
Abstract
Background:
Arthroscopic partial meniscectomy (APM) is performed for symptomatic meniscal tears that fail conservative treatment. Patients often report pain at night, although little research has been done to evaluate corresponding outcomes.
Purpose:
To (1) evaluate patients with and without preoperative nighttime pain who underwent APM and (2) assess postoperative resolution of symptoms and associated patient-reported outcome measures (PROMs).
Study Design:
Case series; Level of evidence, 4.
Methods:
Consecutive patients undergoing primary APM with or without chondroplasty at a tertiary academic center were prospectively enrolled in a database. Patient characteristics and PROMs were obtained pre- and postoperatively up to 2 years—including the visual analog pain scale, Knee injury and Osteoarthritis Outcome Score (KOOS), Marx Scale, and Veterans RAND 12-Item Health Survey (VR-12) physical and mental components. Patients were included if they had a minimum 3-month PROMs follow-up. Pain at night was defined as reporting greater than mild pain on KOOS P7. Intraoperatively, cartilage was assessed using the Outerbridge Classification.
Results:
A total of 587 patients were included, with 299 (50.9%) reporting preoperative pain at night, which corresponded with worse baseline PROMs. These patients were older and more likely to be women and smokers. No significant difference was observed in Outerbridge grade between patients with and without preoperative pain at night. Postoperatively, nighttime pain resolved by 2 years in 274 (91.6%) patients, 219 of whom (79.9%) reported improvement by 3 months. Patients whose pain at night persisted had a longer duration of symptoms preoperatively, higher body mass index, and a lack of baseline mechanical symptoms. PROMs significantly improved for patients with and without preoperative pain at night, although patients with baseline pain had worse scores compared with those without preoperative nighttime pain.
Conclusion:
Over half of patients undergoing APM reported preoperative pain at night, which was associated with worse baseline functional scores. Postoperatively, >90% of patients with baseline pain at night noted resolution of symptoms by 2 years, with nearly 80% showing improvement by 3 months. Functional scores improved after surgery for patients with and without initial pain at night, remaining lower for patients who had preoperative nighttime pain.
Atraumatic meniscal tears are common in the general population, typically presenting in middle-aged and older individuals. 15 Symptomatic patients may report impairment in quality of life and function, citing issues with pain and mechanical symptoms. 20 Furthermore, patients commonly report nighttime pain, increasing susceptibility to numerous adverse health effects associated with sleep disturbance—including respiratory infection, weight gain, and cardiovascular events.19,22
Debate remains regarding the optimal treatment of patients with symptomatic degenerative meniscal tears, with many studies comparing nonsurgical management via physical therapy versus arthroscopic partial meniscectomy (APM).1,10,13,26,29 The indications for APM in the setting of degenerative meniscal tears remain controversial; however, a subset of patients who fail conservative therapy and do not meet indications for total knee arthroplasty (TKA) likely still benefit. Several studies have investigated the impact of osteoarthritis and TKA on pain at night and sleep disturbance.4,5,8 However, little research has been conducted on nighttime pain in patients with symptomatic meniscal tears undergoing APM.
Therefore, this study aimed to investigate the incidence and factors related to preoperative pain at night in patients undergoing APM. Second, this study aimed to assess the postoperative resolution of nighttime pain and associated patient-reported outcome measures (PROMs).
Methods
After obtaining approval from the Mass General Brigham institutional review board (Protocol No. 2011P002663), a cohort of consecutive patients undergoing APM with or without chondroplasty at a single tertiary academic center by a single surgeon (E.M.) between March 2014 and April 2022 was prospectively enrolled in the Surgical Outcome System (SOS) (Arthrex)—a global registry database compliant with the Health Information Portability and Accountability Act (HIPAA). All patients provided informed consent. Patients were enrolled in the SOS by a research coordinator (N.L.), and preoperative questionnaires—including patient characteristics and PROMs—were collected at enrollment. Patients received PROMs surveys at 3-month, 6-month, 12-month, and 24-month timepoints postoperatively via email, and compliance was monitored by a research assistant (N.L.). Patients received follow-up emails and phone calls to improve follow-up compliance.
Patients included in the present study were consecutive patients at our institution who underwent primary APM with or without chondroplasty, had surgery at least 1 year before the data analysis (ie, eligible to complete PROMs up to 1 year after surgery), and had follow-up PROMs at ≥1 postoperative timepoints as described above. A preoperative response to KOOS question P7, “What amount of knee pain have you experienced in the last week at night while in bed?” was required. Pain at night was defined as reporting greater than mild pain on this question. A total of 693 patients underwent primary APM with or without chondroplasty during the study period and were enrolled in the SOS database. Of those, 638 patients provided a preoperative response to KOOS question P7. A total of 587 patients provided PROMs follow-up data at ≥1 postoperative timepoints and were included in the study cohort (Figure 1).
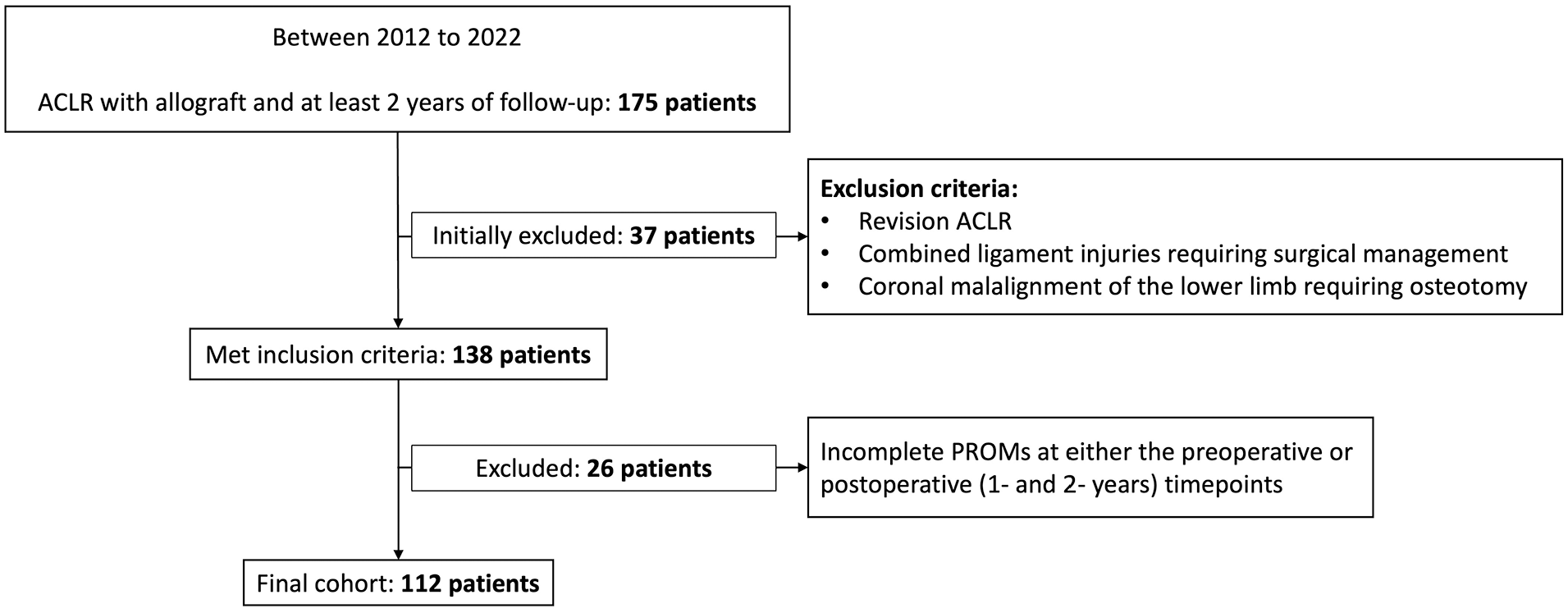
Study cohort selection criteria. ACLR, anterior cruciate ligament reconstruction; PROMs, patient-reported outcome measures.
APM was recommended for patients based on their clinical history, physical examination, and/or magnetic resonance imaging findings. Before surgical intervention, patients had failed a course of conservative treatment—including activity modification, anti-inflammatory drugs, physical therapy, and/or injections. All patients underwent outpatient APM under general anesthesia using a 2-portal arthroscopy technique. Patients were permitted to weight-bear as tolerated, were discharged with cryotherapy or ice packs, and instructed to use ibuprofen and acetaminophen for pain management as medically appropriate. A standard postoperative knee arthroscopy rehabilitation protocol was followed with physical therapy initiated at 2 weeks postoperatively.
Collected data included patient age, body mass index (BMI), sex, ethnicity, race, history of diabetes, smoking history, workers’ compensation status, presence or absence of mechanical symptoms, preoperative pain at night, and symptom duration. Validated clinical outcome instruments were administered both pre- and postoperatively—including the visual analog pain scale (VAS), 18 Knee injury and Osteoarthritis Outcome Score (KOOS), 23 Marx Scale, 17 and Veterans RAND 12-Item Health Survey (VR-12) physical and mental components. 25 According to standard PROMs survey collection intervals at our practice, KOOS and VAS Pain measures were collected at baseline, 3 months, 6 months, 12 months, and 24 months postoperatively, while the VR-12 was assessed at baseline, 6 months, 12 months, and 24 months postoperatively. The Marx Scale was assessed at baseline, 12 months, and 24 months postoperatively. The knee cartilage was assessed arthroscopically at the time of surgery and described using the Outerbridge Classification. 21
Measures of demographic and clinical characteristics were summarized using descriptive statistics. Comparisons were conducted using Fisher exact tests for categorical variables and independent-sample t tests or Wilcoxon rank sum tests for continuous variables. Linear mixed-effects models were used to assess changes in PROMs from preoperative baseline to postoperative follow-up intervals. Models were adjusted for age, smoking status, and sex. P < .05 was considered statistically significant. Statistical analyses were performed by a biostatistician at the study institution (J.C.) using SAS Version 9.4 (SAS Institute).
Results
Patient characteristics and clinical presentation are summarized in Table 1. The mean age at the time of surgery was 50.7 ± 9.5 years, with a median preoperative duration of symptoms of 4 months (interquartile range, 2-9 months). The mean BMI was 30.2 ± 6.1 kg/m2, with women accounting for 55.9% of patients. A total of 499 (85%) patients reported preoperative mechanical symptoms. Meniscal pathology involved only the medial meniscus in 403 (68.8%) patients, the lateral meniscus in 97 (16.6%) patients, and both in 86 (14.7%) patients.
Demographic Characteristics and Clinical Presentation a

BMI, body mass index; IQR, interquartile range; Preop, preoperative.
Preoperatively, 299 patients (50.9%) reported pain at night that was more than mild, as defined by KOOS question P7. Patients with preoperative pain at night were significantly older, more likely to be female, and more likely to be smokers compared with those without baseline pain at night, while there were no significant differences in meniscal tear laterality and Outerbridge grade assessment (Table 2). PROMs for patients with and without preoperative pain at night are presented in Table 3. When adjusted for age, sex, and smoking status, patients reporting preoperative pain at night had worse PROMs before surgery, except on the Marx Activity Scale.
Comparison of Patients With and Without Preoperative Pain at Night a

Bold P values indicate statistical significance. BMI, body mass index; IQR, interquartile range; Preop, preoperative.
Comparison of Preop PROMs in Patients With and Without Pain at Night, Adjusted for Sex, Age, and Smoking Status a
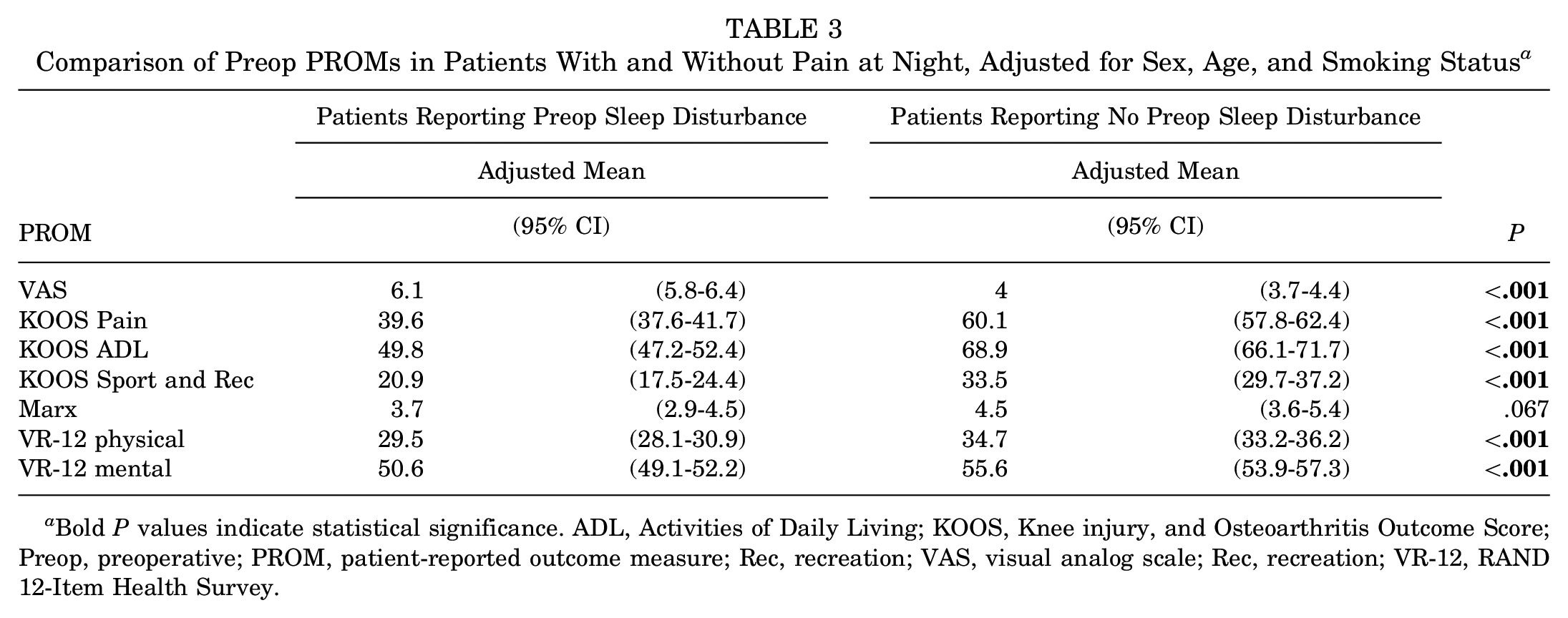
Bold P values indicate statistical significance. ADL, Activities of Daily Living; KOOS, Knee injury, and Osteoarthritis Outcome Score; Preop, preoperative; PROM, patient-reported outcome measure; Rec, recreation; VAS, visual analog scale; Rec, recreation; VR-12, RAND 12-Item Health Survey.
Postoperatively, of the 299 patients who reported preoperative pain at night, 274 (91.6%) reported resolution of symptoms by 2 years after surgery; 219 (79.9%) reported resolution by 3 months postoperatively, and 270 (98.5%) reported improvement by 1 year. Postoperative PROMs data were available for 80% of patients at 1 year postoperatively and for 70% of patients at 2 years post-operatively. When adjusted for sex, age, and smoking status, PROMs remained worse at the follow-up for patients who reported baseline nighttime pain compared with those without preoperative symptoms (Figure 2). A linear mixed effects model demonstrated that patients with preoperative pain at night achieved greater improvement in PROMs from baseline, although these values did not reach the level of patients without initial nighttime pain at the corresponding follow-up.
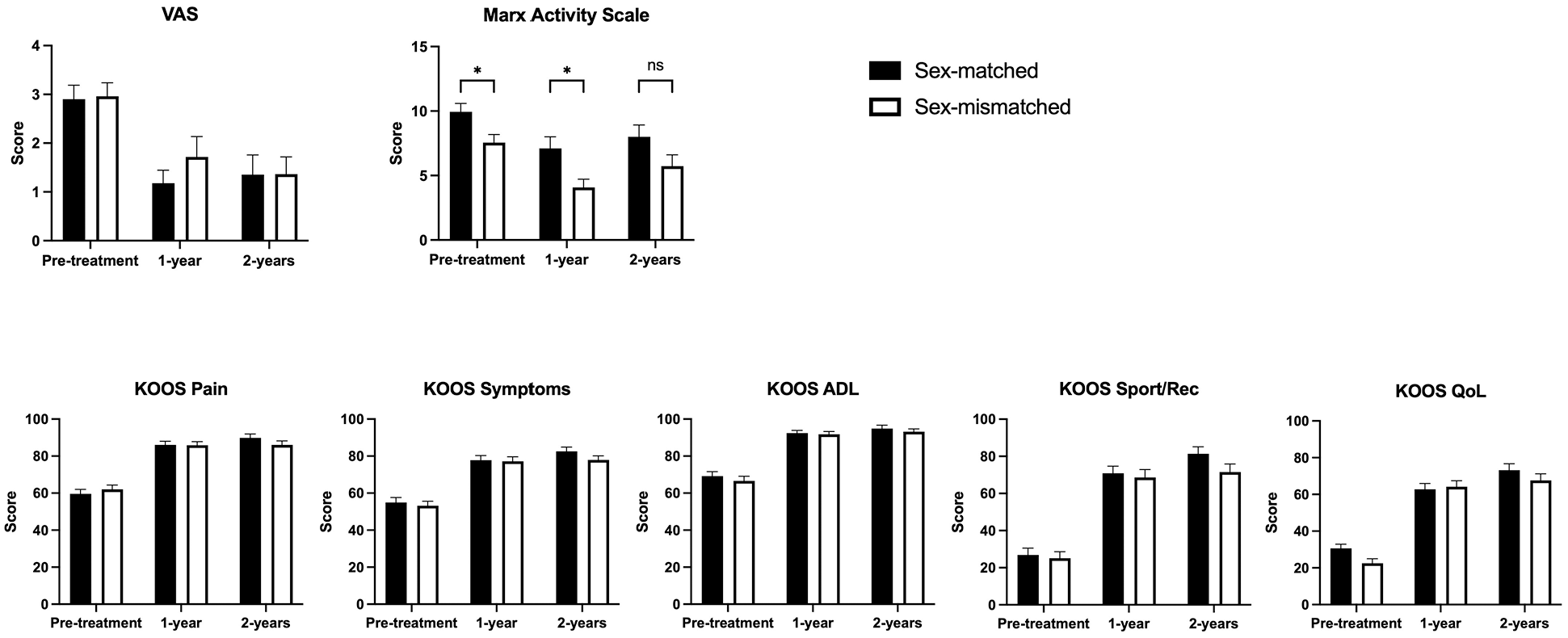
PROMs improved significantly for both patients with and without preoperative pain at night, although scores for those with baseline preoperative pain at night remained lower at the follow-up. ADL, activities of Daily Living; KOOS, Knee injury, and Osteoarthritis Outcome Score; Rec, recreation; PROMs, patient-reported outcome measures; Qol, quality of life; VAS, visual analog scale.
Among patients with preoperative pain at night, those who had persistent symptoms postoperatively reported a significantly longer duration of preoperative symptoms compared with patients whose symptoms resolved after surgery (10 months vs 4 months; P < .05) (Table 4). In addition, patients with persistent symptoms tended to have higher BMIs and were less likely to have had preoperative mechanical symptoms, although these differences did not reach statistical significance (P = .06; P = .06). A significant difference in the distribution of collected race characteristics between the 2 groups was noted (P = .031). No significant difference was identified in intraoperative Outerbridge grade between patients whose pain at night resolved and those whose pain did not.
Comparison of Patients With Resolved and Unresolved Pain at Night a
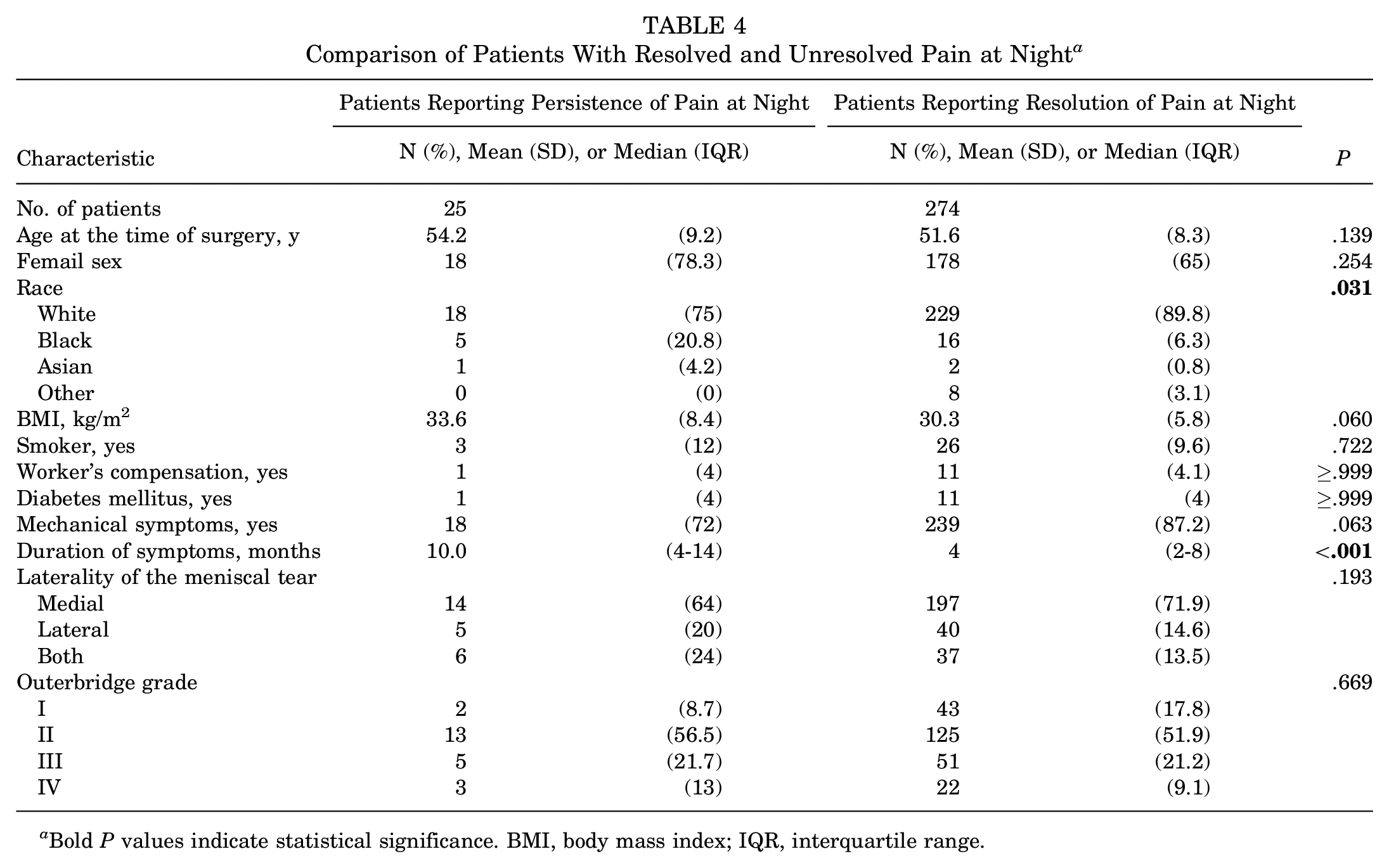
Bold P values indicate statistical significance. BMI, body mass index; IQR, interquartile range.
Discussion
Osteoarthritis is estimated to affect >37.5% of adults in the United States and often leads to significant functional impairment. 15 The association between osteoarthritis of the knee and nighttime discomfort, in particular, is well established.24,27 Many patients have symptomatic degenerative disease of the knee but lack sufficient arthritis for consideration of TKA. For these patients, APM is commonly performed to treat symptomatic meniscal tears that fail conservative management. However, little research has assessed nighttime pain in this population and the impact of APM. Over half of the patients who underwent APM in our study reported significant preoperative pain at night, indicating a significant level of impairment. As nighttime pain was associated with worse baseline functional scores, clinicians should inquire about these symptoms when evaluating patients with symptomatic meniscal pathology. Our study suggests that patients with pain at night are older and more likely to be smokers compared with those without preoperative nighttime pain.
Indications for APM in the setting of degenerative disease of the knee remain the subject of significant debate. Several historical studies with mid- to longer-term follow-ups demonstrate favorable outcomes after APM.2,3 However, reports in the medical literature suggest that there may be no difference in outcomes between APM and conservative management or sham surgery.10,13,26,29 While well-publicized, many of these studies demonstrate methodologic concerns—including small sample sizes, nonrepresentative patient inclusion criteria, and treatment crossover. 7 Recent reports by Gauffin et al 9 suggest improved short- to medium-term outcomes after APM in conjunction with physical therapy when compared with physical therapy alone, although the long-term sustainability of these benefits remains unclear. Based on the existing body of evidence, a subset of patients are likely to still benefit from APM, with current research ongoing to identify these patients. APM remains commonly performed for symptomatic meniscal tears that persist despite conservative management alone.1,7,11,14
The present study indicates that patients with preoperative nighttime pain before APM can usually expect rapid resolution of these symptoms, with most reporting improvement by 3 months. In our cohort, PROMs also improved postoperatively for both patients with and without preoperative pain at night, although postoperative PROMs remained poorer for patients who had pain at night before surgery. This suggests that patients may see improvement in symptoms and function regardless of the presence or absence of preoperative pain at night, although, after surgery, those with preoperative nighttime pain do not catch up to those who did not have preexisting pain at night. As the indications for APM remain the topic of significant debate, the impact of surgery versus conservative therapy alone on nighttime pain warrants further investigation.
Numerous factors have been hypothesized to influence outcomes after APM—including the presence of mechanical symptoms, meniscal tear pattern, degree of osteoarthrosis, and patient age.12,16,28 A recent review by Eijgenraam et al 6 suggested that longer duration of symptoms, radiographic osteoarthritis, and greater meniscal resection were associated with worse clinical outcomes after APM. Similarly, our study found that patients who reported persistent nighttime pain postoperatively had a longer duration of preoperative symptoms. Although our study found no influence of intraoperative Outerbridge grade assessment, longer symptom duration may reflect more severe degenerative pathology, with further study needed to identify other confounding variables. Patients with persistent symptoms after surgery also tended to have higher BMIs and were less likely to have had preoperative mechanical symptoms, although these differences did not reach statistical significance. Notably, 85% of patients in our study endorsed mechanical symptoms preoperatively, with improved outcomes after surgery possibly related to intervention on the source of these mechanical symptoms. Our study also identified a significant difference in the distribution of reported race between patients who reported resolution of pain at night and those who persisted. As our study participants were predominantly White and from a single institution with relatively few patients noting persistent nighttime pain, additional investigation is necessary to assess demographic and socioeconomic factors that may impact patient outcomes after APM.
Limitations
The present study has several limitations. First, the lack of a nonoperative control group prevents definitive conclusions about the extent that APM results in improvement of nighttime pain. Second, just as with any study design tracking longitudinal patient outcomes, longer-term follow-ups, and PROM assessments may suffer from attritional bias due to differences between patients who respond to surveys compared with those who do not. Our study achieved a 70% PROMs follow-up at 2 years for eligible patients, although future studies with complete longer-term patient follow-ups will reduce bias and provide a more comprehensive understanding of patient outcomes. Next, while our study included intraoperative assessment of focal cartilage defects via Outerbridge grading, insufficient collection of radiographic Kellgren and Lawrence grading limited our analysis of radiographic degenerative disease. Additional assessment of other factors—including meniscal tear morphology and degree of surgical excision—will also help better identify patients who maximally benefit from APM. Finally, APM may not be a definitive treatment for many patients, with longer-term follow-ups needed to assess for reemergence of symptoms, subsequent radiographic changes, and progression to TKA. Future prospective multicenter investigations with larger sample sizes will improve the generalizability of findings and guide both patient selection and operative technique to advance patient outcomes.
Conclusion
Approximately half of patients undergoing APM reported significant preoperative pain at night, which was associated with worse baseline functional scores. Postoperatively, >90% of patients with initial nighttime pain reported a resolution of symptoms by 2 years, and nearly 80% of the symptoms improved by 3 months. Functional scores improved significantly postoperatively for both patients with and without preoperative pain at night, although they remained lower in patients who had night-time pain before surgery.
Footnotes
Final revision submitted August 28, 2024; accepted October 4, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.G.M. has received nonconsulting fees from Arthrex; education payments from Arthrex, Kairos Surgical, and Peerless Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Mass General Brigham (reference No. 2011P002663).