set at 0.05, SPSS software version 21.0 (IBM) was used.
Results
Demographic information is summarized in Table 1, and there were no significant differences for age, height, weight, body mass index, injured side, dominant knee, concomitant meniscal injuries, or sports activities between the 2 groups (P > .05).
Demographic Data a

Data are presented as mean ± SD unless otherwise indicated. HS, hamstring; LM, lateral meniscus; MM, medial meniscus; TA, tibialis anterior.
Quadriceps and HS strength in both groups, HS strength in deep knee flexion in both groups, and OSI in the autograft group significantly improved at 12 months (P < .05). Repeated-measures ANOVA did not show any significant interactions between time and grafts in terms of quadriceps strength (F[1.73, 117.54] = 2.19; P = .12), HS strength (F[1.61, 109.8] = 0.956; P = .37), and RPP (F[2, 136] = 2.50; P = .09). In addition, repeated-measures ANOVA did not show any significant interactions between time and graft in terms of limb symmetry indices of the quadriceps and HS strength (Table 2).
Comparative LSI Outcomes of Quadriceps and HS Muscle Strength a
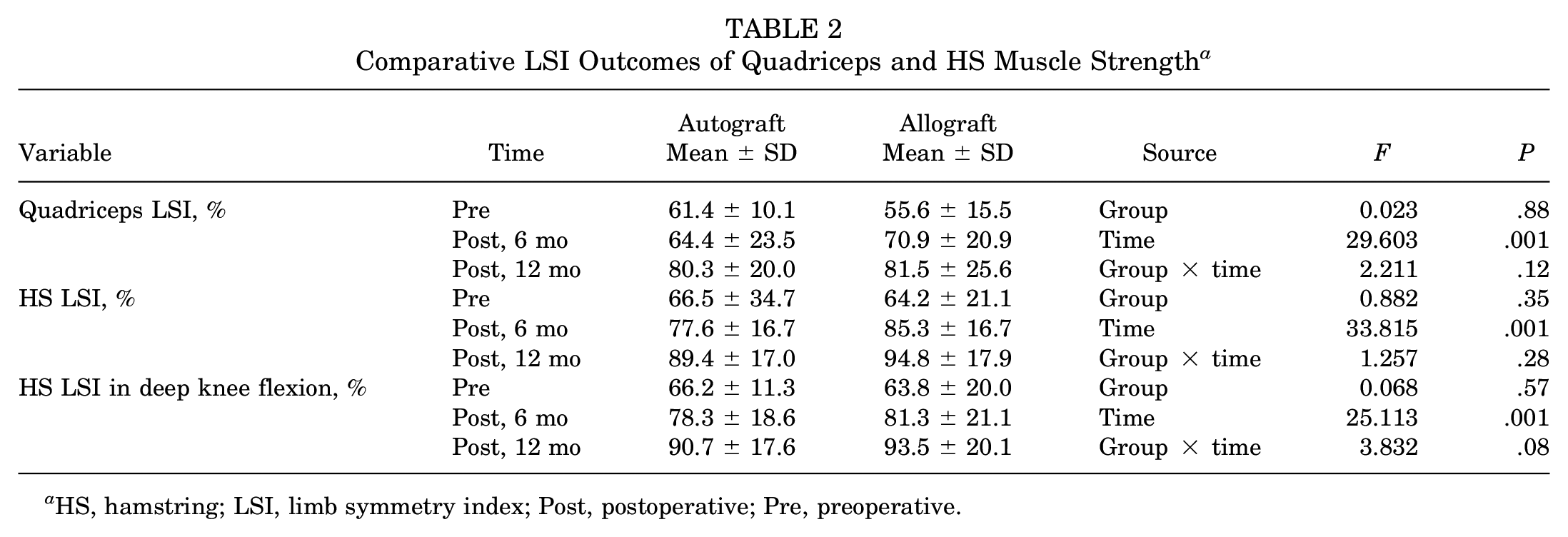
HS, hamstring; LSI, limb symmetry index; Post, postoperative; Pre, preoperative.
Repeated-measures ANOVA revealed significant interactions between time and graft for HS strength in deep knee flexion (F[1.73, 117.93] = 6.76; P = .003) and OSI (F[2, 136] = 5.08; P = .007). The subsequent independent t-test demonstrated that although there was no statistically significant difference in the HS strength in deep knee flexion between the groups, the OSI was significantly greater in the allograft group (2.7 ± 1.0) than that of the autograft group (2.1 ± 0.8) at 12 months (P = .009), indicating better dynamic postural stability in the autograft group (Table 3).
Comparative Neuromuscular Outcomes Between Autograft and Allograft ACLR a

ACLR, anterior cruciate ligament reconstruction; HS, hamstring; OSI, overall stability index; Post, postoperative; Pre, preoperative; RPP, reproduction of passive positioning; TA, tibialis anterior.
Both the Lysholm and the IKDC scores significantly improved in both groups at 12 months (P < .001). No significant interaction was observed between time and graft in Lysholm (F[1.67, 136] = 0.412; P = .63) and IKDC (F[1.48, 100.76] = 0.622; P = .49). These results are summarized in Table 4.
Comparative PROs Between Autograft and Allograft ACLR a

ACLR, anterior cruciate ligament reconstruction; HS, hamstring; IKDC International Knee Documentation Committee; Post, postoperative; Pre, preoperative; PRO, patient-reported outcome; TA, tibialis anterior.
Discussion
This study aimed to compare the functional and patient-reported outcomes between HS tendon autografts and TA allografts in patients undergoing ACLR with remnant preservation. We found that although knee muscle strength and patient-reported outcomes significantly improved at 12 months in both groups without significant differences between the groups, HS tendon autografts were associated with better dynamic postural stability than TA allografts in the operated knees.
ACL injuries can interfere with intricate interactions within the neuromuscular system, leading to impaired proprioception and kinesthesia, delayed muscle activation, and dynamic knee joint instability.4,24 Neuromuscular control after ACL injuries or ACLR has been evaluated using various evaluation methods such as proprioception, postural stability, functional performance, and isokinetic tests.4,24,28 In our study, JPS and OSI were measured to evaluate neuromuscular control. Although there were no significant differences between the 2 groups in terms of JPS, patients in the autograft group demonstrated lower OSI, indicating better dynamic postural stability. Previous studies have shown a decrease in the number of mechanoreceptors after ACL injury, which are responsible for afferent sensory input to the central nervous system.1,15,16,26 These mechanoreceptors are thought to exist in the cruciate ligaments, articular capsule, lateral collateral ligament, tendons, and muscles around the knee.5,38 Although the exact cause for better dynamic postural stability in the autograft group cannot be determined, given the similar knee muscle strength outcomes between the 2 groups, different recovery of mechanoreceptors in the ligaments or surrounding structures between the 2 groups might be considered as a possible cause. Therefore, further histological studies with large samples would be necessary to verify the difference in the recovery of mechanoreceptors between the 2 groups.
Another noteworthy finding was that no significant differences in subjective outcome measures, such as the IKDC and Lysholm scores, between HS tendon autografts and irradiated TA allografts were noted ≤1 year postoperatively in our study. There is still controversy regarding subjective outcomes after ACLR between autografts and allografts. Although some previous studies reported no statistically significant differences in subjective clinical outcomes between autograft and allograft groups,7,22 some recent systematic reviews concluded that autografts may offer greater advantages in IKDC and Lysholm scores than irradiated allografts in ACLR.43,48 Animal studies have proposed that irradiation could weaken the biological properties of allografts.37,47 Clinically, there has been concern regarding graft failure associated with irradiated allograft. 31 In addition, although rare, allografts pose a potential risk of disease transmission.9,49 However, allografts also have some advantages, including shorter recovery times and less postoperative pain, as well as no donor-site morbidity, which could induce better postoperative functional outcomes. 33 Therefore, in the present study, graft selection was decided through in-depth discussions with enrolled patients after detailed explanation about advantages and disadvantages with each graft type.
In our study, regardless of the graft type, ACLR was performed with remnant preservation. A recent systematic review found that remnant preservation was associated with significantly better results in terms of Lysholm and IKDC scores. 46 Another review also showed that remnant preservation may have more benefits in terms of JPS than remnant excision. 10 Therefore, this may partly explain the lack of significant differences in Lysholm and IKDC scores in our study. In addition, although the OSI was better with autografts in our study, no significant difference in JPS was observed between the groups.
Limitations
Our study had several limitations. First, this was a prospective comparative study without randomization; therefore, it may have been subjected to selection bias. However, no significant differences in the baseline demographic information between the 2 groups were observed. Second, we did not compare the remnant tissue type between the 2 groups in this study. In future studies, further detailed analysis of remnant tissue morphology and type can be considered. Third, the grafts used in our study were HS tendon autografts and irradiated TA allografts; thus, our findings may not be generalizable to other autografts or allografts. Last, our follow-up period was limited to 1 year.
Conclusion
Our study demonstrated no significant differences in knee muscle strength or patient-reported outcomes between HS tendon autografts and TA allografts after ACLR with remnant preservation for up to 1 year except for dynamic postural stability favoring HS tendon autografts. However, whether this difference in dynamic postural stability translates into other clinical outcomes, such as return to sports, reinjury rate, or knee function, in the long term should be further investigated.
Footnotes
Final revision submitted May 2, 2024; accepted June 11, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the Korea Medical Device Development Fund grant funded by the Korea government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health & Welfare, the Ministry of Food and Drug Safety) (Project Number: 1475013503, RS-2023-00210209). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Anam Hospital, Korea University (2018AN0261 / K2018-0444-003).