
Abstract
Background:
Posterior glenohumeral instability is an increasingly recognized cause of shoulder pain and dysfunction among young, active populations. Outcomes after posterior stabilization procedures are commonly assessed using patient-reported outcome measures including the Single Assessment Numeric Evaluation (SANE), the Rowe instability score, the American Shoulder and Elbow Surgeons (ASES) score, and the visual analog scale (VAS) for pain. The clinical significance thresholds for these measures after arthroscopic posterior labral repair (aPLR), however, remain undefined.
Purpose:
We aimed to define the minimal clinically important difference (MCID), substantial clinical benefit (SCB), and patient acceptable symptomatic state (PASS) for the SANE, Rowe score, and ASES score as well as the VAS pain after aPLR. Additionally, we sought to determine preoperative factors predictive of reaching, as well as failing to reach, clinical significance.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
This study was a retrospective analysis of patient-reported outcome scores collected from patients who underwent aPLR between January 2011 and December 2018. To determine the clinically significant threshold that corresponded to achieving a meaningful outcome, the MCID, SCB, and PASS were calculated for the SANE, Rowe score, ASES score, and VAS pain utilizing either an anchor- or distribution-based method. Additionally, univariate and multivariate logistic regression analyses were performed to determine the factors associated with achieving, or not achieving, the MCID, SCB, and PASS.
Results:
A total of 73 patients with a mean follow-up of 82.55 ± 24.20 months were available for final analysis. MCID, SCB, and PASS values for the VAS pain were 1.10, 6, and 3, respectively; for the ASES score were 7.8, 34, and 80, respectively; for the SANE were 10.15, 33, and 85, respectively; and for the Rowe score were 11.3, 60, and 90, respectively. To meet the MCID, male sex (odds ratio [OR], 1.1639; P = .0293) was found to be a positive predictor for the VAS pain, and a lower preoperative SANE score (OR, 0.9939; P = .0003) was found to be a negative predictor for the SANE. Dominant arm involvement was associated with lower odds of achieving the PASS for the ASES score (OR, 0.7834; P = .0259) and VAS pain (OR, 0.7887; P = .0436). Patients who reported a history of shoulder trauma were more likely to reach the PASS for the SANE (OR, 1.3501; P = .0089), Rowe score (OR, 1.3938; P = .0052), and VAS pain (OR, 1.3507; P = .0104) as well as the SCB for the ASES score (OR, 1.2642; P = .0469) and SANE (OR, 1.2554; P = .0444). A higher preoperative VAS pain score was associated with higher odds of achieving the SCB for both the VAS pain (OR, 1.1653; P = .0110) and Rowe score (OR, 1.1282; P = .0175). Lastly, concomitant biceps tenodesis was associated with greater odds of achieving the SCB for the ASES score (OR, 1.3490; P = .0130) and reaching the PASS for the SANE (OR, 1.3825; P = .0038) and Rowe score (OR, 1.4040; P = .0035).
Conclusion:
To our knowledge, this study is the first to define the MCID, SCB, and PASS for the ASES score, Rowe score, SANE, and VAS pain in patients undergoing aPLR. Furthermore, we found that patients who reported a history of shoulder trauma and those who underwent concomitant biceps tenodesis demonstrated a greater likelihood of achieving clinical significance. Dominant arm involvement was associated with lower odds of achieving clinical significance.
Posterior glenohumeral instability is an increasingly recognized cause of shoulder pain and dysfunction.6,21,29,35,37,41 Military populations are known to be at an increased risk for posterior instability because of the high-demand shoulder activities required as a part of routine military training and therefore represent a unique opportunity to study this abnormality.17,32,35,37,41 Although operative management is often indicated for the treatment of posterior instability,2,29,32 outcomes after posterior stabilization remain incompletely understood compared with after anterior labral repair.
Outcome reporting after shoulder stabilization procedures is heavily reliant on patient-reported outcome measures (PROMs) such as the Single Assessment Numeric Evaluation (SANE), the Rowe instability score, the American Shoulder and Elbow Surgeons (ASES) score, and the visual analog scale (VAS) for pain.12,14,17,20,24,32-34 Given the frequency with which these measures are used to evaluate surgical outcomes, it is imperative that the clinical relevance for these measures be understood. Commonly used clinical significance thresholds include the minimal clinically important difference (MCID), substantial clinical benefit (SCB), and patient acceptable symptomatic state (PASS). Specifically, the MCID defines the change in the outcome score that results in the smallest, appreciable clinical improvement after surgery, 18 the SCB indicates a further improvement that a patient finds to be considerable, 9 and the PASS establishes the postoperative outcome score required to reflect patient satisfaction.30,39 While these values have been reported for a variety of shoulder procedures,9,19,25,26,30,36,38 they remain undefined for arthroscopic posterior labral repair (aPLR).
The purpose of this study was to define the MCID, SCB, and PASS for the VAS pain, SANE, Rowe score, and ASES score after aPLR. Additionally, we sought to determine preoperative factors predictive of reaching, as well as failing to reach, clinical significance. With respect to predictors, our hypothesis was that patients with a history of shoulder trauma and who undergo concomitant biceps tenodesis would experience a higher likelihood of achieving clinically significant outcomes.
Methods
Study Design
This study was a retrospective analysis of shoulder PROMs. All patients who underwent aPLR between January 2011 and December 2018 were screened for possible inclusion. The outcomes for these patients have been previously reported in a separate study investigating the effect of anchor composition on posterior labral repair outcomes. 32 Excluded from this study were patients with posterior glenoid bone loss >20% or glenoid retroversion >15°, patients who were voluntary shoulder subluxators, patients with anterior instability, patients who underwent concomitant arthroscopic rotator cuff repair or superior labrum anterior-posterior (SLAP) repair, or patients who underwent a revision posterior stabilization procedure. Clinically, all patients had pain as their primary chief complaint and noted pain and posterior apprehension symptoms severe enough to regularly interfere with their military occupation requirements and activities of daily living. All patients had undergone at least 3 months of nonoperative treatment, including anti-inflammatory medications, physical therapy, and home exercises before being considered for surgery. On physical examination, all patients were found to have positive posterior apprehension test and Kim test findings. Intraoperatively, biceps tenodesis was performed for patients with evidence of biceps tendon abnormalities, such as the lipstick sign or fraying of the biceps tendon as it entered the proximal aspect of the bicipital groove, on diagnostic arthroscopic examination. Institutional review board approval was obtained before beginning the study.
Outcome Measures
All patients completed shoulder-specific PROMs including the SANE, the Rowe instability score, and the ASES score preoperatively and at final follow-up. In addition, patients graded their pain level from 0 to 10 utilizing the VAS for pain. Preoperative and postoperative factors collected and analyzed to identify predictors of achieving clinical significance included military occupation, delay until surgery, time since surgery, number of anchors used, history of tobacco use, patient age at the time of surgery, dominant arm involvement, history of shoulder trauma, concomitant biceps tenodesis, endorsement of recurrent instability, and maintenance of active-duty military status.
Functional Outcome Evaluation
To determine the clinically significant threshold that corresponded to achieving a meaningful outcome, the MCID, SCB, and PASS were calculated for the SANE, Rowe score, ASES score, and VAS pain utilizing either an anchor- or distribution-based method.7,8 Because many patients undergoing posterior labral repair will have improvements in outcomes, the MCID for the SANE, Rowe score, ASES score, and VAS pain was calculated utilizing a distribution-based method, using one-half of the standard deviation for the overall change in each outcome score across the entire cohort. 15 Patients were classified as surpassing the MCID if their improvement in the outcome score was greater than the calculated MCID value.
The PASS was calculated using an anchor-based method. At final follow-up, patients were asked the following anchor question: “Taking into account all activities you have done during your daily life, your level of pain, and also your functional impairment, do you consider that your current state is satisfactory?” 9 PASS values were then determined through receiver operating characteristic (ROC) curve analysis. 16 The PASS threshold was determined by selecting the cutoff that maximized the Youden J statistic (defined as sensitivity + specificity – 1). Patients were classified as meeting the PASS if the value of the outcome score in question at final follow-up met or exceeded the cutoff score as calculated above.
Calculation of the SCB was also performed using an anchor-based method. Previous evidence has demonstrated that both pain- and physical function–related questions are acceptable as anchor questions to identify clinically meaningful improvements in pain and function. 23 To determine the SCB for the SANE, Rowe score, and ASES score, at final follow-up, patients were asked the following anchor question: “Since your surgery, how would you rate your overall physical activity?” To determine the SCB for the VAS pain, at final follow-up, patients were asked the following anchor question: “Since your surgery, how would you rate your overall shoulder pain?” Patients answering “much improved” were classified as the substantially improved group, while those answering “improved” or “slightly improved” were classified as the improved group. Patients answering “no change,”“slightly worse,”“worse,” or “much worse” were classified as the unimproved group. Using similar ROC curve analysis methodology as was employed to calculate the PASS, the SCB threshold was determined by selecting the absolute cutoff that maximized the Youden J statistic to establish the difference between patients in the unimproved group and the substantially improved group. Patients were classified as achieving the SCB if the change in the outcome score from preoperatively to final follow-up met or exceeded the cutoff score as calculated above.
Statistical Analysis
All statistical analyses were performed with RStudio (Version 2023; Posit). Continuous variables were reported as the mean ± standard deviation, whereas categorical variables were reported as the frequency and percentage. The paired-samples t test was used to compare preoperative and postoperative outcome scores. Statistical significance was set at alpha <.05. Nonparametric ROC and area under the curve (AUC) analyses were conducted to calculate the PASS and SCB using the anchor-based method. The degree of association was considered acceptable if the AUC was >0.7 and excellent if the AUC was >0.8.4,5 These values were then used to determine which patients in the cohort achieved the MCID, PASS, and SCB.
Univariate analysis was performed with respect to each demographic and preoperative variable using the chi-square or Student t test for categorical and continuous variables, respectively. Multivariate logistic regression analysis was performed for variables that achieved a P value <.15 on univariate analysis. Variables were considered significant predictors of achieving clinical significance if the final P value was <.05. Odds ratios (ORs) and 95% confidence intervals were calculated for each demographic and preoperative variable with respect to achieving the MCID, PASS, and SCB.
Results
During the study period, the senior author (N.P.) surgically managed 128 patients with posterior glenohumeral instability. Of these 128 patients, 17 underwent concomitant arthroscopic rotator cuff repair, 13 underwent concomitant SLAP repair, and 15 patients underwent a revision posterior stabilization procedure. An additional 10 patients were unable to be contacted for follow-up, leaving a total of 73 patients with a mean follow-up of 82.55 ± 24.20 months available for final analysis (Figure 1). Patient demographic and surgical data are summarized in Table 1. A statistically significant increase was noted in all postoperative PROM scores. Furthermore, the VAS pain score improved significantly at final follow-up (Table 2).
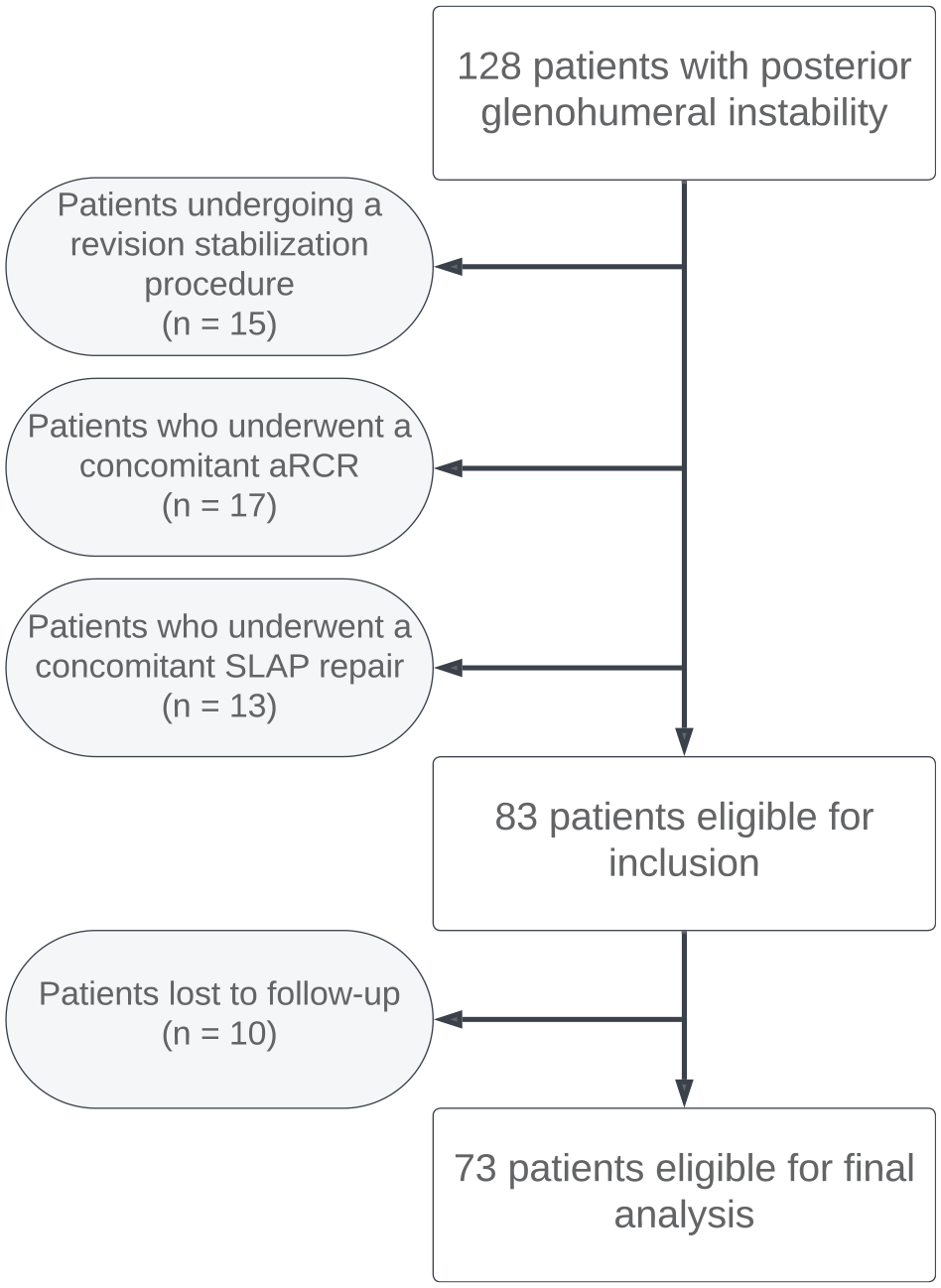
Flowchart of patient inclusion.
Patient and Surgical Characteristics
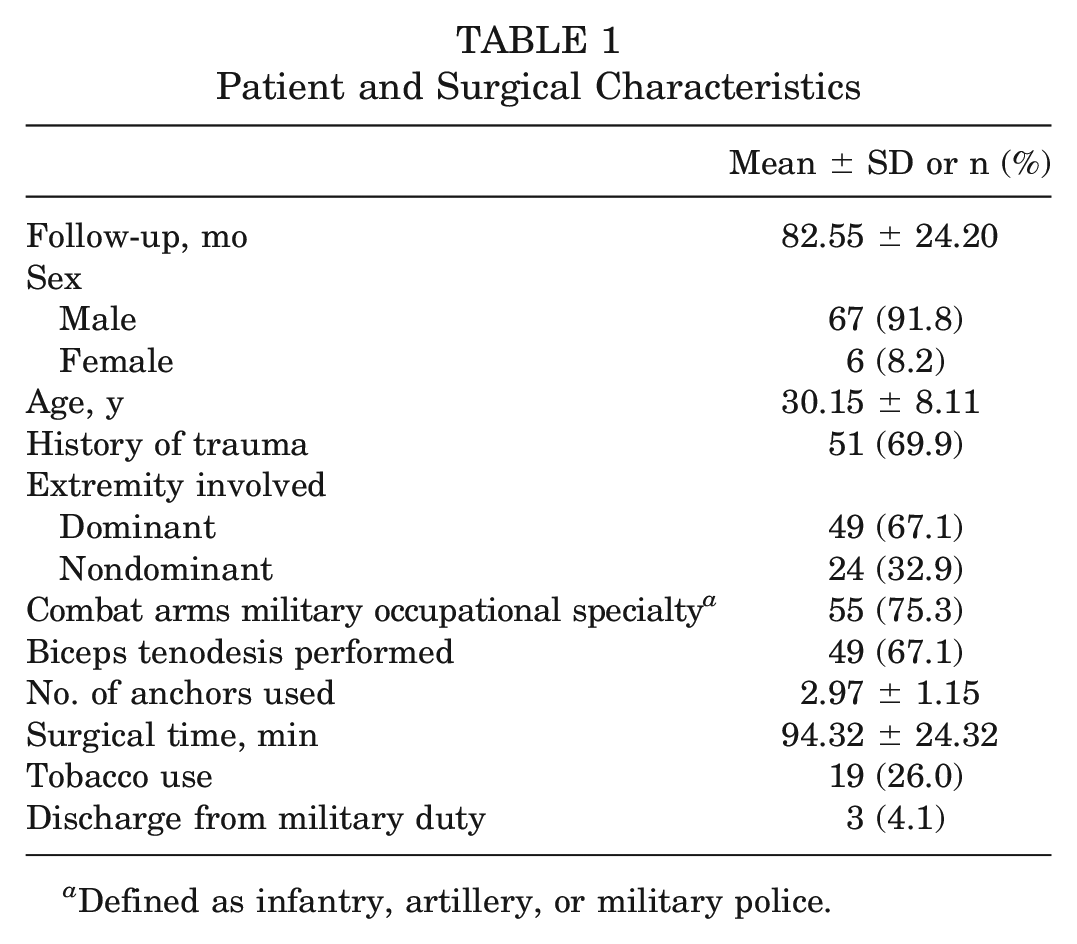
Defined as infantry, artillery, or military police.
Preoperative and Postoperative Outcome Scores a
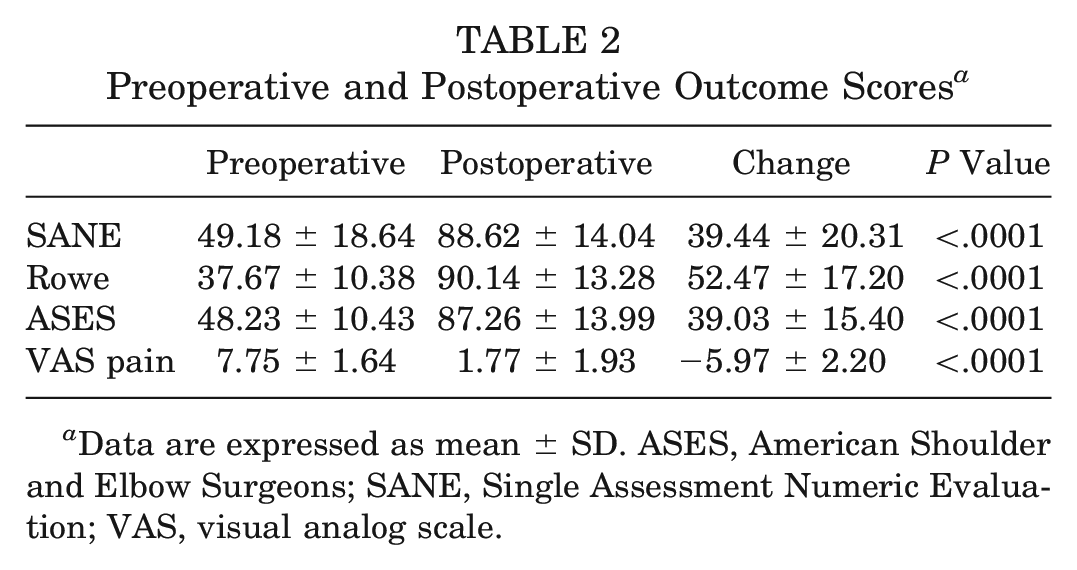
Data are expressed as mean ± SD. ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
The calculated MCID, PASS, and SCB values for the SANE, Rowe score, ASES score, and VAS pain, in addition to the sensitivity, specificity, and AUC for the respective ROC curves, are summarized in Table 3. The frequency with which patients in our cohort achieved a clinically meaningful improvement based on the various outcome scores and threshold values is summarized in Table 4.
MCID, PASS, and SCB Threshold Values a
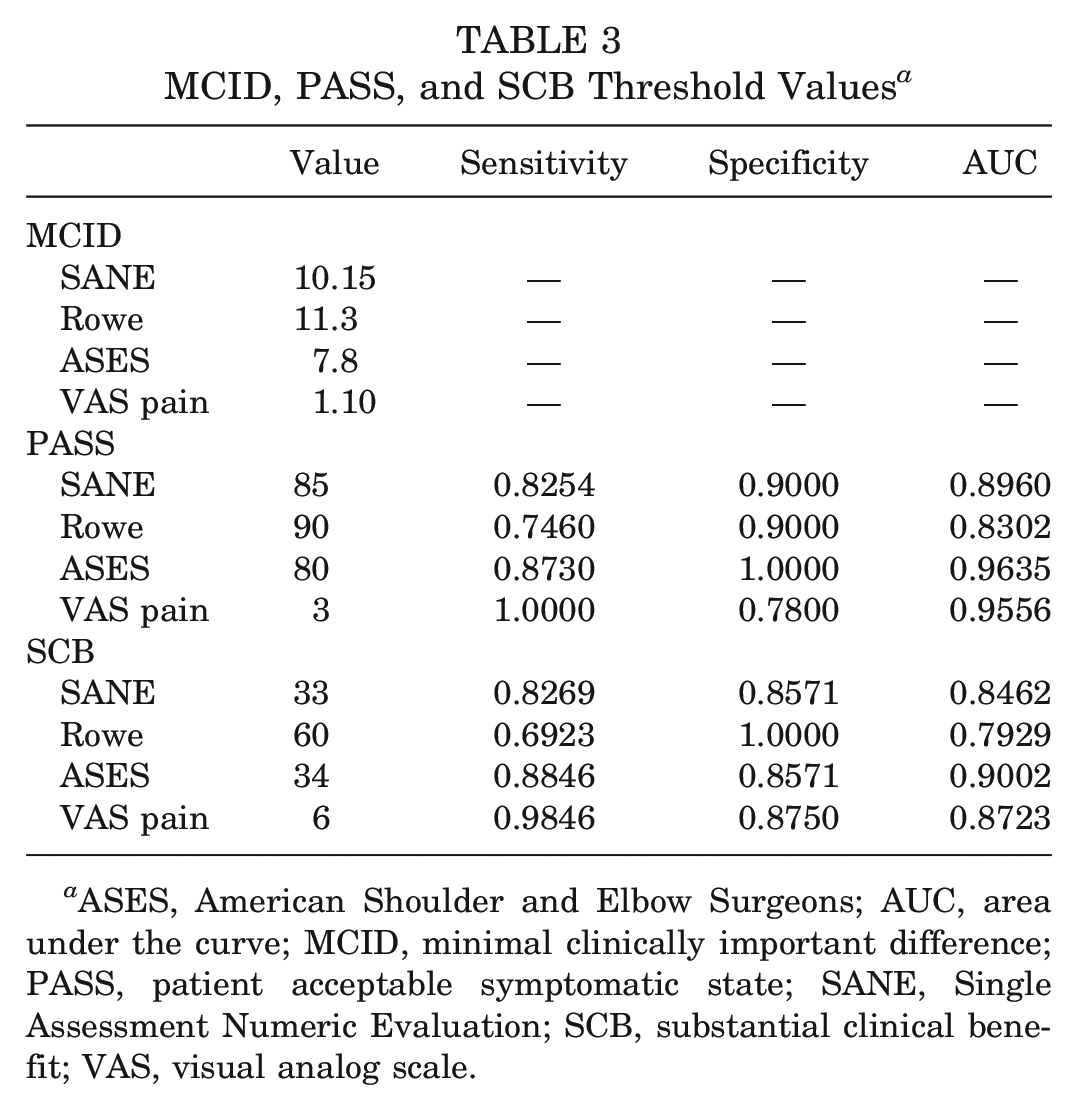
ASES, American Shoulder and Elbow Surgeons; AUC, area under the curve; MCID, minimal clinically important difference; PASS, patient acceptable symptomatic state; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit; VAS, visual analog scale.
Patients Achieving Clinically Significant Improvement at Final Follow-up a
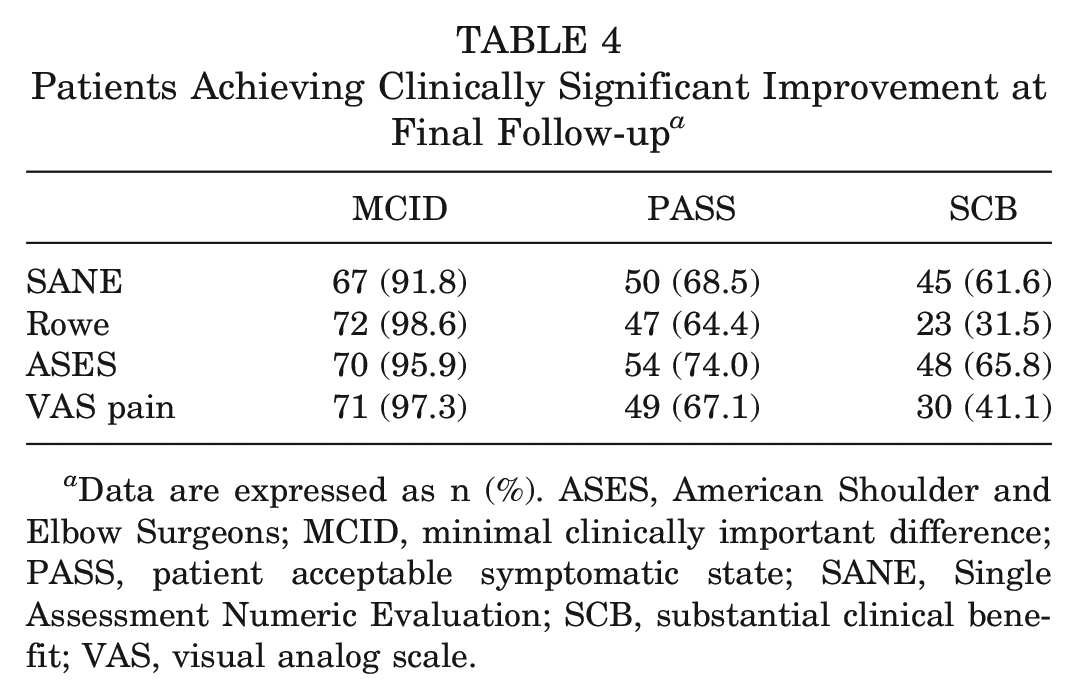
Data are expressed as n (%). ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; PASS, patient acceptable symptomatic state; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit; VAS, visual analog scale.
Logistic regression analysis was performed to determine the demographic and surgical factors associated with achieving clinical significance. Univariate analysis for all collected data and for factors with a univariate P value <.15, subsequent multivariate analysis were performed. For achieving the MCID, male sex (OR, 1.1639; P = .0293) was found to be a positive predictor for the VAS pain, and preoperative SANE score (OR, 0.9939; P = .0003) was found to be a negative predictor for the SANE (Table 5).
Logistic Regression of Variables Associated With Achieving MCID a
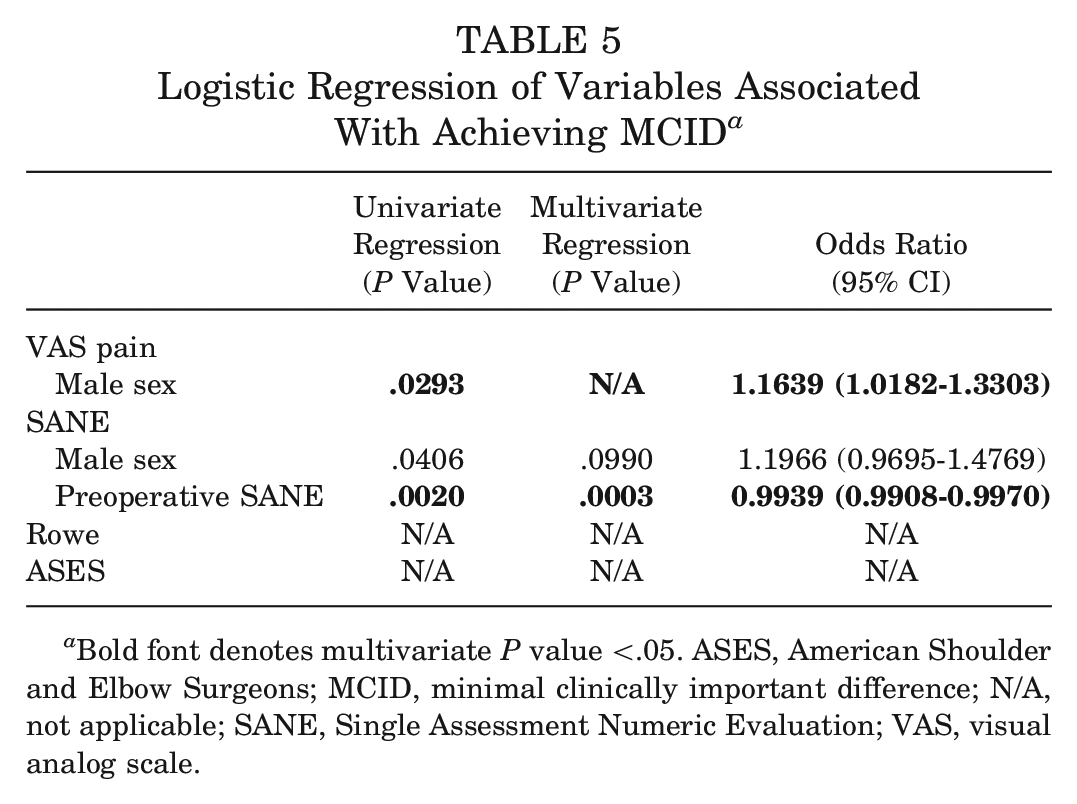
Bold font denotes multivariate P value <.05. ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; N/A, not applicable; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
For achieving the PASS, dominant arm involvement (OR, 0.7887; P = .0436) was found to be a negative predictor for the VAS pain, and a history of shoulder trauma (OR, 1.3507; P = .0104) was found to be a positive predictor for the VAS pain. For both the SANE and Rowe score, a history of shoulder trauma (OR, 1.3501; P = .0089 and OR, 1.3938; P = .0052, respectively) and concomitant biceps tenodesis (OR, 1.3825; P = .0038 and OR, 1.4040; P = .0035, respectively) were found to be positive predictors. For the ASES score, dominant arm involvement (OR, 0.7834; P = .0259) was found to be a negative predictor, and a higher preoperative ASES score (OR, 1.0107; P = .0324) was found to be a positive predictor (Table 6).
Logistic Regression of Variables Associated With Achieving PASS a
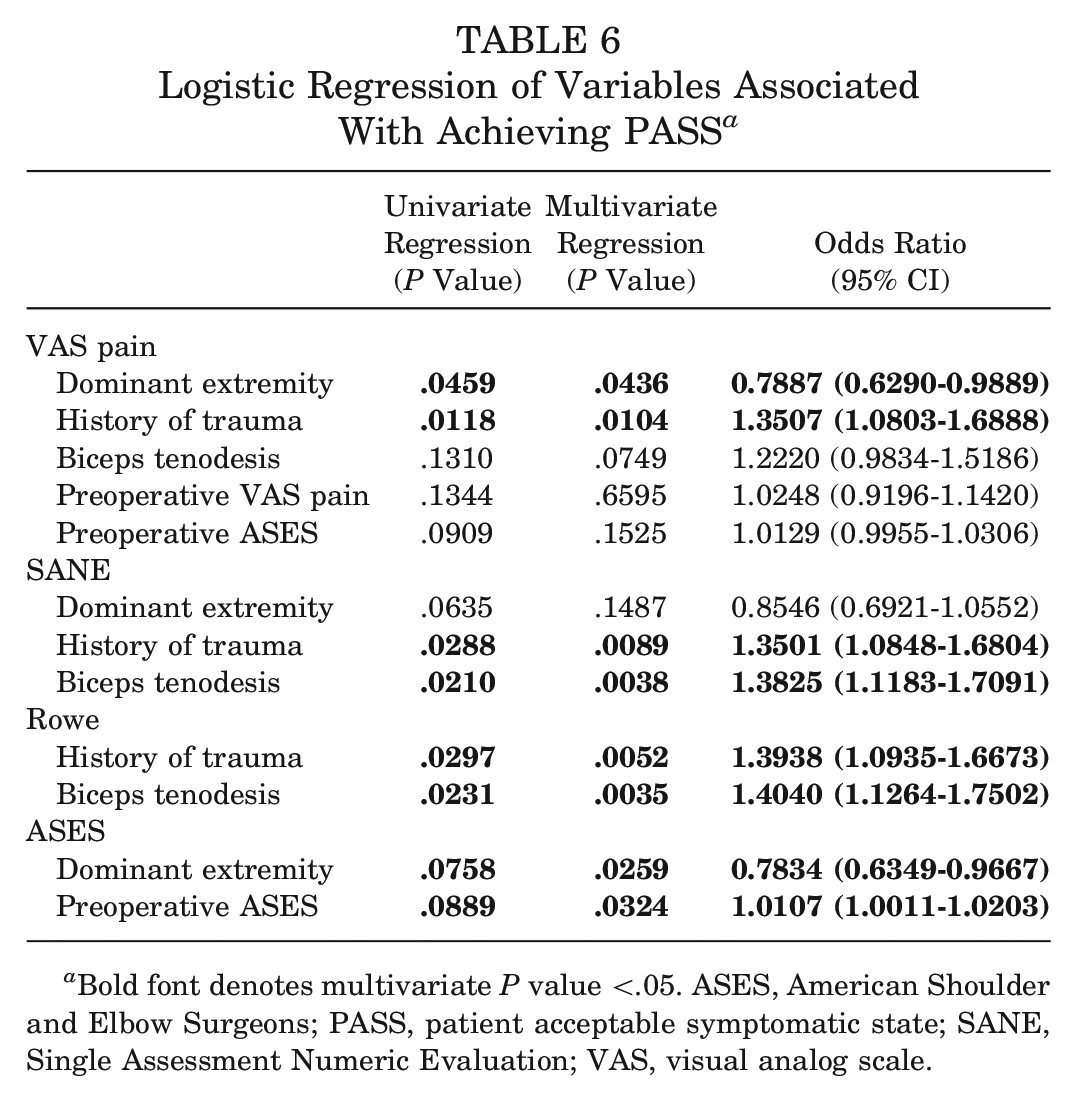
Bold font denotes multivariate P value <.05. ASES, American Shoulder and Elbow Surgeons; PASS, patient acceptable symptomatic state; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
For achieving the SCB, a history of shoulder trauma (OR, 1.2554; P = .0444) was found to be a positive predictor for the SANE, and a higher preoperative SANE score (OR, 0.9908; P = .0037) was found to be a negative predictor for the SANE. For the Rowe score, a higher preoperative Rowe score (OR, 0.9816; P = .0004) was found to be a negative predictor, and a higher preoperative VAS pain score (OR, 1.1282; P = .0175) was found to be a positive predictor. For the ASES score, both a history of shoulder trauma (OR, 1.2642; P = .0469) and concomitant biceps tenodesis (OR, 1.3490; P = .0130) were found to be positive predictors (Table 7). Predictors that reached statistical significance for more than one meaningful improvement metric are detailed in Table 8.
Logistic Regression of Variables Associated With Achieving SCB a
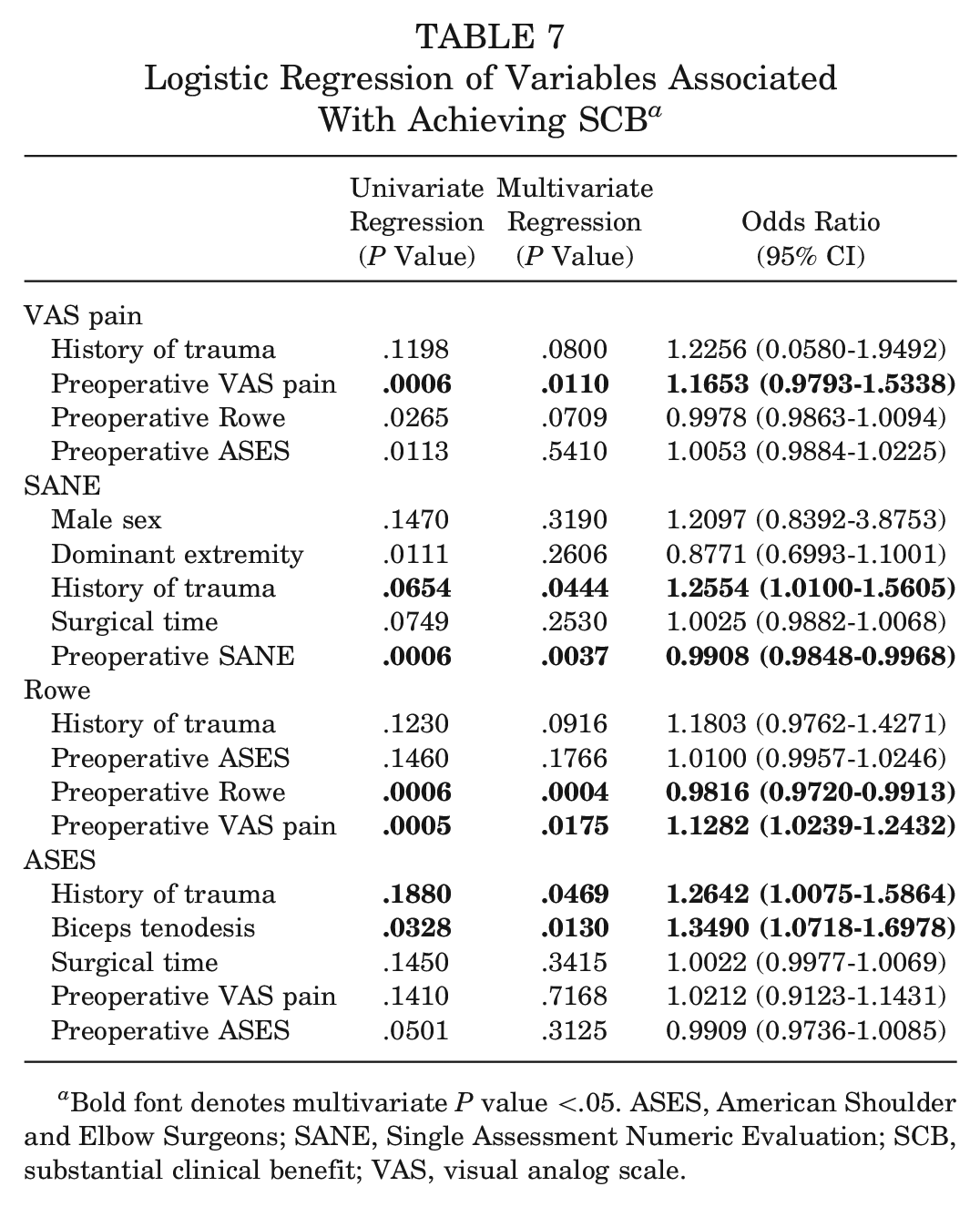
Bold font denotes multivariate P value <.05. ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit; VAS, visual analog scale.
Notable Predictors of Achieving Clinically Significant Outcome a
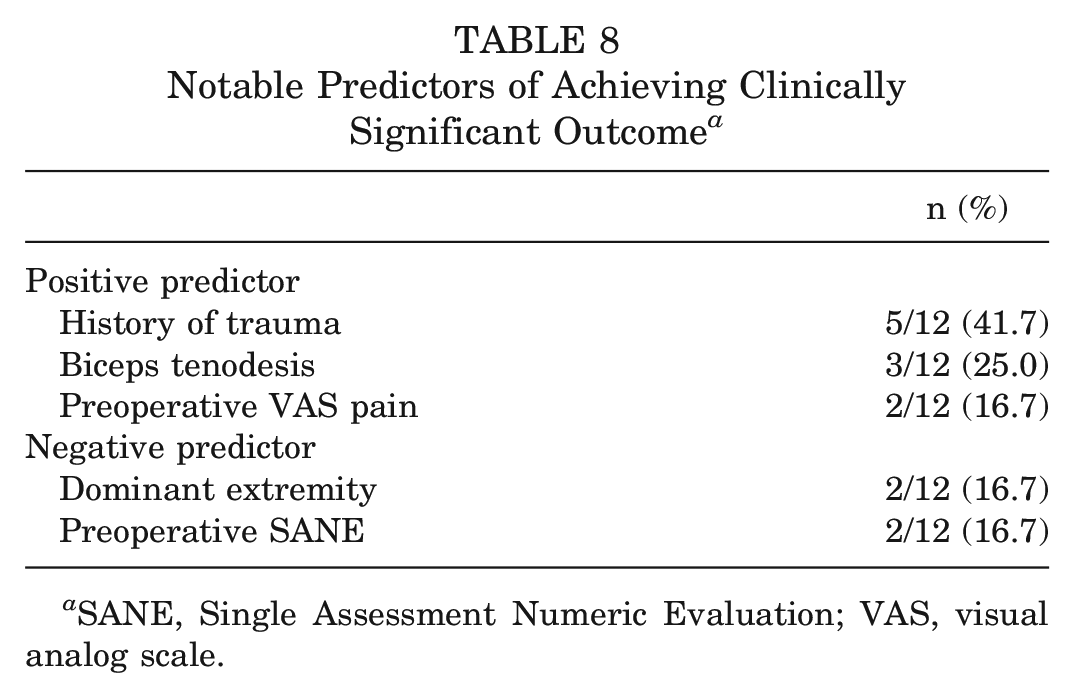
SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
Discussion
The results of this study defined the MCID, SCB, and PASS for the ASES score, Rowe score, SANE, and VAS pain after aPLR. Regarding factors affecting the likelihood of achieving clinical significance, dominant arm involvement was found to be associated with lower odds of achieving the PASS for the ASES score and VAS pain. In support of our hypothesis, a history of shoulder trauma was associated with an increased likelihood of reaching the PASS for the VAS pain, SANE, and Rowe score. Additionally, patients who underwent concomitant biceps tenodesis were more likely to achieve the PASS for the SANE and Rowe score.
A posterior labral abnormality is an increasingly recognized cause of shoulder pain and dysfunction. While initially thought to comprise only 2% to 10% of instability cases, recent studies have suggested that posterior instability may account for up to a quarter of cases in highly active populations.29,35,37,41 Military populations are known to suffer a disproportionately high incidence of posterior labral abnormalities compared with their civilian counterparts, likely attributable to the high-demand shoulder activities, such as push-ups and bench presses, required as a part of routine military training.17,32 As such, soldiers represent a unique opportunity to study posterior instability, and several studies have reported outcomes after aPLR in military cohorts. Scanaliato et al 32 demonstrated significantly improved outcomes in a cohort of young military patients at midterm follow-up, with over 90% of patients returning to active-duty military service. Similar outcomes were noted by Hines et al, 17 who reported high rates of return to active duty and low reoperation rates in a cohort of active-duty service members at a mean of 4.5 years’ follow-up. However, these existing studies have been forced to rely on clinical significance thresholds derived from procedures after surgical repair of other glenohumeral abnormalities and therefore may incorrectly characterize the clinical significance of these outcomes.
To our knowledge, this study is the first to report clinical significance thresholds after aPLR; however, previous studies have reported on these values after anterior stabilization. Park et al 25 calculated the MCID for the Rowe score to be 9.7 in 198 patients using an anchor-based method and 5.6 using a distribution-based method after arthroscopic Bankart repair. In another publication by Park et al, 26 the authors calculated the MCID for the ASES score to be 8.5 after Bankart repair using an anchor-based method. A recent study by Menendez et al 22 reported on clinical significance thresholds in patients undergoing the Latarjet procedure. MCID values for the ASES score, SANE, and VAS pain were found to be 9.6, 12.4, and 1.7, respectively, and PASS values for the ASES score, SANE, and VAS pain were 86.0, 82.5, and 2.5, respectively. 22 These values align with those observed in the present study and suggest that similar thresholds may exist for aPLR compared with those utilized for anterior shoulder instability. Concerning superior labral and biceps abnormalities, Puzzitiello et al 30 examined 123 patients who underwent isolated biceps tenodesis and calculated the MCID, SCB, and PASS for the ASES score to be 11.0, 16.8, and 59.6, respectively. For the SANE, the MCID, SCB, and PASS were calculated to be 3.5, 5.8, and 65.5, respectively. 30 While our values deviate somewhat from those reported after isolated biceps tenodesis, this may be attributable to the inherent differences between posterior and superior labral abnormalities. Additionally, differences in the study design and the active-duty military status of our cohort may contribute to discrepancies between threshold values. Ultimately, large prospective studies are needed to definitively define clinical significance thresholds; however, the findings of this study provide a much needed framework for interpreting PROMs after posterior labral repair.
A secondary purpose of this study was to identify variables associated with increased or decreased odds of achieving clinically significant improvements on PROMs. Regarding negative predictors, dominant arm involvement was noted to be associated with significantly lower odds of achieving a clinically meaningful improvement in outcome scores. This finding is intuitive, as functional demands are often greater of the dominant extremity. Concerning positive predictors, patients who reported a history of shoulder trauma were significantly more likely to achieve the PASS for the VAS pain, SANE, and Rowe score. This is of particular interest, as in contrast to anterior instability, frank posterior dislocation is uncommon with posterior instability. Rather, posterior instability more often results from repetitive posterior subluxation, microtrauma, or ligamentous laxity with an insidious onset.3,29,32 However, it is possible that patients who suffer an acute, traumatic injury may seek surgical treatment in a more timely manner compared with those whose instability is secondary to a degenerative mechanism. Additionally, the labral and capsular sequelae of chronic posterior instability may be less amenable to repair, and chronic instability has been associated with increased glenoid bone loss.3,11,28 Recent evidence supports a shorter time to operative stabilization in young, active patients with Bankart lesions, with timely operative interventions shown to both improve functional outcomes and decrease the risk of recurrent instability.1,40 While further research is necessary to fully understand the nature of this relationship in the setting of posterior instability, it is plausible that timely stabilization may be advantageous in these patients as well. Finally, concomitant biceps tenodesis at the time of posterior labral repair in patients with biceps abnormalities was found to increase the likelihood of achieving clinical significance thresholds. The biceps tendon represents a known pain generator, and many patients with superior labral abnormalities who undergo SLAP repair eventually require revision tenodesis.10,27,31 These findings suggest that removing pain-generating tissue with simultaneous tenodesis at the time of posterior labral repair may help to alleviate pain and increase function in appropriately selected patients. Furthermore, this finding aligns with existing literature, as combined biceps tenodesis and posterior labral repair has been demonstrated to produce favorable outcomes in patients with type VIII SLAP lesions. 13
This study was not without its limitations. First, the small sample size, predominantly male cohort, and retrospective nature of the investigation represent inherent sources of bias in our analysis. Additionally, all procedures were performed by a single shoulder and elbow fellowship-trained surgeon on an exclusively active-duty military patient population, potentially limiting the generalizability of our findings to broader populations. Outcome data utilized in this analysis were collected at a mean time point postoperatively rather than during a predefined window. Because of the nature of our database, details regarding the traumatic cause or number of dislocation events were not available for analysis. Regarding our statistical analysis, MCID, SCB, and PASS values may be calculated using various methods, and as such, different threshold values may exist depending on the scoring system used. Further studies in other patient populations utilizing different calculation methods are warranted to definitively characterize clinically meaningful improvements in patients undergoing aPLR. Lastly, our analysis also did not account for additional variables that may influence postoperative outcomes and satisfaction, such as mental health and patient expectations.
Conclusion
This study is the first to define the MCID, SCB, and PASS for ASES score, Rowe score, SANE, and VAS pain in patients undergoing aPLR. Furthermore, we found that patients who reported a history of shoulder trauma and those who underwent concomitant biceps tenodesis were more likely to achieve clinical significance. Dominant arm involvement was associated with lower odds of achieving clinical significance. Altogether, the findings of this study will allow surgeons to better understand the clinical significance of outcomes after posterior labral repair as well as appropriately counsel patients regarding postoperative expectations.
Footnotes
Submitted May 25, 2023; accepted September 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.P.S. has received hospitality payments from Stryker. C.M.H. has received consulting fees from Miach and Ossia, has received a gift from Wright Medical Technology, and holds stock in Activas Orthopedics. N.P. has received consulting fees from DePuy Synthes. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.