
Abstract
Background:
Chronic ankle instability (CAI) develops in 20% to 40% of patients after ankle sprains because of inappropriate management or a premature return to sports (RTS). Patients become candidates for surgery when nonoperative treatment fails. The results of arthroscopic lateral ligament reconstruction have been shown to be excellent. However, there is no consensus on the RTS criteria in these cases. The Ankle-GO score, which has been validated in lateral ankle sprains, is an evidence-based protocol for RTS.
Purpose:
To evaluate the discriminant and predictive capacity of the Ankle-GO score for RTS after arthroscopic lateral ankle reconstruction.
Study Design:
Cohort study. Level of evidence, 2.
Methods:
This prospective multicenter cohort study, conducted between January 2022 and January 2023, evaluated patients with CAI who underwent arthroscopic anatomic lateral ankle ligament reconstruction using gracilis tendon autografts or allografts. The RTS rates at 4 and 6 months postoperatively were the primary and secondary outcomes, respectively. The evaluated variable at both timelines was the Ankle-GO score—a composite of 4 functional tests and 3 questionnaires. The study determined the discriminant validity of the Ankle-GO score for RTS at each timeline—Ankle-GO scores at 4 months for RTS at 4 months; Ankle-GO scores at 6 months for RTS at 6 months. The predictive capacity of the Ankle-GO score at 4 months for RTS at 6 months was also evaluated.
Results:
A total of 51 patients, with a mean age of 32.8 years, were included, of whom 23 (45%) had returned to sports at 4 months and 39 (76.5%) at 6 months. The mean Ankle-GO score was significantly higher in the group that returned to sports than in the group that did not (12 ± 4.7 vs 8.8 ± 4.7 at 4 months, respectively, P = .003; 16.8 ± 3.6 vs 11.3 ± 4.8 at 6 months, respectively, P = .002).
The predictive capacity of the Ankle-GO score at 4 months for RTS at 6 months was good, with an area under the curve of 0.74 (95% CI, 0.58-0.90; P = .005). The optimal threshold was 6 (sensitivity, 95%; specificity, 50%). The odds ratio of RTS when surpassing the Ankle-GO cutoff score was 18.5 (95% CI, 3-113.95; P = .002).
Conclusion:
The Ankle-GO score is effective in discriminating the RTS status at 4 and 6 months after lateral ligament reconstruction of the ankle. In addition, the Ankle-GO score at 4 months was also moderately predictive of RTS at 6 months after surgery.
Keywords
Ankle sprains are the most common osteoarticular injuries.16,27 A premature return to sports (RTS) is a possible cause of recurrence, leading to chronic ankle instability (CAI). 15 CAI is characterized by recurrent ankle sprains, persistent pain, and a feeling of giving away. An estimated 20% to 40% of patients with an initial ankle sprain develop CAI, which can significantly influence daily activities and lead to long-term functional limitations.8,12
Nonoperative treatment remains the gold standard for CAI. 1 This includes pain control, achieved by the use of nonsteroid anti-inflammatory drugs, and protected mobilization followed by physical therapy to strengthen muscles and proprioceptive retraining. 8 If nonoperative treatment fails, surgery is recommended to prevent recurrence and further cartilage damage.8,27 Arthroscopic anatomic lateral ligament reconstruction was described by Guillo et al. 13 Lopes et al 17 simplified the technique and performed a prospective study over 286 patients, including 171 who underwent anterior talofibular ligament (ATFL) and calcaneal fibular ligament (CFL) reconstruction using the gracilis tendon, who reported satisfactory functional outcomes with a low complication rate. As a result of the encouraging outcomes of arthroscopic reconstruction, the use of this technique has become more popular.3,6,18
Nevertheless, there is no composite score to assess readiness for RTS after surgical ankle stabilization. A recent review performed by Wright et al 34 found that RTS after surgery was not based on prospective criteria or patient-reported outcome measures. When the RTS criteria were mentioned, the decision was time-based and not evidence-based. 34 The timing and readiness for RTS is a major concern for athletes after ankle sprains.29,30,33 RTS may be different depending on the patient, the sport, and the level of practice (recreational, competition, or professional). A recent review of literature listed the most clinically relevant functional tests—including single-leg stance test (SLS), modified version of the star excursion balance test (mSEBT), single hop test (SHT), and figure-of-8 test (F8T)—and self-reported questionnaires—including Foot and Ankle Ability Measure (FAAM), Ankle Ligament Reconstruction-Return to Sport after Injury (ALR-RSI)— that assess patients with CAI. 21 Based on the aforementioned study, Picot et al 22 developed and validated the Ankle-GO score, which includes objective, subjective, and psychological criteria to predict RTS after an acute ankle sprain and helps clinicians to make a valid decision on RTS. They proved excellent psychometric properties (excellent test-retest reliability; intraclass correlation coefficient for repeated measure = 0.99), good internal consistency (Cronbach alpha coefficient = 0.79), and good discriminant and predictive value of the score for assessing RTS after lateral ankle sprain.
This study aimed to evaluate the discriminant validity and predictive capacity of the Ankle-GO score for RTS after arthroscopic lateral ankle ligament reconstruction.
We hypothesized that patients who returned to sports would have higher Ankle-GO scores than those who did not at 4 and 6 months. We also hypothesized that the Ankle-GO score at 4 months could predict patients who are more prone to RTS at 6 months after arthroscopic ankle ligament reconstruction.
Methods
Study Design
A prospective multicenter cohort study included all patients with CAI who underwent an arthroscopic anatomic lateral ankle ligament reconstruction at 2 centers between January 2022 and January 2023.
Patient selection was based on 3 components: history, physical examination, and imaging.
CAI was defined as recurrent ankle sprains, persistent pain, and a feeling of giving away that are refractory to 6 months of nonoperative treatment, as mentioned in the International Ankle Consortium.10,12
All candidates were examined meticulously before selection for signs of ankle stability (anterior drawer test and lateral tilt).
An imaging protocol was mandatory for all candidates to confirm the diagnosis.
Ankle radiograph (anterior-posterior, lateral, and mortise view)
Telos stress radiographs (sagittal and coronal plan)
Radiograph with a cerclage of Meary for hindfoot alignment
Ankle magnetic resonance imaging (MRI) for lateral ankle ligament (ATFL and CFL assessment).
MRI serves to assess the quality of the remaining ATFL and CFL.12,20
The exclusion criteria included patients who underwent nonarthroscopic or nonanatomic ligament reconstruction or another type of ligament repair. Patients who underwent revision surgery or additional procedures for associated injuries (osteochondral lesion of the talus, fibular tendinopathy) were also excluded. Finally, patients showing osteoarthritic changes and those with sedentary lifestyles not practicing sports were excluded.
The institutional review board approved the study. The patients gave their consent by filling out the online survey and accepting to undergo the examination at 4 and 6 months.
Surgical Technique and Postoperative Rehabilitation Protocol
The surgical technique described by Guillo et al 13 and simplified by Lopes et al 18 was used by senior surgeons (A.H. and R.L.) to operate on all patients under spinal anesthesia.
We started by harvesting the gracilis tendon. If absent, an allograft was ordered as a substitute.
An arthroscopic evaluation of the tibiotalar joint through usual anteromedial and anterolateral portals was done. Calcaneal, talar, and fibular tunnels were drilled in their anatomic position. Reconstruction of the ATFL and the CFL using double strands of the gracilis was performed. First, a 4.75 × 20–mm tenodesis screw (Arthrex) was used to secure the graft within the talus. The graft was then inserted into the fibular tunnel using an ACL TightRope RT (Arthrex). The second stump was fixed in the calcaneus with a 6 × 25–mm tenodesis screw (Arthrex) while maintaining the ankle in a neutral position and the hindfoot in valgus.
Postoperatively, patients were placed in a walking boot for 3 weeks (day and night). Full weightbearing was authorized immediately. Passive rehabilitation began early (range of motion, drainage), with active rehabilitation starting after 3 weeks.
RTS was progressively allowed; its timeline varied according to the sport’s nature, with noncontact/nonpivot sports, such as cycling and swimming, allowed at 3 months and pivot/contact sports at 6 months after surgery.
Outcome Measures and Evaluation
The primary outcome measure of the study was the RTS rate at 4 months postoperatively. The primary evaluated variables were the Ankle-GO scores collected at 4 months postoperatively.
The secondary outcome measure was the RTS rate (rate and quality) at 6 months postoperatively. The secondary evaluated variables were the Ankle-GO scores collected at 6 months postoperatively.
In both timelines, the evaluation focused on determining the discriminant validity of the Ankle-GO score for RTS at the respective timeline—Ankle-GO scores at 4 months for RTS at 4 months; Ankle-GO scores at 6 months for RTS at 6 months. For this analysis, patients were categorized into 2 groups at each timeline, depending on their RTS status: those who returned to sports and those who did not.
The predictive capacity of the Ankle-GO scores at 4 months for RTS at 6 months was also evaluated. This timing was based on the study performed by Bouveau et al 3 who showed a median time to RTS at 6 months. Two months prior was statistically sufficient to determine the predictive capacity of the Ankle-GO score.
Ankle-GO Score
The Ankle-GO score is a composite score composed of 4 objective functional tests and 3 subjective questionnaires, each weighted according to their level of evidence (Table 1). The overall score ranges from 0 to 25, with a higher score indicating greater functional capability. 22
List of Tests and Questionnaires of the Ankle-GO a

ADL, activities of daily living; ALR-RSI, ankle ligament reconstruction-return to sport after injury; ANT, anterior; FAAM, foot and ankle ability measure; F8T, figure-of-8 test; mSEBT, star excursion balance test; PM, posteromedial; SHT, side hop test; SLS, single-leg stance test.
The 4 functional tests are illustrated in Figure 1 and include the following:
SLS test on a firm surface 25 : The patient must stand on a single barefoot (unipedal on the injured side) support, with both hands on hips, knee slightly flexed, and eyes closed for 20 seconds. Losing the original position was signaled as an error.
mSEBT10,23,26: The patient must stand barefoot on the tested foot in the center of a “Y” formed by 3 branches. The patient must reach as far as possible with the opposite leg in the 3 directions: anterior, posteromedial, and posterolateral, then return to the initial position.
SHT 7 : This test requires hopping laterally and medially on the injured ankle 10 times as quickly as possible between 2 lines spaced 30 cm apart.
F8T 4 : This test involves skipping in Figure 8 around 2 posts 5 m apart as fast as possible.
Caffrey et al 4 highlighted the importance of the subjective feeling of stability in patients with a lateral ankle sprain (LAS) or CAI. At the end of each test, patients were asked if they experienced any instability. If the answer was “No,” an additional point was awarded.

A picture illustrating the functional performance tests (Picot et al 21 ).
Three self-reported questionnaires were added to form the score:
A. FAAM-Activities of Daily Living (21 items)
B. FAAM-Sports Activity (8 items)
The weight of each test was adapted in relation to the level of evidence, which explains, for example, the high number of points assigned to the mSEBT.
Data Collection
Data were collected prospectively through an internet-based software, Websurvey, which was accessed and filled out by surgeons for physical examination and surgical technique, by physical therapists for functional testing, and by patients for demographic characteristics and questionnaires.
The Ankle-GO assessment was performed at 4 and 6 months postoperatively by 1 single experienced physical therapist (B.P., G.R., F.F. and K.A.) trained in assessing each of the functional tests. Patients were also asked if they had returned to sports at any level of practice with a “yes” or “no” answer. RTS was based on the patients’ perception of their performance by comparing it to their preoperative status. By choosing “yes” as an answer, patients were included in the RTS group. In addition, patient characteristics, type of sport, and preoperative information were collected.
Participants
During the study timeframe, 62 patients were operated for CAI. Of them, 4 were excluded because of the presence of associated cartilage damage, 2 were excluded because they had revision surgeries, and 5 were lost to follow-up. The final study sample size was 51 patients.
Statistical Analysis
Means and standard deviations were used to describe quantitative variables. The frequencies and percentages were used to describe dichotomous variables. The discriminant capacity of the Ankle-GO score between the group that returned to sports (RTS group) and the group that did not (non-RTS group) was evaluated by a paired t test. Cohen d values were reported to measure the effect size, where 0.2, 0.5, and 0.8 represented small, moderate, and large effects, respectively.
The predictive capacity of the Ankle-GO score at 4 months to determine RTS at 6 months was evaluated by the receiver operating characteristic curve statistics. The area under the curve (AUC) score can range from 0 to 1. A score of 0.5 indicates random guessing, and a score of 1 indicates perfect performance. The Youden index J, J = Sn – (1 – Sp), was used to calculate the optimal cutoff with the corresponding sensitivity and specificity.
Statistical significance was set at P < .05.
A logistic regression analysis was performed to examine the influence of surpassing the cutoff of the Ankle-GO score at 4 months on RTS at 6 months to determine the odds ratio of RTS.
All statistical analyses were performed using R software Version 4.2 (R Core Team).
Results
Patient Characteristics
A total of 51 patients (28 women and 23 men), with a mean age of 32.7 ± 11.9 years, were included. One patient was a professional athlete (2%), 21 practiced competitive sports (41%), and 29 were recreational and occasional athletes. Patient characteristics and the distribution of the patients’ usual sports are summarized in Table 2.
Baseline Characteristics of the Study Population a
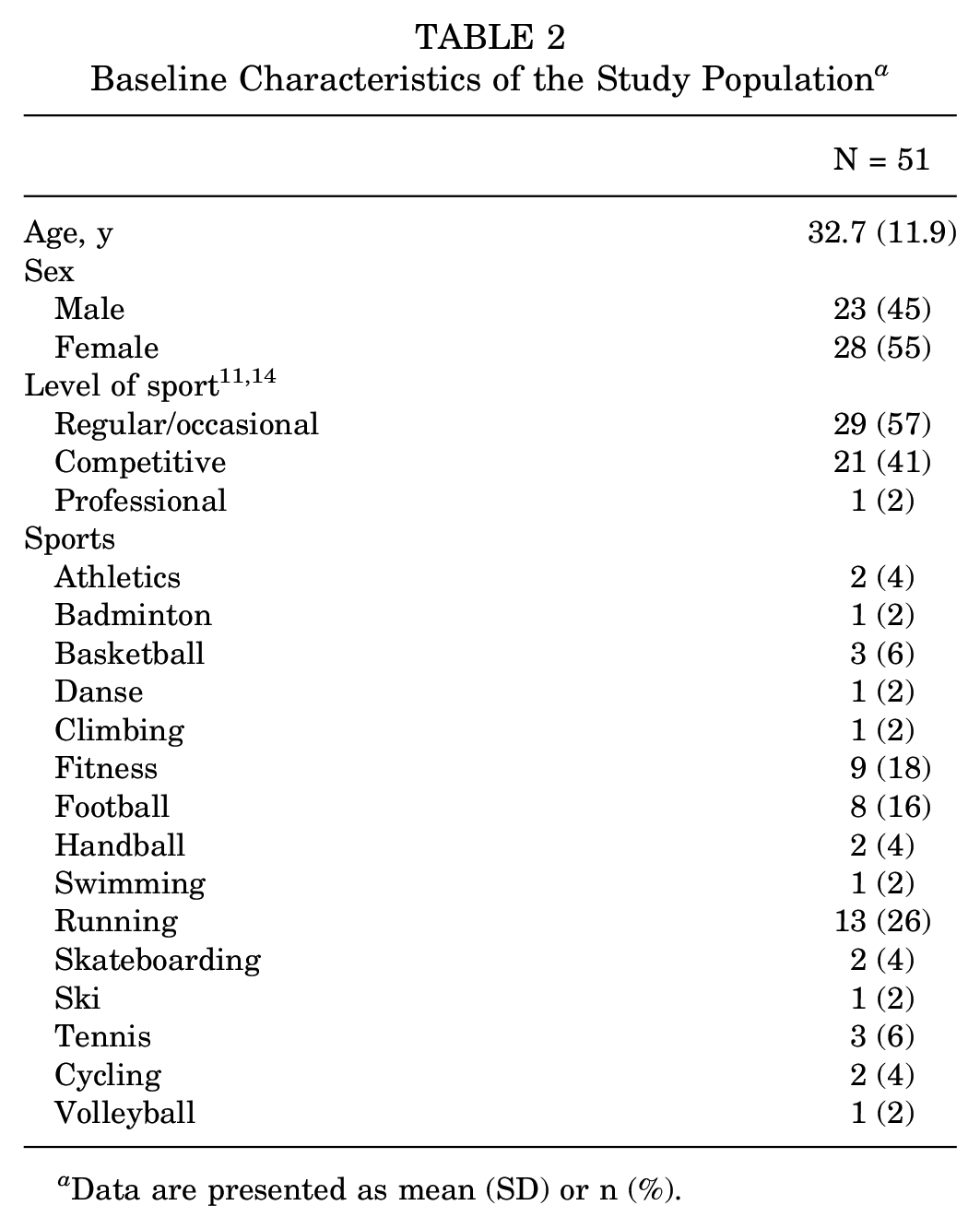
Data are presented as mean (SD) or n (%).
Return To Sports
At 4 months postoperatively, 45% of the patients had returned to sports. This rate increased up to 76.5% 2 months later (Table 3).
Discriminant Validity of the Ankle-GO Score for RTS a
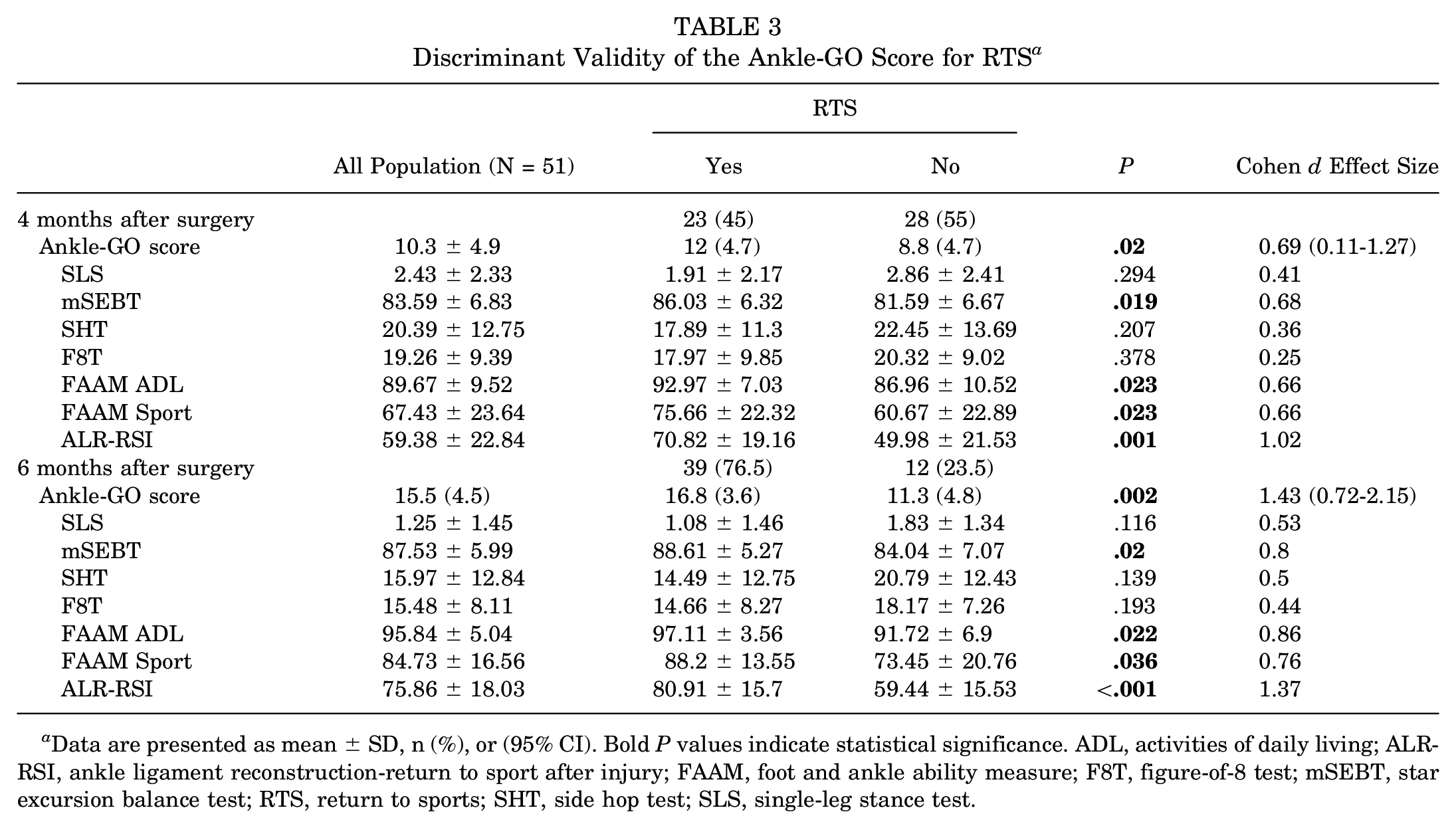
Data are presented as mean
No significant difference was found between in-line and pivot sports in terms of RTS (Table 4).
In-line Versus Pivot Sports a
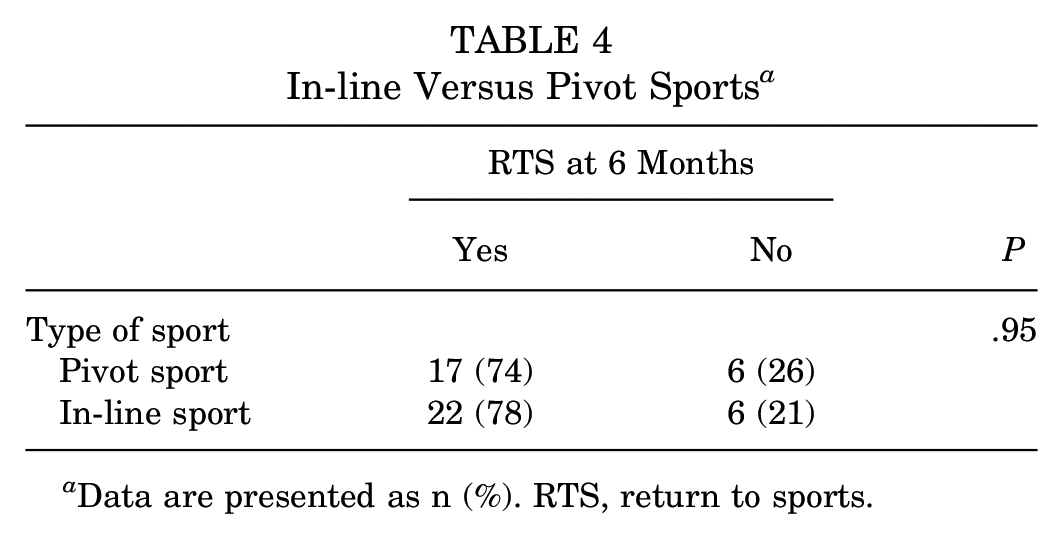
Data are presented as n (%). RTS, return to sports.
Discriminant Validity of the Ankle-GO Score at 4 and 6 Months
At 4 months postoperatively, the mean Ankle-GO score for the entire group was 10.3 (SD, 4.9) points. Those who returned to sports had a significantly higher Ankle-GO score (12 vs 8.8; P = .02) (Table 3). The Cohen d effect size was 0.69, indicating a moderate effect (95% CI, 0.11-1.27).
The raw scores for the Ankle-GO components are presented in Table 5.
Ankle-GO Scores at 4 and 6 Months a

Data are presented as mean ± SD (range). ALR-RSI, ankle ligament reconstruction-return to sport after injury; ANT, anterior; COMP, composite; FAAM, foot and ankle ability measure; F8T, figure-of-8 test; mSEBT, star excursion balance test; PL, posterolateral; PM, posteromedial; RAW, measurement according to the test score; Score, measurement according to the Ankle GO contribution; SHT, side hop test; SLS, single-leg stance test.
At 6 months postoperatively, the mean Ankle-GO score increased to 15.5 (SD, 4.5) points for all participants. Patients who returned to sports (16.8 [SD, 3.6]) had a more pronounced scoring than those who did not (11.3 [SD, 4.8])—reflected in P = .002. A large effect size was manifested by Cohen d effect size (Cohen d =1.43).
Predictive Capacity of the Ankle-Go Score at 4 Months for RTS at 6 Months
The predictive capacity of the Ankle-GO score at 4 months for RTS at different levels at 6 months was fair, with an AUC of 0.74 (95% CI, 0.58-0.90; P = .005) (Figure 2). The Youden index was 0.45, corresponding to an optimal cutoff of 6 points with a sensitivity of 95% and a specificity of 50% for a prediction of RTS at 6 months.

ROC curve for the Ankle-GO score for predicting no RTS. ROC, receiver operating characteristic; RTS, return to sport.
The odds ratio of RTS when surpassing the Ankle-GO cutoff score was 18.5 (95% CI, 3-113.95; P = .002).
Discussion
Our main finding is that the Ankle-GO score has good discriminant validity for RTS after arthroscopic lateral ankle ligament reconstruction. Moreover, this study demonstrated a moderate predictive value of this score at 4 months for RTS at 6 months, regardless of the level of practice (recreational, competition, or professional).
Picot et al 22 applied the Ankle-GO on 64 patients after an acute LAS treated nonoperatively at 2 and 4 months and showed a good discriminant validity with a minimal detectable change (MDC) of 1.2 points. They also have displayed a good predictive ability to RTS.
In our study, we were able to prove its predictive ability to RTS after an arthroscopic lateral ankle ligament reconstruction. However, it lacks a group control to determine its MDC.
The Ankle-GO increased by 5 ± 3.2 points between 4 and 6 months in our study. The same pattern of improvement was seen in Picot et al 22 study—the Ankle-GO score was raised by 6.4 points between 2 and 4 months after LAS. However, both groups had a lower score at their last follow-up than the control group.
The Ankle-GO score at 4 months in our study was 10.9 points after reconstruction compared with 14.2 points after LAS reported by Picot et al 22 at the same time. This suggests that the score progresses more slowly after surgical reconstruction than after nonoperative treatment of LAS. CAI is more aggressive than LAS, and the healing process is usually longer after an intervention; hence, RTS may take a longer time. Based on the Ankle-GO, the performance of the patients in our study at 6 months was lower than that of the control group studied by Picot et al 22 (19.6 points). It would be interesting to evaluate patient's performances after a longer follow-up.
Moreover, the predictive value of the Ankle-GO score at 4 months for RTS at 6 months was also confirmed. Our cutoff level at 4 months was 6 points. Clinically, patients who recorded a score of >6 points at 4 months after the reconstruction were more likely to RTS at 6 months. When surpassing this score, the odds of RTS will multiply 18 times. In comparison, Picot et al 22 showed that an Ankle-GO score at 2 months predicts RTS at 4 months after LAS, but their cutoff level was 8 points. The sensitivity of the cutoff was better (95% vs 72%) in our study. However, specificity is only 50%, which is considered low. The positive predictive value (PPV) is 86%, indicating that 86% of those who score above 6 points at 4 months will successfully return to sports at 6 months. In addition, the negative predictive value (NPV) is 75%, meaning that 75% of patients who score <6 points will not RTS. Our PPV and NPV values are considered good when evaluating a test.
The Ankle-GO preserves its predictive value to RTS despite the change of the pathology (LAS to CAI), the adapted treatment (nonoperative vs operative), and the time to RTS; however, the cutoff should be adapted for each entity.
We also found that ALR-RSI, FAAM, and mSEBT scores were significantly higher in those who returned to their practice. Based on these findings, we believe that psychological readiness— including fear of reinjury and lack of confidence—are the primary obstacles preventing patients from resuming sports. However, these factors may vary depending on the specific pathology. The Ankle-GO score aimed to create a comprehensive scoring system to assess ankle function regardless of the type of injury. It was initially validated for RTS after LAS. In our study, we used the Ankle-GO to evaluate RTS after ligamentous reconstruction for CAI. Additional research is underway to validate the score for other ankle-related conditions—including Achilles tendon rupture.
A total of 39 patients (76.5%) returned to sports at 6 months in our study, which is similar to other results in the literature. For example, in a prospective study by Lopes et al 17 evaluating 286 patients—including 171 who underwent the same surgical technique—RTS at the same preinjury level was 80% for recreational athletes at 6 months. However, this rate declined to 48% in competitive athletes. In addition, Bouveau et al 3 had a similar RTS rate in 40 patients after all-arthroscopic lateral ankle ligament reconstruction. Although the follow-up in that study was 12 months, the median time to RTS was 6 months; thus, it was similar to our findings.
The originality of our study is that it validates the predictive value of the Ankle-GO for RTS at 6 months after lateral ankle reconstruction and provides an evidence-based composite test to help in decision-making. In addition, this score could help practitioners adapt their postoperative care protocols and estimate the timing of RTS. Certainly, the application of a complex composite score, such as the Ankle-GO, which necessitates 20 minutes, demands more time compared with simpler scores. However, we think that the substantial clinical advantages it provides by encompassing functional, subjective, and psychological dimensions far outweigh the benefits derived from a single test—shown by the higher Cohen index. This hypothesis remains uncertain, and future studies should be conducted to show the superiority of the Ankle-GO score.
Limitations
This study has certain limitations. In particular, the differences in demographic characteristics, sex, and level of practice in patients could create a patient bias. Better patient selection and an analysis of subgroups (recreational and professional) could provide more specific results. Another limitation includes the small sample size. In addition, the level of practice at RTS was not determined in our study. This should be reported in future studies, as this is a major concern for professional athletes who request information on their ability to RTS at the same level. Also, the initial instability is an important factor that was not evaluated. This could have an important effect on RTS, and especially on the level of practice at RTS. Finally, a minimum follow-up of 6 months is short to assess the predictive value of the score; thus, longer follow-ups are needed to assess the RTS rate after reconstruction and detect whether the rate of recurrence could be correlated with this score.
Conclusion
The Ankle-GO score is effective in discriminating the RTS status at 4 and 6 months after lateral ligament reconstruction of the ankle. At 4 months after injury, a patient exhibiting an Ankle-GO score of >6 points is likely to resume sports at 6 months.
Footnotes
Final revision submitted September 8, 2024; accepted October 1, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.H. and R.L. are educational consultants for Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from “Comité d’Ethique”– IRB (Institutional Review Board) of the Ramsay Santé Group.