
Abstract
Background:
The abnormal morphology of complete discoid lateral meniscus (CDLM) is associated with a greater propensity for tears. The magnetic resonance imaging (MRI) morphology of CDLM is most often described in the coronal plane, with few morphological studies in the sagittal position.
Hypothesis:
The sagittal anteroposterior diameter of CDLM is smaller than that of normal meniscus and is increased after tear in adults.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
The authors searched the radiology records at our institution from June 2018 to December 2023 for patients aged from 18 to 55 years with knee pain. According to inclusion and exclusion criteria, 70 knees (66 patients) with torn CDLM were enrolled as group A, 36 knees (31 patients) with intact CDLM were enrolled as group B, and 48 knees (32 patients) with normal lateral meniscus (LM) were enrolled as group C. The coronal view passing through the middle point of the lateral tibial plateau (LTP) were identified the referrence coronal view, then the sagittal view passing through the middle point of the LTP on the referrence coronal view were selected for the measurements, the anterior distance, posterior distance, and anteroposterior diameter of the LM, sagittal tibial diameter (TD) were measured. The 4 measurements and the ratios were compared among the groups by independent sample t test.
Results:
The reliability of all measurements was excellent, except that posterior distance was classified as good in group B. The anteroposterior diameter and TD were smaller in group A than in group C (both P < .001) and smaller in group B than in group C (P < .001 and P = .007). anteroposterior diameter and anteroposterior diameter/TD in group A were larger than in group B (P = .003 and P < .001), while anteroposterior diameter/TD in group A and group C were similar (P > .05). The anterior distance and anterior distance/TD were smaller in group A than in group B (P = .02 and P = .03) and smaller in group A than in group C (P < .001 and P = .008). Posterior distance, posterior distance/anteroposterior diameter, and posterior distance/TD were larger in group A than in group C (P < .001, P < .001, and P < .001) and larger in group B than in group C (P < .001, P < .001, and P < .001).
Conclusion:
Our study demonstrates that in adults, the meniscal anteroposterior diameter and the TD are smaller in CDLM than in normal LM, and the anteroposterior diameter of torn CDLM is larger than intact CDLM.
Discoid meniscus is an anatomical abnormality that mainly affects the lateral meniscus (LM) of the knee. It is more common in Asian populations.18,21 According to the Watanabe classification, discoid LM (DLM) can be divided into 3 types: complete, incomplete, and Wrisberg.14,18 Complete DLM (CDLM) is known to tear easily, mainly because the abnormal size and shape of the meniscus predisposes to abnormal biomechanics of the knee 18 and also because the meniscal collagen fiber system is disorganized and the vascularity of the inner areas is poor. 18
Magnetic resonance imaging (MRI) is the most commonly used modality for radiologic evaluation of the knee.7,16,19 MRI can distinguish the morphological characteristics of the meniscus well and has good value in the examination of injured meniscus. Most MRI observations of DLM are based on coronal views of the knee. Araki et al 3 have proposed that the minimum width of DLM on coronal MRI is >14 mm. However, Samoto et al 17 believe the critical value should be 15 mm and have also proposed that the minimum meniscal width/tibial width ratio on coronal MRI should be ≥20% in DLM, 21 while Choi et al 5 propose that in CDLM, the minimum meniscal width/tibial width ratio is ≥32%. On sagittal view, DLM is indicated by visualization of the fused anterior and posterior horns of the meniscus in ≥3 consecutive 4-mm slices.3,17
When the meniscus is compressed by the femur and tibia, it will expand to the surrounding area. This phenomenon, known as the hoop stress mechanism, plays a role in relieving stress. However, the CDLM is disc like, with the anterior and posterior horns connected from birth. 18 This leads to limited enlargement of the meniscal diameter during growth and limited expansion upon compression, especially in the anterior and posterior direction. 8 These, along with the smaller anteroposterior diameter (APD) in CDLM compared with normal LM, also recently reported by Hashimoto et al, 8 are risk factors for tear of the CDLM. However, most of the patients in Hashimoto et al’s 8 study were children, and the APD changed with age.
The purpose of the study was to observe the morphological characteristics of adult CDLM on the sagittal MRI view. We hypothesized that the meniscal APD and the tibial diameter (TD) are smaller in CDLM than in normal LM in adults, and the APD of torn CDLM is larger than intact CDLM.
Methods
All procedures involving humans were performed in accordance with ethical standards of the institutional or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Our study protocol was authorized by the local ethics committee.
Study Design
The electronic medical record was searched for patients diagnosed with CDLM in our hospital from June 2018 to December 2023. The inclusion criteria were age between 18 and 55 years with CDLM and complete MRI data of the knee in our hospital; there were 146 knees (126 patients) included. CDLM was diagnosed by calculating the ratio of the minimum meniscal width to the maximum tibial width in coronal sections, with CDLM defined as a ratio >0.32 and a normal meniscus as a ratio <0.20, according to the method established by Choi and Samoto et al.5,17 Exclusion criteria were (1) unclear, indeterminate, or defective edges of the LM on MRI (n = 22 knees); (2) knee joint degeneration with Kellgren-Lawrence grade ≥3 (n = 12 knees); and (3) CDLM complicated with knee ligament injury, fracture, or previous surgery (n = 6 knees).
Finally, a total of 106 knees (94 patients) were included. Group A consisted of 70 knees in 66 patients with torn CDLM; all patients had pain on the lateral side of the affected knee, tenderness at the lateral joint line, and mechanical symptoms including snapping (n = 16), sudden locking (n = 8), or both (n = 6). McMurray tests were positive in 30 knees and Apley compression tests were positive in 70 knees. There were 57 knees of no shift and 13 knees of central shift according to the Ahn classification, 1 and no anterocentral shift and posterocentral shift were included in the study. Group B included 36 knees (31 patients) with intact CDLM. Three patients with bilateral CDLM, with one side torn and the other side intact, were included in both group A and group B; the others in group B came from patients with torn medial meniscus and those with intact CDLM (n = 28), confirmed by MRI and arthroscopy, and without pain or tenderness along the lateral joint line of the knee. From June 2018 to December 2023, we also selected 48 consecutive knees in 32 patients aged between 18 and 55 years with normal meniscus, 30 with tendonitis, and 18 with Hoffa disease, for the control group (group C), the exclusion criteria were same to group A and group B (Figure 1).

Flowchart of the patient selection.
Imaging
All MRI measurements were performed with a Philips Ingenia 3.0 T MR scanner. Coronal and sagittal images were obtained with the patient supine and the knees fully extended, and the study measurements were performed on the sagittal images. The images were read on a picture archiving and communication system similar to the previous study. 14 The image parameters for the T2 fast spin-echo image slices were: repetition time, 2510 to 3500 ms; echo time, 81 to 85 ms; slice thickness, 2 mm; matrix 256 × 256; and visual field, 160 mm. The measurements were performed automatically to ≤2 decimal points of accuracy with the built-in line tool.
Measurements
In this study, the MRI measurements were performed by a senior surgeon (Z.D.) with 20 years of experience in orthopaedics and a junior surgeon (Y.C.) with 3 years of experience in orthopaedics, The measurements were performed in a blinded and randomized manner to determine interobserver reliability. To assess intraobserver reliability, the senior surgeon reviewed all measurements after 4 weeks. Measurements from the 2 observers were averaged and statistically analyzed with intraclass correlation coefficient (ICC).
The coronal MRI views passing through the middle point of the LTP were identified as the referrence coronal view, then the sagittal view passing through the middle point of the LTP on the referrence coronal view were selected for the measurements. The datum line was drawn referring to the anterior and posterior edges of LM, not the tibial plateau line because the lateral tibial plateau surface was curved in most cases and difficult to confirm. As seen in Figure 2, a line was drawn connecting the middle point of the anterior edge of the LM (b) and posterior edge of the LM (c). Then vertical lines perpendicular to the anteroposterior line of the LM were drawn from the anterior-most point of the tibia and the posterior-most point of the tibia, and the cross-points were labeled a and d. The distance from the anterior edge of the meniscus to the anterior edge of the tibia (ab) was recorded as the anterior distance (AD). The distance from the posterior edge of the LM to the posterior edge of the tibia (cd) was recorded as the posterior distance (PD). The distance from the anterior edge of the LM to the posterior edge of the LM (bc) was recorded as the APD, and the distance from the anterior edge of the tibia to the posterior edge of the tibia (ad) was recorded as the TD.

Meniscal measurements in the midcoronal and midsagittal planes. The cross-point of the vertical line perpendicular to the anteroposterior line of the LM from the anterior-most point of the tibia (a). The middle point of the anterior edge of the LM (b). The middle point of the posterior edge of the LM (c). The cross-point of the vertical line perpendicular to anteroposterior line of LM from the posterior-most point of the tibia (d). AD, anterior distance; APD, anteroposterior diameter; LM, lateral meniscus; PD, posterior distance; TD, tibial diameter.
Statistical Analysis
All data were statistically analyzed by using SPSS software (Version 26.0; IBM). The quantitative data were expressed as means ± SD, and the age of each group was compared by 1-way analysis of variance, while the sex and knee joint sides were compared by chi-square test. The test-retest reliability was assessed by using the ICC with a 2-way mixed model and with absolute agreement. An ICC >0.900 meant excellent agreement and 0.750 to 0.900 meant good agreement. The comparison of the measurements and ratios (AD, PD, APD, TD; AD/APD, AD/TD, PD/APD, PD/TD, and APD/TD) among groups was conducted by independent-samples t test. A P value <.05 was considered significant.
The sample size was estimated utilizing MedSci sample size tools (Version 2.1; MedSci). The accepted α error was .05, and the β error was 0.2 to ensure a power of 80%. APD was used in the sample size calculation. At least 66 knees in group A and 33 knees in group B were needed in the comparison of mean values between groups A and B, and ≥26 knees in each group were needed in the comparison of mean values between groups A and C.
Results
There were 70 knees (66 patients) with torn CDLM in group A; 36 knees (31 patients) with intact CDLM in group B; and 48 consecutive knees (32 patients) with normal LM in group C. There were no significant differences in sex, age, and side of knee joint among the 3 groups. Detailed characteristics of the study patients are presented in Table 1.
Clinical Characteristics of 3 Groups of Research Participants a

Data are presented as n or mean ± SD.
The intra- and interobserver reliability of the measurements in group A (AD, PD, and APD) was in excellent agreement (all ICC >0.900), but TD was in good agreement (ICC = 0.826 and 0.884). While in group B and group C, the intra- and interobserver reliability of all parameters were excellent (all ICC >0.900), except that the intraobserver reliability of APD was classified as good in group B (ICC = 0.865) (Table 2).
Comparison of the Intra- and Interobserver Reliability of the Measurements a

Data are presented as ICC value (95% confidence interval), ICC value of >0.90 indicates excellent agreement and >0.75 indicates good agreement. AD, anterior distance; APD, anteroposterior diameter; PD, posterior distance; TD, tibial diameter.
There was no significant difference in PD, TD, or PD/TD between groups A and B (all P > .05), while AD, AD/APD, AD/TD, and PD/APD were smaller in group A than in group B (P = .02, .007, .03, and .01), and APD and APD/TD were larger in group A than in group B (P = .003 and P < .001). AD, APD, TD, and AD/TD were smaller in group A than in group C (P < .001, P < .001, P < .001, and P = .008), and PD, PD/APD, and PD/TD were larger (all P < .001). There was no significant difference in AD/APD and APD/TD between group A and group C (both P > .05). When comparing group B with group C, PD, PD/APD, and PD/TD were all larger in group B (all P < .001), and APD, TD, and APD/TD were smaller (P < .001, P = .007, and P < .001). There was no significant difference in AD, AD/APD, and AD/TD (all P > .05). (Figure 3, Table 3). In group A, no significant difference was found in all parameters between no shift CDLM and central shift CDLM (all P > .05) (Table 4).

Measurement of the study parameters in 3 groups. (A) Torn CDLM in group A. (B) Intact CDLM in group B. (A) and (B) come from different knee of the same patient. (C) Normal lateral meniscus in group C. The anterior distance is the length ab. The posterior distance is the length cd. The anteroposterior diameter is the distance bc, and the tibial diameter is the distance ad. CDLM, complete discoid lateral meniscus.
Comparison of Measurements and Ratios in Groups a
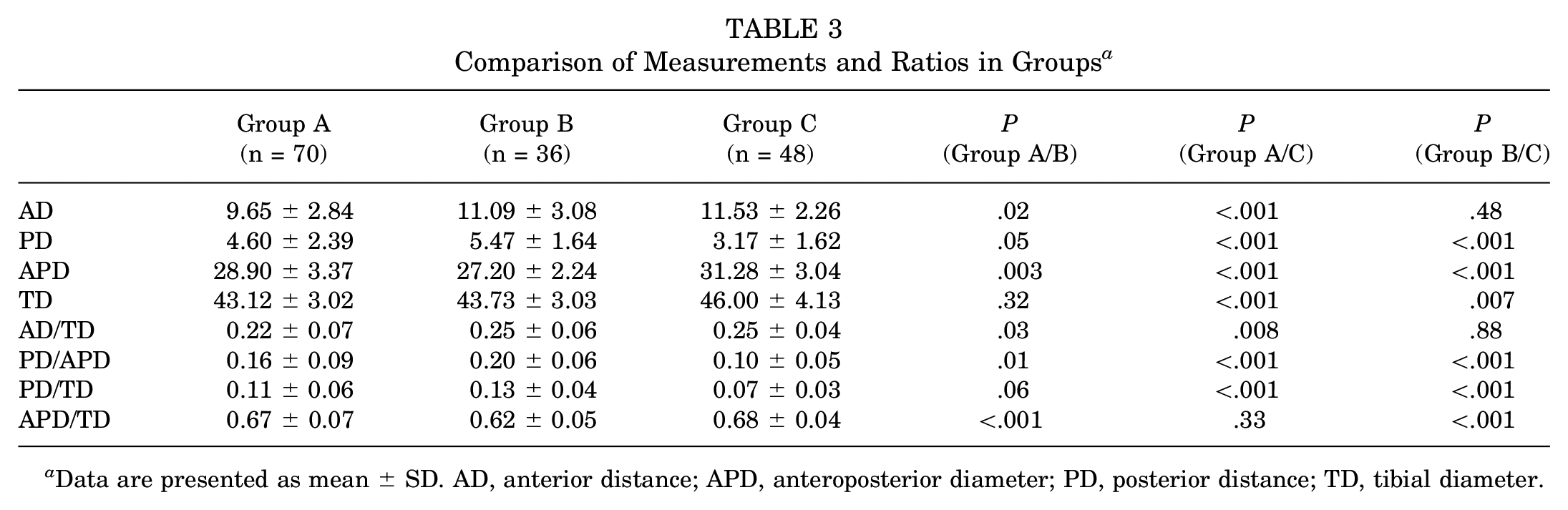
Data are presented as mean ± SD. AD, anterior distance; APD, anteroposterior diameter; PD, posterior distance; TD, tibial diameter.
Comparison of Measurements and Ratios in Group A a

Data are presented as mean ± SD. AD, anterior distance; APD, anteroposterior diameter; PD, posterior distance; TD, tibial diameter.
Discussion
The most important findings of this study were that (1) the APD of the LM and the TD is smaller in CDLM than in normal LM in adults (APD, 27.20 ± 2.24 vs 31.28 ± 3.04; TD, 43.73 ± 3.03 vs 46.00 ± 4.13; APD/TD, 0.62 ± 0.05 vs 0.68 ± 0.04) and (2) the APD of torn CDLM is larger than intact CDLM (APD, 28.90 ± 3.37 vs 27.20 ± 2.24; APD/TD, 0.67 ± 0.07 vs 0.62 ± 0.05).
The discoid shape does not conform well to the curved femoral condyle. Histologically, the circular collagen fibers in the DLM are sparse and disordered and are found in 7 symmetrical layers, each with its own fibrillar orientation. The medial middle zone of the central layer has an irregular arrangement of collagen, and the vascularity of the inner areas is poor.6,18 These are all possible reasons why a CDLM is more prone to tearing.
In a normal knee, the concave meniscus matches the curved structure of the femoral condyle, and the meniscus expands to disperse the stress at the knee in weightbearing. The hoop stress mechanism restricts excessive expansion, not only maintaining the function of the meniscus, but also preventing meniscal injury. 18 CDLM is not well matched with the curved femoral condyle. Compressive stress is distributed unevenly across the meniscus, and the local compressive stresses are obviously increased. Under the condition of weightbearing, the body of the CDLM bears the maximal stress, and during flexion and extension of the knee, the contact position between the femoral condyle and the meniscus is constantly changing, which will produce separation stress between the upper and lower layers of the CDLM.
Our study found that the APD and the APD/TD ratio in intact CDLM are smaller than those in normal LM on sagittal MRI, indicating that the APD of CDLM is significantly smaller than that of a normal LM in adults. It is possible that the smaller APD in CDLM is inherent from birth because of the fusion of the anterior horn and posterior horn; in addition, Hashimoto et al 8 found that there was only a limited increase in the APD of the CDLM and less than the TD during growth and that the sagittal meniscal ratio decreased with age. As the APD of CDLM is smaller than that of the normal LM, the mean stress of the meniscus under the same load is relatively higher than the stresses on normal meniscus.
The smaller APD in CDLM (compared with the normal LM) is accompanied by decreased circumferential expansion during compression because of the fusion of the anterior and posterior horns. 15 During flexion and extension, the CDLM must have a larger anteroposterior shift than the normal LM to suit the kinematic state of the knee, 9 which could explain the high incidence of anterior and posterior peripheral rim instability in CDLM. Klingele et al 13 observed posterior rim instability at a rate of 28.1% in DLM and noted that 47.2% were unstable at the anterior-third peripheral attachment and 38.9% at the posterior-third peripheral attachment. Peripheral rim instability was significantly more common in CDLM compared with incomplete DLM. Kim et al 10 reported that both intact DLM and torn DLM had greater peripheral rim instability of the anterior horn and posterior horn than the intact LM, which was similar with Ammann et al. 2 The high incidence of anterior and posterior peripheral rim instability in CDLM was associated with a higher risk of tear.
Our finding in adults that the APD/TD is larger in torn CDLM (group A) than in intact CDLM (group B) suggests that the tear causes an increase in the APD of CDLM. These findings are in accordance with the latest report by Nishino et al, 15 although their data excluded knees aged >20 years and all cases in the symptomatic CDLM group were no shift type. The current study included 57 knees of no shift and 13 knees of central shift in group A according to Ahn classification. No significant difference was found between no shift CDLM and central shift CDLM. Maybe the enlargement of APD is realized by both tearing and shift of the CDLM. The APD/TD in torn CDLM in our study (group A) was similar to that of normal LM (group C), which was in accordance with Kim et al, 11 who reported that the preoperative sagittal ratio of a symptomatic DLM was similar to that of normal meniscus. The CDLM is more prone to tearing because of the dimished APD.
The PD, PD/APD, and PD/TD in torn CDLM (group A) and intact CDLM (group B) were larger than in normal LM (group C). This finding is in accordance with the latest report by Hashimoto, 8 indicating that the posterior horn also locates more anteriorly in CDLM than in normal meniscus during extension. The PD and PD/TD were similar between group A and group B, indicating that the posterior horn does not move posterior after tear. The AD, AD/APD, and AD/TD were similar between group B and group C, but larger in group A, indicating that the anterior horn moves anteriorly after tear, and we believe the increasing of the APD of a torn CDLM is mainly realized by the anterior shift of the anterior horn relative to the tibial plateau.
The lateral tibial plateau in patients with CDLM also exhibits anomalies. Brutico et al 4 found that the articular cartilage thickness of the lateral tibial plateau in discoid meniscus is thinner than that of nondiscoid meniscus, and the studies by Xu et al 20 and Kinoshita et al 12 showed hypoplasia of the lateral femoral condyle and larger posterior inclination of the lateral tibial plateau in CDLM compared with normal meniscus. We found that the TD of the lateral tibial plateau in CDLM was significantly smaller than that of normal meniscus. This may affect the outward expansion of CDLM during growth and development, which would be one of the reasons for the smaller APD in CDLM.
Limitations
Our study has limitations. First, the sample size was small, and the information was collected from a single hospital only. Our conclusions have not yet been confirmed by a large multicenter study. Second, the MRI slice thickness was 2 mm, which may have introduced bias between the selected midcoronal and midsagittal level for measurement and the middle position of the tibial plateau. Third, most of the patients in group B had torn medial meniscus and degeneration of the knees, which would affect the measurements of CDLM.
Conclusion
Our study demonstrates that in adults, the meniscal anteroposterior distance and the TD are smaller in CDLM than in normal LM, and the anteroposterior distance of torn CDLM is larger than intact CDLM.
Footnotes
Acknowledgements
We thank Dr. Weijie Fan for assistance in the statistical analysis of our data and preparation of figures for this article.
Final revision submitted September 25, 2024; accepted October 25, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from the Natural Science Foundation of Hunan Province (2023JJ60050) and the Health Commission of Hunan Province (20201907). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was provided from First Affiliated Hospital of South China University (No. 2018056).