
Abstract
Background:
Active-duty military service members experience posterior glenohumeral instability at a rate that far outpaces that of nonmilitary populations. While the outcomes after primary posterior labral repair (PLR) in this population are promising, the outcomes after revision procedures remain poorly described.
Purpose:
To report midterm outcomes after revision PLR in a population of active-duty military patients.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients who underwent revision PLR from January 2011 through December 2018 by the senior surgeon with a minimum of 5 years of follow-up were deemed eligible for inclusion. Preoperative and postoperative outcome scores for the visual analog scale (VAS) for pain, the American Shoulder and Elbow Surgeons (ASES) score, the Single Assessment Numeric Evaluation (SANE), and the Rowe instability score as well as the rates of return to active duty and sports and the rate of recurrent instability were collected and pooled for analysis.
Results:
Overall, 21 patients with a mean follow-up of 77.95 ± 39.54 months met inclusion criteria and were available for analysis. At midterm follow-up, patients who underwent revision PLR experienced significantly improved VAS (from 7.3 ± 1.8 to 2.9 ± 2.4), ASES (from 49.5 ± 12.6 to 79.7 ± 16.7), SANE (from 45.0 ± 14.8 to 80.2 ± 20.3), and Rowe (from 37.6 ± 9.4 to 79.4 ± 24.7) scores. Over 80% of patients also achieved the minimal clinically important difference for these outcome measures; however, only 52% to 62% of patients achieved the Patient Acceptable Symptom State. The return-to-sport rate was 66.67%, and the return to active-duty rate was 80.95%.
Conclusion:
While patients who underwent revision PLR experienced improvements in outcomes and a decrease in pain on average, they exhibited rates of return to active-duty and sports that lagged behind those demonstrated in a previous cohort that underwent a primary procedure. Furthermore, the achievement of clinically significant outcomes after revision PLR was less consistent compared with that after primary PLR.
Keywords
Posterior glenohumeral instability has become increasingly recognized as a source of shoulder pain in certain patient populations.1,13,20,23,28,31,34 Although this subset of shoulder instability occurs less frequently than classic anterior instability, recent evidence suggests that the incidence of this abnormality is far higher than previously thought, especially in athletic and military populations.1,13,20,23,31,34 In patients whose symptoms are refractory to nonoperative management, surgical treatment is typically arthroscopic posterior labral repair (PLR), a procedure that has demonstrated reliability in returning patients to both athletic pursuits and military duty.6-8,12,14,17,25,26,28
Promisingly, failure rates after primary PLR are low, and the procedure is associated with high rates of return to both sports and military duty. 8 Patients who do experience treatment failure, however, often continue to experience shoulder pain and symptoms that remain unresponsive to nonoperative management.2,3,16 Unfortunately, the optimal management of these patients remains unknown. A recent systematic review that screened the full text of 28 studies was only able to identify 26 patients across 3 studies who underwent revision arthroscopic PLR.3,5,16,27 Subsequently, much remains to be investigated regarding outcomes after revision PLR, especially among active-duty patients whose physical training requirements such as pushups contribute to their ability to complete their occupational requirements and be promoted in rank.
Because of limited research into revision PLR, the purpose of this study was to investigate the outcomes of revision PLR in a population of military patients at midterm follow-up to contribute to a greater body of literature discussing expected postoperative outcomes. The secondary purpose of this study was to compare these findings with outcomes after primary PLR among active-duty patients as described in existing literature. 28 We hypothesized that revision PLR would result in clinical and subjective improvements that would be sustained at midterm follow-up.
Methods
Study Design
This is a retrospective review of prospectively collected data investigating patient-reported outcomes, range of motion, complications, and recurrence in active-duty service members who underwent revision PLR between January 2011 and December 2018. Institutional review board approval was obtained before beginning the study.
Patient Population
Inclusion criteria included active-duty United States Army patients older than 18 years who underwent revision PLR for unidirectional posterior glenohumeral instability with a minimum 5-year follow-up. Excluded from this study were patients with multidirectional instability (defined as patients without a discrete labral tear on imaging who demonstrated a sulcus sign and hyperlaxity on clinical examination), patients who were habitual or voluntary shoulder subluxators, patients with concomitant cartilage injuries at the time of revision, patients undergoing concomitant rotator cuff repair or superior labrum anterior to posterior (SLAP) repair, patients with previous surgery on the involved shoulder (except for PLR), and patients with posterior glenoid bone loss >13.5%. Bone loss was quantified on magnetic resonance imaging based on modifications of the technique first described by Di Giacomo et al. 9
Patients deemed to have recurrent instability and to have failed index PLR all (1) reported pain as their chief complaint, (2) demonstrated posterior apprehension on provocative posterior instability tests, and (3) described pain frequent enough to interfere with both military-duty requirements and their activities of daily living. Patients with posterior dislocations, subluxations, or pain with posterior instability were all included in this study.
Patient age, sex, laterality, and military occupation were obtained. Outcome scores collected included those for the Rowe instability score, the American Shoulder and Elbow Surgeons (ASES) score, and the Single Assessment Numeric Evaluation (SANE).18,19,30 Additional outcomes collected included the visual analog scale (VAS) for pain score, range of motion in forward flexion as well as external rotation and internal rotation, complications, and rate of return to active-duty service. Patients with subjective military-duty limitations or those who required separation from military duty because of their shoulder abnormality were classified as failure to return to active duty. Outcomes were collected by the operating surgeon and clinical team. The reporting of our findings adheres to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) recommendations. 33
Surgical Technique
All surgical procedures were performed by the senior author (N.P.). Patients were positioned in a modified beach-chair position after the administration of general anesthesia and a presurgical interscalene block. An examination was performed under anesthesia to evaluate shoulder range of motion and stability in the anterior and posterior directions. A Spider hydraulic arm holder (Smith & Nephew) was then employed to stabilize the operative shoulder, and the patient was draped in a standard fashion. A complete diagnostic arthroscopic examination of the glenohumeral joint was performed. An evaluation of the posterior labrum was performed with the arthroscope in the anterior portal. Once the tear was confirmed, all suture material from the previous repair site was removed, and the quality of remnant capsulolabral tissue was evaluated. The labrum and glenoid were mobilized and prepared similarly to primary procedures, 28 and 0.5 to 1.0 cm of capsular tissue was included with each pass of the suture passer. All procedures were completed with 3 or 4 double-loaded anchors. Of note, our revision technique does not vary significantly from primary surgical fixation other than the removal of suture material from the primary repair site.
Postoperative Rehabilitation
All procedures were performed on an outpatient basis. Patients were instructed to begin shoulder pendulum exercises as well as elbow, wrist, and finger active range of motion exercises once their interscalene nerve block had worn off. Patients were immobilized in neutral rotation in a SmartSling (Ossur) for 6 weeks. Passive forward elevation was permitted beginning at 4 weeks postoperatively. Active range of motion and progressive strengthening were initiated at 6 weeks postoperatively. All patients attended formal physical therapy sessions at the same military physical therapy group and were prescribed the same protocol. Return to unrestricted activity was allowed as early as 6 months postoperatively, depending on clearance from the treating physical therapist and the patient reporting a subjective readiness to return to active duty, which included the ability to perform the minimum number of pushups to pass the army physical fitness test. All patients were placed on a limited-duty profile for 90 days after surgery to allow for maximum participation in physical therapy while avoiding possible injuries during group physical readiness training.
Statistical Analysis
All statistical analyses were performed with RStudio (Version 2023; Posit). Previously published values based on a military population with posterior shoulder instability for the minimal clinically important difference (MCID), Patient Acceptable Symptom State (PASS), and substantial clinical benefit (SCB) were used. 29 Continuous data were reported as mean ± standard deviation, whereas the frequency and percentage were reported for categorical variables. Paired-samples t tests were used to compare preoperative and postoperative outcome scores. The chi-square test and Fisher exact test were utilized to compare categorical variables. Statistical significance was set at alpha <.05.
Results
During the study period, the senior surgeon performed 128 PLR procedures. Of these, 17 patients underwent concomitant arthroscopic rotator cuff repair, 13 patients underwent concomitant SLAP repair, and 4 patients were unable to be contacted for follow-up. Of the remaining patients, 73 underwent a primary procedure, leaving 21 patients who underwent a revision procedure eligible for study inclusion (Figure 1). Notably, 3 of the patients eligible for inclusion underwent primary repair with the senior author and met the criteria for revision PLR. Patient- and surgery-specific data are available in Table 1.
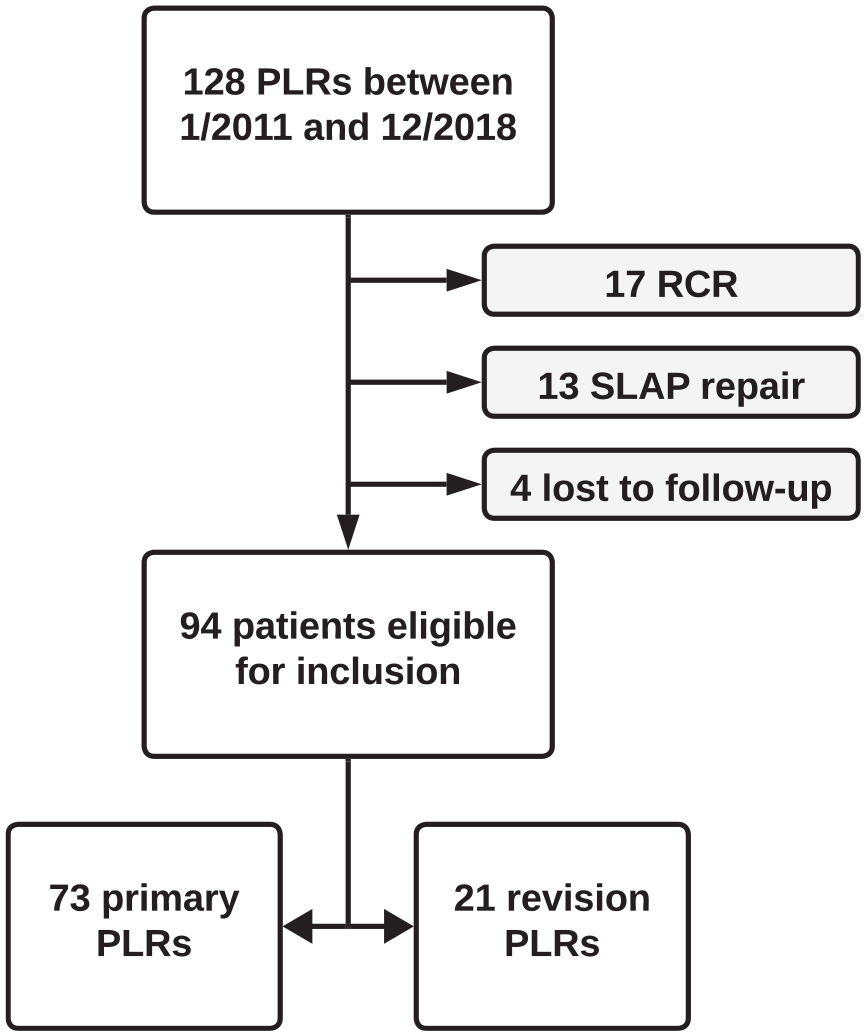
Flowchart of patient selection.
Patient and Surgical Characteristics a

Data are reported as mean ± SD or n (%).
This category is defined as patients whose military duties require regular high-demand physical readiness training, firearms manipulation, movement across uneven or rugged terrain and/or obstacles with heavy loads, hand-to-hand combat training, and other war-fighting tasks.
In our cohort of revision PLR, 15 (71.43%) patients had evidence of the utilization of only 1 or 2 anchors during their initial procedure. There were 18 (85.71%) patients who underwent their initial procedure by a surgeon without sports medicine or shoulder/elbow fellowship training. While none of the patients had >13.5% glenoid bone loss, 14 (66.67%) patients had some degree of bone loss (mean, 6.4%), and the dominant arm was involved in 15 (71.43%) revision cases.
At midterm follow-up, most patients who underwent revision PLR were able to return to both active duty and sporting activities (80.95% and 66.67%, respectively). There were 2 (9.52%) cases of recurrent instability. Patient-reported outcomes all significantly improved postoperatively including the VAS pain (from 7.3 ± 1.8 to 2.9 ± 2.4), ASES (from 49.5 ± 12.6 to 79.7 ± 16.7), SANE (from 45.0 ± 14.8 to 80.2 ± 20.3), and Rowe (from 37.6 ± 9.4 to 79.4 ± 24.7) scores, as shown in Table 2. There were no statistically significant changes in range of motion postoperatively including forward flexion, external rotation, and internal rotation.
Preoperative and Postoperative Outcomes a

Data are reported as mean ± SD. Bold P values indicate statistical significance. ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
The improvement in patient-reported outcome scores met the MCID in 85.71% of patients for the VAS pain, 80.95% of patients for the ASES score, 85.71% of patients for the SANE, and 85.71% of patients for the Rowe score. There were fewer patients who achieved the SCB (19.05% for VAS pain, 38.10% for ASES score, 61.90% for SANE, and 23.81% for Rowe score). Over half of the patients achieved the PASS postoperatively (61.90% for VAS pain, 61.90% for ASES score, 52.38% for SANE, and 57.14% for Rowe score). These rates are detailed in Table 3.
Patient-Reported Outcome Measure Thresholds a

ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; PASS, Patient Acceptable Symptom State; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit; VAS, visual analog scale.
Discussion
Classically, posterior glenohumeral instability with a concomitant posterior labral injury was considered a rarely encountered abnormality.5,8,23,27 More recent evidence, however, suggests that posterior glenohumeral instability is far more commonly encountered than previously thought, especially among active and military patient populations.1,13,20,31,34 Fortunately, outcomes after primary PLR are promising, with multiple studies asserting that, with clear indications and a sound surgical technique, patients can expect high rates of return to sports and activities of daily living with a marked decrease in pain.6,12,14,17,21,25,26,28 Despite the high rates of success seen with primary repair, treatment failure can occur, with patients often experiencing the return of pain and difficulty in conducting not only athletic pursuits but also occupational and daily activities. 16 Given our increasing understanding of the true incidence of the underlying abnormality, and the likely increase in patients undergoing treatment, it is imperative that we further characterize not only the risk factors for failure but also the outcomes after a revision surgical intervention.
Even as our understanding of the nature of glenohumeral instability, and specifically posterior instability, continues to grow, outcomes after revision PLR remain poorly described, with only a few studies in the literature. A recent systematic review that screened 990 studies identified only 3 studies (26 cases) in which outcomes after revision PLR were reported. 16 The earliest outcomes after revision PLR were described by Provencher et al. 27 In that study, 4 patients, all of whom had been previously treated with posterior thermal capsulorrhaphy, underwent either PLR (n = 3 [75%]) or capsular plication (n = 1 [25%]). Outcomes after that procedure, overall, were poor, with half of the patients reporting persistent pain and 3 of 4 patients reporting symptoms consistent with treatment failure. Given the fact that all 4 patients had undergone previous thermal capsulorrhaphy, these results are not surprising. 11 Chalmers et al 5 also published a small case series of 3 patients who underwent revision PLR. Promisingly, none of their patients reported persistent pain or recurrent instability, and all 3 patients were able to achieve full range of motion and the restoration of strength. The largest series on outcomes after revision PLR was conducted by Bradley et al, 3 who reported on the outcomes of 19 patients. Based on their study criteria, 21% of patients experienced treatment failure, and only 15% of patients thought that the revision surgical intervention was worthwhile. Their group has also published on the outcomes of revision posterior stabilization in contact and throwing athletes, with patients undergoing revision procedures demonstrating less favorable return-to-sports rates and outcome scores.2,32 Of concern, despite a litany of evidence asserting that active-duty military members experience posterior glenohumeral instability at a much higher rate compared with nonmilitary patients, there is only a single small case series of 4 patients reporting on the outcomes of revision posterior stabilization in this patient population.1,13,20,23,27,28,31,34 It is important to note that those 4 patients had previously undergone posterior thermal capsulorrhaphy, a procedure that has all but fallen out of clinical practice and application.
The current study represents, to the best of our knowledge, the first report of outcomes after revision PLR in a population of active-duty patients. Promisingly, our results showed statistically and clinically improved outcomes after revision PLR at midterm follow-up. Patients who underwent revision PLR, on average, experienced improvements in function and a decrease in pain, with over 80% of patients achieving the MCID. Most patients were also able to return to sports (66.67%) and return to activity duty (80.95%).
A secondary aim of our study was to compare the current study’s results of revision PLR to those of a similar military patient population that underwent primary PLR in a previously published study. Results from existing data published by Scanaliato et al 28 regarding outcomes after primary PLR among active-duty service members with posterior instability without significant glenoid bone loss were compared with results from the present study detailing outcomes after revision PLR.
Patients who underwent revision procedures were able to return to both active duty (80.95% vs 95.89%, respectively; P = .022) and sporting activities (66.67% vs 90.41%, respectively; P = .007) less frequently than those who underwent primary procedures. Furthermore, patients who underwent revision procedures, on average, experienced less pronounced improvements in outcomes, as measured by the ASES score (30.14 vs 39.03, respectively; P = .042), and less improvement in pain, as measured by the VAS pain (4.48 vs 5.98, respectively; P = .027) (Appendix Table A1). Otherwise, there was no difference between the cohorts with respect to preoperative or postoperative function and range of motion, rate of recurrent symptoms, or improvement in function and range of motion.
With respect to the achievement of clinically significant outcomes, patients who underwent primary procedures were more likely to exceed the MCID for the VAS pain (97.26% vs 85.71%, respectively; P = .0378) and ASES score (95.89% vs 80.95%, respectively; P = .0216), meet the PASS for the VAS pain (82.19% vs 61.90%, respectively; P = .0492), and achieve the SCB for the ASES score (65.75% vs 38.10%, respectively; P = .0229) than patients who underwent revision procedures (Appendix Table A2). Otherwise, there was no statistically significant difference in the achievement of clinically significant outcomes between the 2 cohorts.
When revision surgery was compared with primary surgery in a similar population of patients, the revision cohort experienced improvements in outcomes and a decrease in pain but exhibited rates of return to active duty and sports that lagged behind those of the primary cohort. Furthermore, the achievement of clinically significant outcomes after revision PLR was less consistent compared with that after primary PLR. Altogether, these findings suggest that while revision PLR can provide improvements in outcomes and a reduction in pain, the results are not as predictable and profound as primary PLR and that patients should be counseled accordingly on the expected outcomes before pursuing a revision surgical intervention.
Overall, these findings do not deviate markedly from the published literature, limited as it is.2,5,27 While revision PLR, on average, produced improvements in patient function and decreases in pain, when compared with the outcomes after primary procedures, patients were less likely to achieve clinically significant outcomes and more likely to experience an inability to return to both sporting activities and, in the case of our cohort, active-duty military service. Furthermore, these outcomes grossly align with those seen in patients undergoing revision anterior stabilization, and other intra-articular procedures in the shoulder, in that while outcomes can be favorable for some patients, they are less predictable and often lag behind those observed in patients undergoing primary procedures.4,10,15,22,24 While the exact reason behind the disparity in outcomes in the current study remains speculative at best, it is our experience that patients undergoing revision PLR often possess capsulolabral tissue that demonstrates attritional wear and degeneration. It, therefore, follows that even when well-performed PLR is completed, the posterior capsule and ligamentous restraints may be unable to fully aid in preventing posterior subluxations, leading to continued symptoms for patients.
Given that patients undergoing revision PLR exhibit outcomes that lag behind those after primary procedures, continued study into the risk factors for failure after repair is of paramount importance. In a recent study, Bradley et al 3 identified dominant shoulder surgery, female sex, a concomitant rotator cuff injury, the use of ≤3 anchors, and smaller glenoid bone width as risk factors for failure after primary posterior capsulolabral repair. When limited to a population of contact athletes, a smaller glenoid bone width and higher degrees of preoperative instability were independent risk factors for failure. 2 Among throwing athletes, female sex has been identified as a risk factor for failure. 32 Because most of the revision cases were referred to our team, we are unable to perform any statistical analysis regarding risk factors for failure. Given the likely multifactorial nature of failure after PLR, we believe that large prospective multicenter studies would be best for elucidating the risk factors for failure after PLR in a military population.
Limitations
This study is not without limitations. The cohort is predominantly male and composed entirely of active-duty soldiers, which may limit the generalizability to non-military patients. All procedures were performed by a single shoulder/elbow fellowship-trained surgeon with extensive experience in managing active-duty military patients. With that said, not all of the primary procedures in the revision cohort were performed within our system; therefore, detailed surgery-specific data for these patients were not available. Finally, the results are from a retrospective analysis of prospectively collected data, which introduces the risk of selection bias inherent to this type of study design.
Conclusion
While patients who underwent revision PLR, on average, experienced improvements in outcomes and a decrease in pain, they exhibited rates of return to active duty and sports that lagged behind those demonstrated in patients who underwent a primary procedure. Furthermore, the achievement of clinically significant outcomes after revision PLR was less consistent compared with that after primary procedures in existing literature. Overall, these results suggest that while revision PLR, on average, can produce meaningful improvements in outcomes and decreases in pain, there are patients who are at risk for poor outcomes after this procedure.
Footnotes
Appendix
Comparison of Achievement of Clinical Outcome Thresholds Between Primary and Revision PLR a

| Primary (n = 73) | Revision (n = 21) | Difference b | P | |
|---|---|---|---|---|
| VAS pain | ||||
| Exceeded MCID | 71 (97.26) | 18 (85.71) | 11.55 |
|
| Met PASS | 60 (82.19) | 13 (61.90) | 20.29 |
|
| Achieved SCB | 30 (41.10) | 4 (19.05) | 22.35 | .0639 |
| SANE | ||||
| Exceeded MCID | 67 (91.78) | 18 (85.71) | 6.07 | .4051 |
| Met PASS | 53 (72.60) | 11 (52.38) | 20.22 | .0798 |
| Achieved SCB | 45 (61.64) | 13 (61.90) | −0.26 | .9832 |
| ASES | ||||
| Exceeded MCID | 70 (95.89) | 17 (80.95) | 14.94 |
|
| Met PASS | 55 (75.34) | 13 (61.90) | 13.44 | .2251 |
| Achieved SCB | 48 (65.75) | 8 (38.10) | 27.65 |
|
| Rowe | ||||
| Exceeded MCID | 72 (98.63) | 18 (85.71) | 12.92 | .0927 |
| Met PASS | 48 (65.75) | 12 (57.14) | 8.61 | .4693 |
| Achieved SCB | 23 (31.51) | 5 (23.81) | 7.70 | .4967 |
Data are reported as n (%). Bold P values indicate statistical significance. ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; PASS, Patient Acceptable Symptom State; PLR, posterior labral repair; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit; VAS, visual analog scale.
Positive value denotes a higher value for the primary procedure, with results from Scanaliato et al. 28
Final revision submitted October 6, 2024; accepted October 10, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.P.S. has received hospitality payments from Stryker and Encore Medical. N.P. has received consulting fees from Medical Device Business Services and DePuy Synthes and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Carthage Institutional Review Board (2023-8).