
Abstract
Background:
The discoid lateral meniscus (DLM) is a common congenital abnormality of the meniscus. Tears are common, and initial treatment is often not definitive, leading to a spectrum of complications, including persistent symptoms, meniscal insufficiency, osteochondral defects, and recurrent tears potentially requiring reoperation.
Purpose:
To determine demographic, injury, and perioperative risk factors that increase the likelihood of complications and reoperation after treatment in patients with DLM.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients surgically treated for DLM from 9 institutions between 2000 and 2020 were reviewed. Data on demographics, presenting symptoms and signs, surgical findings and treatments, complications, and reoperations were collected and analyzed using a 2-level generalized linear mixed model. The conditional probability of complications was predicted using logistic regressions. Odds ratios were calculated to identify findings associated with an increased likelihood of postoperative complications and reoperations.
Results:
In total, 867 knees in 784 patients were surgically treated for DLM. There were 175 complications in 139 knees (16%); reoperations were performed in 110 knees (13%). Complication rates varied among institutions, ranging from 0% to 29%. The most common complication was retear of the meniscus (12%). Female patients were more likely to have complications and reoperations than male patients. Patients with a meniscus tear were 74% less likely to have a complication than those without tears, although patients with a complex meniscal tear were 3.4 times more likely to have a complication and 4.4 times more likely to have a reoperation than those without. Horizontal tears, as well as the open repair technique, had an increased risk of reoperation. Other tear types, tear locations, repair techniques, the presence of rim instability, age, and preoperative symptoms were not significantly associated with complications.
Conclusion:
Of the patients, 17% (16% of knees) had postoperative complications after DLM treatment, of whom 17% had more than 1 complication. Additionally, 13% underwent reoperation. Complications were less likely in those treated for their DLM who had a meniscus tear and more likely in female patients and those with complex meniscus tears. Reoperation was more likely in female patients, those with a horizontal or complex tear, and those who had an open meniscus repair.
Keywords
A discoid lateral meniscus (DLM) is a common congenital abnormality of the meniscus. 21 Although the exact prevalence is unknown, largely due to the commonly asymptomatic nature of DLM, studies have shown that 3% to 5% of the US population may have this anatomic variant, with up to 20% of cases representing bilateral DLM.4,8,21 Most commonly, discoid menisci involve the lateral meniscus, although in 0.1% to 0.3% of cases, it is present medially. 28 The structure of the discoid meniscus, including its increased surface area, covering nearly half the tibial plateau, may contribute to the high prevalence of meniscus tears in surgically treated DLM.5,17,22,29 Various risk factors have been associated with symptomatic DLM, including age, sex, and race.19,23,24,26 While discoid lateral menisci are frequently asymptomatic, tears of a DLM may present with mechanical symptoms, such as locking, clicking, snapping, or knee stiffness.24,28 Saucerization with repair of unstable tears and restoration of rim stability are accepted treatments for a symptomatic DLM, although the success rates of these treatments are infrequently mentioned in the literature and vary between 80% and 90%.1,14,25 Given the small sizes of most case series of patients with DLM, associations between preoperative and intraoperative presentations, treatments, and outcomes are rarely reported. Our current work builds off the findings from a previous study by the Pediatric Research in Sports Medicine (PRiSM) Meniscus Research Interest Group, which reported on patient presentation, including preoperative symptoms and intraoperative DLM classification, the presence (or lack) of a meniscal tear, characteristics of the tear if one was present, treatment used, and incidence of postoperative complications or additional surgical procedures. 24 The purpose of this multicenter study was to examine the same study population as Sheasley et al 24 to identify demographic features, preoperative signs or symptoms, intraoperative findings, and methods of surgical treatment that were associated with increased likelihood of complications and/or reoperations.
Methods
Following institutional review board approval (STUDY00001869), we reviewed cases of patients with DLM treated at 9 pediatric hospitals in North America between January 2000 and March 2020. We included patients with a diagnosis of DLM, which was confirmed surgically with either an open or arthroscopic approach, and we excluded patients who had a presumed diagnosis of DLM by indirect means alone, as opposed to direct visualization, such as patients with magnetic resonance imaging findings suggestive of DLM who did not undergo surgical intervention. We used International Classification of Diseases, 9th and 10th Revisions, to search patient databases to build our cohort and searched for Current Procedural Terminology codes for arthroscopic or open treatment of the meniscus. From patient records and operative reports, we collected data for age, sex, DLM laterality, preoperative symptoms and signs, classification (morphology and stability), tear presence and type, surgical treatment, complications, and surgical retreatment. Complications included persistence of preoperative symptoms (eg, popping, locking, clicking, stiffness, swelling, pain, or feelings of instability), tear of the meniscus (either retear or new tear), parameniscal cyst formation (likely a sign of persistent or recurrent meniscus tear), development of genu valgum, arthrofibrosis, painful implants, meniscal insufficiency requiring meniscal transplant (as assessed by the treating surgeon at the time of reoperation), synovitis, patellofemoral syndrome, osteochondral defect, or anterior cruciate ligament (ACL) disruption.
Statistical Analysis
Means with ranges were calculated for continuous variables, and counts with proportions and median values were calculated for categorical variables. Correlations were analyzed by 2-level generalized linear mixed models. The conditional probability of complications and reoperations was predicted using logistic regression. The Wald test was used to assess the significance of fixed effects, where P < .05 was considered statistically significant. Odds ratios were calculated to identify findings that predicted increased likelihoods for postoperative complications and reoperations.
Results
A total of 867 knees in 784 patients were included in this study. Of the 784 patients, 442 (56%) were female. Mean age at diagnosis of DLM was 12 ± 3.7 years (range, 1-22 years), with a mean follow-up of 22.6 months (range, 0-154 months). DLMs were complete in 420 knees, incomplete in 281 knees, and not specified in 166 knees. In total, 175 complications were reported in 139 knees (16%). Complication rates varied among institutions, ranging from 0% to 29% (median, 22%), but the estimated likelihood of complications occurring for an average individual in an average hospital was 7%. Of the knees with complications, 116 knees (83%) had 1 complication, while 23 knees (17%) had >1 complication. The most common complication was a retear or new lateral meniscus tear in 100 knees (12%). A total of 110 knees (79% of knees with complications) underwent reoperation, most commonly arthroscopic partial lateral meniscectomy (in 60 knees, 55%) or meniscus repair (in 40 knees, 36%). Overall, the most common reoperations were repeat arthroscopy for partial meniscectomy (7%) or meniscal repair (5%) but less commonly included hemiepiphysiodesis, meniscal transplant, cartilage procedures, or manipulation under anesthesia.
The modeling of 24 potential risk factors for complications revealed that female patients had a higher likelihood of complications (odds ratio [OR], 2.2; P = .01). Although the presence of a meniscus tear was associated with decreased likelihood of complications (OR, 0.3; P = .03), the presence of a complex tear conferred a higher likelihood of complications (OR, 3.4; P = .02). There was no statistically significant association between increased complications and age, discoid morphology (complete vs incomplete; OR, 1.09; P = .37), tear location, rim instability, repair technique, or preoperative symptoms (Figure 1). Confidence intervals and P values are provided in Table A1 of the Appendix.
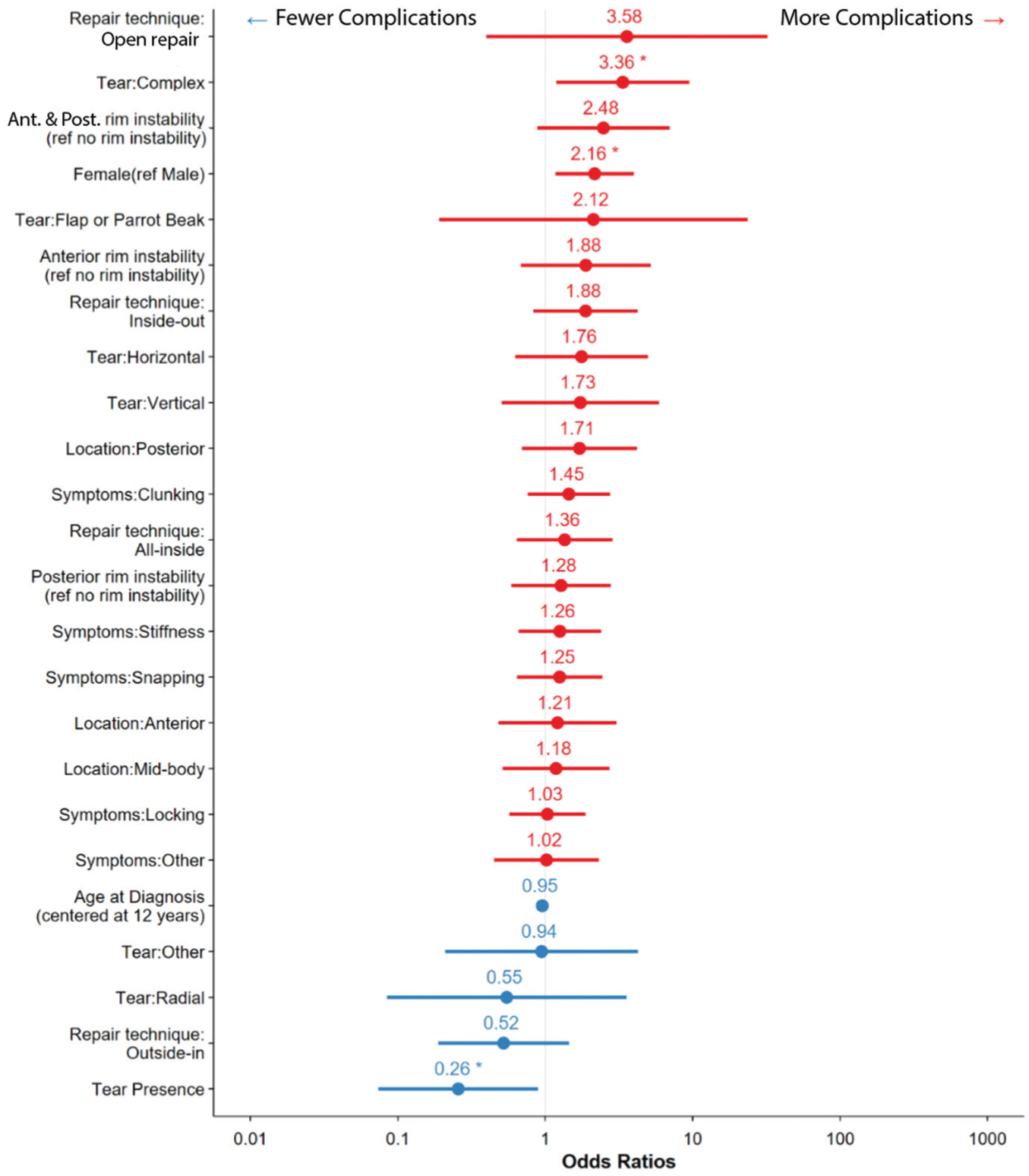
Odds ratios with 95% confidence intervals for complications by predictor.
When these same 24 predictors were evaluated as risk factors for reoperation, female patients were again found to have a statistically significantly higher likelihood of reoperation (OR, 2; P = .02) (Figure 2). A horizontal tear (OR, 2.9; P = .03) or a complex tear (OR, 4.4; P = .003) of the DLM, as characterized by the operative report, also increased the likelihood of reoperation. Finally, an open repair technique, as opposed to an arthroscopically assisted technique, increased the likelihood of reoperation (OR, 19.5; P = .02). Confidence intervals and P values are provided in Table A2 of the Appendix.

Odds ratios with 95% confidence intervals for reoperation by predictor.
Discussion
We found that female patients and patients with complex DLM tears had a higher likelihood of complications and reoperations. Having a meniscal tear was associated with a lower odds of complication, unless the tear was identified as complex. We also found that horizontal tears and open surgical meniscal repairs were associated with a higher likelihood of reoperation.
Tear Presence, Characteristics, and Repair
Sheasley et al 24 reported that meniscal tears were present in 76% of patients with DLM who underwent surgical treatment, and 11% of all patients had multiple tears. Of the patients, 50% had posterior meniscal tears, whereas 42% and 30% had tears of the body or anterior meniscus, respectively. 24 Most commonly, tears were classified as complex (38%) or horizontal (34%). Recent literature reports that 63% of surgically treated DLM cases have an associated meniscal tear, lower than our reported 76%, but has similarly shown a high incidence of horizontal and complex meniscal tears.14,16 Our data showed that the presence of a meniscal tear at index surgery was associated with lower odds of postoperative complications. We suspect that the presence of a meniscal tear provided an explanation for preoperative symptoms, whether it be pain or mechanical in nature, and served as an actionable pathology with a clear option for surgical management. Compared to symptomatic patients without a meniscal tear, patients with tears who underwent saucerization with or without repair would be expected to have improvement in their symptoms postoperatively. Conversely, patients without a tear but with pain who underwent surgery may not note a significant difference in their symptoms postoperatively. We recommend careful counseling of patients and families that surgical intervention may not resolve their symptoms, especially if no tear is found. Orthopaedic providers should consider this when indicating patients with DLM for surgery—perhaps too often, the choice is made to surgically manage patients with pain as their only symptom in the setting of DLM, with the hope that saucerization will relieve their pain. Our data suggest that operative management for these patients may not lead to an improvement in their symptoms. Caution should be employed when counseling patients regarding the likelihood of pain relief with arthroscopic management if no meniscal tear or rim instability is suspected. It is worth noting that while we included pain as a complication in our analysis, some readers may view pain as more of a reflection of patient satisfaction as opposed to a true postoperative complication.
In contrast, the presence of a complex or horizontal tear of the DLM was associated with increased odds of postoperative complications and need for reoperation compared with other tear patterns. Logan et al 14 retrospectively reviewed 470 pediatric cases of symptomatic DLM and found horizontal and complex tears were common, seen in 36% and 27% of patients, respectively, and that among the 66 patients who required reoperation, 62 of these (94%) had a retear of their remnant meniscus, with horizontal tears being the most common pattern, observed in 40%, although associations between original tear type and retears were not specified.
Nearly all (98%) of our patients with symptomatic DLM underwent saucerization or partial meniscectomy, with repairs performed in 42% of patients (55% of patients with tears; 45% of patients with tears did not undergo repair). 24 Information on whether tears extended into the remaining rim of meniscal tissue after saucerization was not collected. The most frequently repaired tears were complex tears; 51% of repairs were all-inside, 33% were outside-in, and 32% were inside-out, with 16% of procedures using a combination of the above. Of note, we did find that open meniscal repairs were associated with significantly increased odds of reoperation, with an OR of 19.50 (P = .023), greater than any of the other 24 predictors of risk that were assessed. Historically, many pediatric patients with symptomatic DLM were treated with total meniscectomy, but this has fallen out of practice in the past 30 years due to increased risk of progression of osteoarthritis and known poor long-term outcomes after total meniscectomy.1,8,9,13,27,31 Regardless, recent literature has shown that a small subset of patients still undergo more aggressive debridement of their meniscus, with Silverstein et al 26 reporting an 8.4% incidence of patients in their cohort undergoing subtotal meniscectomy in at least 1 location of the meniscus, and another 7.3% requiring >50% meniscal width resection in at least 1 location. We did not collect information on the extent of subtotal meniscectomies that may have been performed in these patients.
Bauwens et al 3 retrospectively reviewed unstable DLM treated with meniscal repair and found that 11 of 57 knees sustained a retear occurring at a median of 42 months after surgery, with 10 that underwent reoperation. All patients had undergone arthroscopic suture repair without any additional meniscal resection, and all but 2 had retears at the same locations as the index tears, believed to be secondary to failure of the primary repair. As we found, the location of DLM instability did not affect the risk of complication or reoperation for failed index repair. The 18% reoperation rate reported by Bauwens et al 3 is not dissimilar to our rate of 13% or to that of Logan et al 14 at 17%, although Sabbag et al 22 reported a 59% rate of retear at 8 years after index surgery.
Sex Differences in Pediatric Knee Injuries
We found that female patients have a higher likelihood of both complications and reoperations. Female sports participation has increased since the initiation of Title IX in 1972, but there is still a 2:3 ratio of female and male participants in youth athletics. 12 A 2013 national database estimated that of over 46.5 million youth sports participants, 3.5 million sustain a sports-related injury every year, and of these, roughly half are due to overuse.7,30 Literature has shown a higher rate of injury in female youth sports participants than their male counterparts.6,18 The reason for the higher incidence of sports-related injuries in the female population is multifactorial, with contributions from hormonal and physiologic differences, discrepancies in innate flexibility, and anatomic factors such as mechanical alignment and size, but broader societal disparities also may have an impact. 6 In their review of gender and sex differences affecting injuries in pediatric athletes, Edison et al 6 postulate that while there has been tremendous progress in terms of female participation in sports, there still remain differences in access to injury prevention and performance-enhancing resources, referencing a recent example of the 2021 National Collegiate Athletic Association basketball tournament setup between the male and female competitions, exposing obvious differences between training facilities and nutritional resources. Thus, while there are physiologic differences between male and female athletes, notable disparities between the experiences of female and male athletes may contribute to injury risk. Powell et al conducted an observational cohort study and found that female athletes were not only more likely to injure their knees but were also more likely to require surgery for the injuries they sustained. 18 Interestingly, in a later study, Rosenberger et al 20 examined nonpediatric patients who underwent arthroscopic partial meniscectomy and found that female patients had worse postoperative knee function and delayed time to maximal recovery compared to their male counterparts; additionally, preoperatively self-reported low fitness and prior knee injuries were associated with delayed recovery for females but not males. Male patients recovered faster, and male patients who were less fit preoperatively improved more than equally unfit female patients. In our study, we found that female patients had a higher likelihood of both complications and reoperations—perhaps these results can be explained by differences in preoperative knee function or self-reported physical fitness, resulting in more modest improvements after surgery in female youth athletes. If our female study participants also experienced a delay to maximal improvement postoperatively, this could in part explain a higher reported rate of complications within our study follow-up period, such as prolonged pain or stiffness, which could simply be the result of a longer recovery period as opposed to a true complication. It currently remains unclear why female patients had a higher risk of reoperation, but if they were at higher risk of prolonged postoperative pain and stiffness, their surgeons may have felt that a revision repair or manipulation under anesthesia was warranted within the study follow-up period. In the Rosenberger et al 20 study, female patients did ultimately achieve the same level of postoperative knee function as males; it simply took longer to reach the same level of improvement.
Peripheral Rim Instability
In our study, we did not find peripheral rim instability to be a risk factor for complications or reoperation. Mechanical symptoms in the setting of DLM are thought to be caused by peripheral rim instability or peripheral tears, such that the meniscus is insufficiently anchored.2,8,10,11 Peripheral rim instability is more common when a DLM is complete and has been shown to be present in 28% to 51% of patients treated arthroscopically for DLM, with most cases involving insufficiency of the anterior-third peripheral attachments (32.5%-47.2% of patients), followed by the middle third (10%-38.9% of patients) and the posterior third (11.1%-30.0% of patients).2,10 Notably, almost 30% of cases can have both anterior and posterior peripheral rim instability. Some authors urge the intraoperative evaluation of the presence of rim instability and repair, even if there is no visible tear, to avoid the risks of postoperative increased tibiofemoral contact pressures and rotational instability, which could occur in the setting of excessive mobility of the lateral meniscus.2,10,15,21 Surgeons can use all-inside or inside-out repair techniques for stabilization of the posterior or middle regions of the meniscus or an outside-in approach to stabilize anterior rim instability or tears. 28 In our cohort, 28% of knees demonstrated peripheral rim instability, similar to rates previously reported in the literature. However, we found that the presence of anterior or posterior (or combined) rim instability was not associated with higher odds of complication or reoperation. One explanation could be that cases of peripheral rim instability were correctly identified and the hypermobile meniscal segments appropriately secured, reducing the risks of persistent mechanical symptoms that could lead to reoperation.
Limitations
A major limitation of this study is its retrospective nature. Although we identified significant associations between certain patient characteristics and risks of complications, we cannot conclude that cause-and-effect relationships existed. Data collected from patient records likely underrepresented the true prevalence of complications, as the mean follow-up period was only 23 months (range, 0-154 months), which certainly resulted in many missed complications and reoperations. With the wide scope and contribution of data from 9 children’s hospitals in North America, there was also inconsistency with the reporting of complications and reoperations; 2 centers likely underreported their complications and reoperations, and other centers had limited descriptions of the nature of complications or the indication for reoperation. Although the 20-year collection period ensured a large sample size, it did not reflect improvements in surgical technique over time and may have resulted in higher reported complication and reoperation rates than what may have been seen with a shorter, more recent collection period. Furthermore, assignment of tear patterns was determined by tear characterization in the operative report, possibly introducing ambiguity or overlap in the assignment of tear patterns, which could have impacted the higher complication and reoperation rates associated with complex tear patterns. Open repair was performed in a few cases (7 patients from 2 centers) and was potentially required by the complexity of the repair. As mentioned above, we also included pain as a complication, although some might view this as a reflection of patient dissatisfaction as opposed to a true complication. Our rate of complication may also have been affected by our inclusion of patellofemoral syndrome and ACL injuries as complications; although a DLM is not a direct cause of ACL injury or patellofemoral dysfunction, the presence of a discoid meniscus results in abnormal knee morphology, and we believed it was reasonable to list all reinjuries or conditions that may have been related to original discoid pathology or otherwise altered knee biomechanics. Additionally, development of osteochondritis dissecans is a known risk associated with arthroscopic management of DLM in younger patients, especially those who have undergone a subtotal meniscectomy. In our cohort, 17 patients went on to require reoperation for either minor or major cartilage-addressing procedures, but it was unclear if these were all for osteochondritis dissecans lesions that occurred as a sequela of their DLM.
Despite our identification of increased complications and reoperations in female patients, we did not break down each type of complication and reoperation to assess whether being female increased the risk of that particular complication or reoperation. In addition, our inclusion and exclusion criteria limited our study population to only operatively treated patients, intended to allow for the highest-quality retrospectively collected data.
Conclusion
After operative management of DLM, 17% of patients reported postoperative complications, of whom 17% had >1 complication. Of the patients, 13% underwent reoperation. Overall, our study suggests that after surgical management for symptomatic DLM, female patients and those with complex meniscal tears were more likely to have a postoperative complication, whereas the presence of a meniscal tear in general was associated with a decreased likelihood of complication. Reoperation was more likely in female patients, those with a horizontal or complex tear, and those who previously had an open repair.
Author
Suzanna Ohlsen, MD, (Department of Orthopaedic Surgery and Sports Medicine, University of Washington School of Medicine, Seattle, Washington, USA); Michelle Son, MD, (Department of Orthopaedic Surgery and Sports Medicine, University of Washington School of Medicine, Seattle, Washington, USA); Waylon Howard, PhD, (Center for Clinical and Translation Research, Seattle Children's Research Institute, Seattle, Washington, USA); Jennifer A. Sheasley, MD, (Department of Orthopedic Surgery, University of Minnesota, Minneapolis, Minnesota, USA); Emily L. Niu, MD, (Department of Orthopaedic Surgery and Sports Medicine, Children's National, Washington, DC, USA); Julia C. Kirby, MBBS, (OrthoSport Victoria, Richmond, Australia); Maya Gopalan, BS, (Center for Clinical and Translation Research, Seattle Children's Research Institute, Seattle, Washington, USA); Tyler Stavinoha, MD, (Christus Health, San Antonio, Texas, USA); Sasha Carsen, MD, MBA, (Children's Hospital of Eastern Ontario, Ottawa, OntarioN, Canada); Zachary S. Stinson, MD, (Nemours Children's Hospital, Orlando, Florida, USA); Craig J. Finlayson, MD, (Lurie Children's Hospital of Chicago, Chicago, Illinois, USA); Marie-Lyne Nault, MD, PhD, (CHU-St. Justine, Montreal, QuebecC, Canada); R. Jay. Lee, MD, (Johns Hopkins, Baltimore, Maryland, USA); Brian Haus, MD, (UC Davis Children's Hospital, Sacramento, California, USA); Daniel W. Green, MD, (Hospital for Special Surgery, New York, New York, USA); John A. Schlechter, DO, (Pediatric Orthopaedic Specialists of Orange County, Orange, California, USA); Benton E. Heyworth, MD, (Boston Children's Hospital, Boston, Massachusetts, USA); Jennifer J. Beck, MD, (Center for Spine and Orthopedics, Boulder, Colorado, USA); Jie C. Nguyen, MD, MS, (Children's Hospital of Philadelphia, Philadelphia, Pennsylvania, USA); Harman Kaur Gill, BS, (UC Davis Department of Orthopaedic Surgery, Sacramento, California, USA); Julia Y. Martin, CCRC, (UC Davis Department of Orthopaedic Surgery, Sacramento, California, USA); Bryan J. Tompkins, MD, (Shriners Hospital for Children, Spokane, Washington, USA); Jennifer Brey, MD, (Norton Children's Hospital of Louisville, Louisville, Kentucky, USA); Matthew J. Brown, MD, (Connecticut Children's Medical Center, Hartford, Connecticut, USA); Nirav K. Pandya, MD, (Connecticut Children's Medical Center, Hartford, Connecticut, USA); Shital N. Parikh, MD, (Cincinnati Children's Hospital, Cincinnati, Ohio, USA); Theodore J. Ganley, MD, (Children's Hospital of Philadelphia, Philadelphia, Pennsylvania, USA); Andrew Pennock, MD, (ady Children's Hospital, San Diego, California, USA); J. Todd R. Lawrence, MD, PhD, (Children's Hospital of Philadelphia, Philadelphia, Pennsylvania, USA); Jay C. Albright, MD, (Sports Medicine Center, Department of Orthopedics, Children's Hospital Colorado, Aurora, Colorado, USA); Stephanie S. Pearce, MD, (Nemours Children's Health, Jacksonville, Florida, USA); Aristides I. Cruz Jr., MD, MBA, (Boston Children's Hospital, Boston, Massachusetts, USA); Jeffrey J. Nepple, MD, MS, (Department of Orthopaedic Surgery, Washington University School of Medicine, St. Louis, Missouri, USA); and Jennah Mann, MD, MHCDS (Children's Hospital of Los Angeles, Los Angeles, California, USA) and Gregory A. Schmale, MD, (Department of Orthopaedic Surgery and Sports Medicine, University of Washington School of Medicine, Seattle, Washington, USA).
Footnotes
Appendix
Reoperation Model Results a

| Predictor | Reoperation | ||
|---|---|---|---|
| Odds Ratio | CI | P Value | |
| Female (ref. male) | 2.03 b | 1.15-3.58 | . |
| Age at diagnosis | 0.94 | 0.88-1.01 | .116 |
| (centered at 12 years) | |||
| Tear presence | 0.37 | 0.12-1.15 | .086 |
| Anterior rim instability | 2.4 | 0.75-7.70 | .141 |
| (ref. no rim instability) | |||
| Posterior rim instability | 1.63 | 0.61-4.39 | .332 |
| (ref. no rim instability) | |||
| Anterior and posterior rim instability (ref. no rim instability) | 2.37 | 0.84-6.68 | .102 |
| Repair technique: Open repair | 19.50 b | 1.52-250.71 | . |
| Repair technique: All-inside | 1.03 | 0.51-2.10 | .933 |
| Repair technique: Inside-out | 1.4 | 0.64-3.06 | .398 |
| Repair technique: Outside-in | 0.6 | 0.25-1.48 | .271 |
| Tear: Horizontal | 2.94 b | 1.10-7.85 | . |
| Tear: Vertical | 0.92 | 0.24-3.53 | .903 |
| Tear: Complex | 4.44 c | 1.65-11.94 | . |
| Tear: Radial | 0.31 | 0.03-3.27 | .328 |
| Tear: Flap or parrot beak | 3.7 | 0.34-39.96 | .281 |
| Tear: Other | 2.02 | 0.53-7.77 | .305 |
| Symptoms: Locking | 1.49 | 0.86-2.59 | .152 |
| Symptoms: Snapping | 0.84 | 0.47-1.50 | .56 |
| Symptoms: Clunking | 1.67 | 0.92-3.02 | .093 |
| Symptoms: Stiffness | 1.09 | 0.56-2.10 | .806 |
| Symptoms: Other | 0.77 | 0.34-1.75 | .528 |
| Tear Location: Posterior | 1.53 | 0.51-4.58 | .443 |
Bold values reflect significant results.
P < .05.
P < .01.
Final revision submitted November 1, 2025; accepted November 11, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.L. Niu has received support for education from Supreme Orthopedic Systems and Arthrex. J.C. Kirby has received compensation for education from Arthrex. T. Stavinoha has received support for education from Medinc. S. Carsen has received research support from Stryker and Smith & Nephew. Z. Stinson has received consulting fees from Arthrex. C. Finlayson has received support for education from Arthrex. R.J. Lee has research support from Vericel. D. Green has received consulting fees and royalties from Arthrex, royalties from Pega Medical, hospitality payments from OrthoPediatrics, and faculty/speaker fees from Synthes. J. Schlechter has received compensation for services other than consulting and support for education from Arthrex and support from Micromed. B. Heyworth has received consulting fees from and holds stock in Imagen Technologies and has received fees for education and education consulting from Arthrex and Kairos. G.A. Schmale has received research and education support from Arthrex and Summit Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Seattle Children's Research Institute (STUDY00001869).