
Abstract
Background:
Recurrent patellofemoral joint instability in adolescent and young adult patients is associated with several anatomic risk factors. A lack of consensus exists as to which risk factor(s) should be addressed at the time of surgery, but the presence of a severely dysplastic femoral trochlea has been described as an indication for surgical intervention. Furthermore, literature has suggested that a severely dysplastic trochlea can be a contributing factor to a failed medial patellofemoral ligament reconstruction (MPFLR) alone.
Purpose:
To investigate the postoperative outcomes of patients <20 years of age who underwent primary trochleoplasty in combination with MPFLR and lateral retinacular lengthening (LRL), with some receiving concomitant tibial tubercle osteotomy (TTO).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective review of prospectively collected data performed in patients <20 years old who underwent trochleoplasty with MPFLR with ≥2 years of follow-up. Demographics, concomitant procedures, patient-reported outcome (PRO) measures, magnetic resonance imaging, and radiographs were reviewed. Patients who also underwent TTO were compared with those who did not.
Results:
A total of 21 knees from 15 patients (11 female, 4 male) with mean age of 16.4 years (13.7-19.8 years) were included. All patients had severe trochlear dysplasia and were treated with trochleoplasty, MPFLR, and LRL. Ten knees underwent additional TTO and were compared with those who did not (n = 11). The Pediatric International Knee Documentation Committee, Kujala, and Lysholm scores collected at a mean of 3.3 years (range, 2-6 years) postoperatively did not differ significantly between groups. There were no patient-reported postoperative episodes of patellar instability by the final follow-up.
Conclusion:
At a minimum 2-year follow-up, there were no statistically significant differences observed in PROs between patients who underwent trochleoplasty and concomitant TTO and those who had trochleoplasty alone, with neither group having any reported episodes of postoperative patellar instability. Furthermore, at final follow-up favorable PROs were achieved in patients who underwent trochleoplasty for the treatment of their patellofemoral instability with severe trochlear dysplasia.
Keywords
Recurrent patellofemoral joint instability often presents during the second decade of life. Patellar tracking is a complex interaction of soft tissue and bony restraints whose contributions to stability change as the knee progresses through its range of motion. Because of this, recurrent patellofemoral instability can arise from multiple etiologies. These etiologies can occur singularly or in combination and range from medial patellofemoral ligament incompetence, patella alta, increased tibial tubercle–trochlear groove (TT-TG) distance, and severe trochlear dysplasia.7,23 While simple first-time traumatic patellar dislocations can often be treated with nonoperative management alone, recurrent dislocations have deviations from the normal soft tissue and bony patellar restraints that require surgical correction.9,22,34 Medial patellofemoral ligament reconstruction (MPFLR) has been established as a safe and effective way of addressing patellar instability19,21; however, this procedure addresses only the soft tissue restraints of the patella and does not address any dysmorphism of the trochlea. Past research suggests that patients with severely dysplastic trochlea are at higher risk of failing soft tissue–only operations such as the MPFLR. 1 Furthermore, preoperative J sign, which has been shown to be significantly correlated with trochlear dysplasia, has been an independent risk factor for MPFLR failure.27,36
This study aims to investigate the postoperative outcomes of patients <20 years of age who underwent primary trochleoplasty to address severe trochlear dysplasia in combination with MPFLR and lateral retinacular lengthening (LRL), with or without concomitant tibial tubercle osteotomy (TTO).
Methods
Data collection and manuscript creation were conducted using the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 33 This study is an institutional review board–approved retrospective review of prospectively collected data from a single urban tertiary institution’s database (Research Electronic Data Capture [REDCap]; Vanderbilt University). Inclusion criteria were patients <20 years of age who underwent a thin flap sulcus-deepening trochleoplasty3,17 with MPFLR/LRL between the years of 2017 and 2023. All patients had closed or nearly closed distal femoral physes. All surgeries were conducted by a single fellowship-trained orthopaedic surgeon specializing in pediatrics and sports medicine (J.A.S.), and all patients included had ≥2 years of follow-up with patient-reported outcome (PRO) measures (PROMs) collected. Exclusion criteria included previous patellofemoral reconstruction, adults aged ≥20 years, and instability secondary to underlying neuromuscular syndromes such as cerebral palsy or Down syndrome.
Trochleoplasty was indicated in patients who had ≥1 of the following findings: symptomatic recurrent lateral patellofemoral instability, apprehension with increased lateral glide patella (≥3 quadrants) at knee ranges of motion >60 degrees of knee flexion, a jumping J sign on physical examination that was demonstrated both when seated and when supine, a chronically subluxated or dislocated patella, and severe trochlear dysplasia. Severe trochlear dysplasia was defined as Dejour B or D dysplasia on lateral knee radiographs and magnetic resonance imaging (MRI) with a lateral trochlear inclination <11 degrees and presence of supratrochlear spurs (anterior trochlear prominence ≥3 mm).5,7 Figure 1 displays preoperative imaging of study patients with severe trochlear dysplasia.

Preoperative axial knee magnetic resonance images (left) with corresponding lateral radiographs (right) from 2 of the patients included in this study. The top panel demonstrates Dejour B trochlear dysplasia, and the bottom panel demonstrates Dejour D trochlear dysplasia.
Surgical Technique
Trochleoplasty was performed via a lateral approach through an approximately 5- to 6-cm vertical incision placed 1 cm lateral to the lateral patellar facet. A thin flap trochleoplasty3,17 was created by sharp periosteal elevation followed by cartilage elevation started with a handheld flexible osteotome and completed with a specialized 3-mm offset guide and high-speed bur. The trochlear depth was increased by cutting a V-shaped osteotomy of the anterior distal femur in line with the intercondylar notch to a depth of ~1 cm lateralizing the trochlear groove to decrease the TT-TG distance. The deepening was further fine-tuned with a handheld high-speed bur, thereby removing the supratrochlear spur. The thin flap elevated cartilage was then reduced to the subchondral osteotomized bone and fixated with 2-0 synthetic, absorbable, braided multifilament sutures folded to create a 6-strand area of suture material to mimic a tapelike material that was implanted with 3 bioabsorbable implants placed first at the superior aspect of the intercondylar notch, next the superolateral corner of the trochlea, and last at the superior trochlear cartilage bone junction in line with the first distally placed implant. The periosteum was then reapproximated with another synthetic, absorbable, braided multifilament suture and dressed with fibrin glue. Figure 2 illustrates an overview of the sulcus-deepening trochleoplasty.
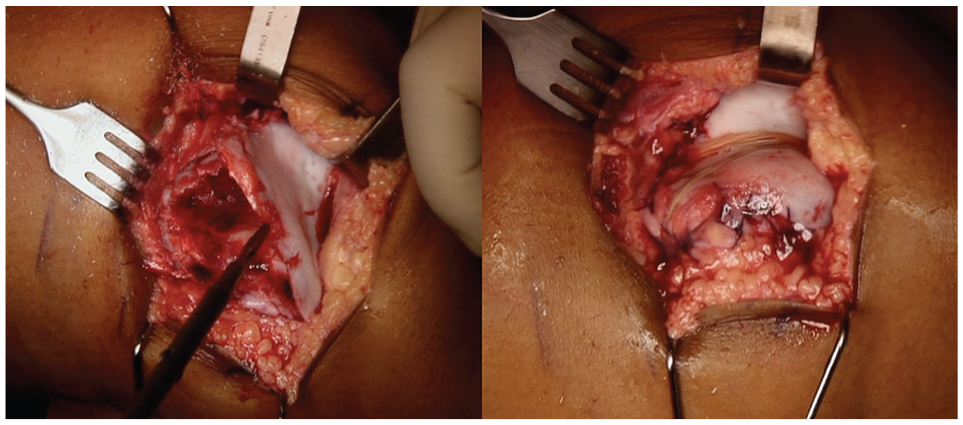
Intraoperative photographs of a trochleoplasty procedure with photographs of a sulcus-deepening trochleoplasty (Bereiter technique3,17) representative of the procedure performed on all study patients. The left panel illustrates the newly created sulcus with a high-speed bur. The right panel demonstrates the finished trochleoplasty after the osteochondral flap was secured and periosteum reapproximated using sutures and fibrin glue.
If the preoperative MRI TT-TG measurement was >20 mm, a TTO was performed after the completion of the trochleoplasty. Knees with an elevated TT-TG were anteromedialized, while those with an elevated TT-TG and patella alta above a Caton-Deschamps index (CDI) of 1.2 received anteromedialization with distalization. This was done using a 45° osteotomy that gave a 1-cm anterior and medial shift, which was the senior author’s (J.A.S.) preferred method to get a larger surface area for healing. The osteotomized bone is fixated with two 4.5-mm partially threaded lag screws. For distalization, a similar cut was made with 1 cm of the distal osteotomy site cut with a sagittal saw and removed. This osteotomized bone was affixed with three 4.5-mm partially threaded lag screws. Knees that had a normal TT-TG but possessed abnormal patellar height did not receive a TTO. Last, attention was then turned to MPFLR, which was done in all study patients. The MPFLR 28 was performed by anatomic double-bundle reconstruction with semitendinosus allograft. Aperture fixation was achieved at both the femur and the patella using 4.75-mm biocomposite SwiveLock anchors (Arthrex) on the patella and a 6-mm × 23-mm biocomposite interference screw in the femoral socket after final graft tensioning.
Postoperatively, all patients were admitted to the hospital for overnight observation and prophylactic antibiotics and subsequently discharged. At the conclusion of the surgery, all patients regardless of procedure combination were allowed to toe-touch weightbear and were placed in a locked range of motion brace, to protect the surgical reconstruction, assist with return of terminal knee extension, and prevent flexion contracture. The brace was to be worn full-time and only removed for personal hygiene, physical therapy, home exercise in which immediate range of motion was allowed and encouraged, and use of a home continuous passive motion machine, which was provided in all cases. The range of motion brace was unlocked for ambulating at weeks 4 to 6 as quadriceps control returned and was discontinued after postoperative week 6. Return to sports and unrestricted activity was allowed at 6 months postoperatively.
Data Collection
The medical charts of patients who fulfilled the inclusion criteria were reviewed for demographic information and intraoperative records. Based on preoperative MRI TT-TG measurements >20 mm, a subset of patients who underwent trochleoplasty with MPFLR/LRL were indicated for concomitant TTO. Preoperative and postoperative MRIs and radiographs were used to assess Dejour classification, as well as measure TT-TG as seen in Figure 3, lateral trochlear inclination angle (LTI), and CDI.4-7 Intraoperative and postoperative records were reviewed for any complications, recurrent dislocations or subluxation, and patient functionality.

Preoperative tibial tubercle–trochlear groove (TT-TG) measurement with 2 superimposed preoperative magnetic resonance imaging axial views of the left knee from patient #10 in Table 1. The green lines demonstrate the TT-TG distance, referenced off the central/anterior apex of the intercondylar notch.
Patient-Reported Outcomes
All patients completed PROMs including the Pediatric International Knee Documentation Committee (Pedi-IKDC), Kujala, and Lysholm questionnaires at a minimum of 2 years after their operation, either at their postoperative clinic visit or via telecommunication. All included PROMs were scored on a 0 to 100 percentile scale, with a score of 100 indicating highest functionality. The Pedi-IKDC is a 92-point assessment gauging pediatric knee function evaluating domains including pain, instability, swelling, catching/locking, difficulties with knee flexion, and activity-specific functional impairments (eg, walking up or down stairs or sitting with knees flexed). 14 The Kujala Anterior Knee Pain Score (or Kujala) is a 13-item instrument designed to assess patellofemoral pain for adolescents and young adults. Domains include limp, support, walking, stairs, squatting, running, jumping, prolonged sitting with knees flexed, pain, swelling, abnormal painful kneecap (patellar) movements, atrophy of the thigh, and knee-flexion deficiency. 16 Finally, the Lysholm knee score is an 8-item instrument that assesses knee function. 32 Domains include limp, support, locking, pain, instability, swelling, and the patient’s ability to use the stairs and squat.
Statistical Analysis
Frequencies or percentages are reported for categorical variables. Mean and 95% CIs are reported for interval data. Categorical data were compared utilizing chi-square test or Fisher exact test. The nonparametric Mann-Whitney U test was utilized to compare continuous outcome variables between groups. Alpha was set at P < .05 to declare significance, and analyses were performed with SPSS Version 28 (SPSS Statistics for Windows; IBM Corp).
Results
A total of 21 knees from 15 patients suffering from recurrent patellofemoral instability were treated with trochleoplasty, MPFLR, and LRL. Ten knees had an additional TTO performed, with 3 knees undergoing anteromedialization of the tibial tubercle while 7 knees had anteromedialization with distalization of the tibial tubercle.
Demographics and Patellar Instability Characteristics
At the time of surgery, all patients were in their second decade of life with a mean age of 16.4 years (range, 13.7-19.8 years). All patients had closed or almost-closed distal femoral physes. The 10 knees that underwent TTO had a mean age of 17.2 (range, 14.9-19.8 years) while the mean age of the 11 patients who did not undergo TTO was 15.7 years (range, 13.7-19.2 years). No significant difference in patient age between groups existed (P = .06). No significant difference in body mass index (BMI) was seen (25.7 with TTO vs 24.5 without TTO; P = .86). Female patients comprised 15 knees and the other 6 were male. No difference was seen in the patient’s sex (60% female with TTO versus 81.8% female without TTO; P = .36) between the groups. For patient data including BMI, sex, laterality, or preoperative subluxation/dislocation episodes between the groups, refer to Table 1.
Patient Demographics and Study Data a

The individual patient’s preoperative characteristics including his or her respective demographics, imaging, and physical examination. BMI, body mass index; TT-TG, tibial tubercle–trochlear groove; LTI, lateral trochlear inclination angle; CDI, Caton-Deschamps index.
Indicates the patient had too many preoperative subluxation/dislocation events and was unable to provide an accurate number.
Unable to obtain due to severely displaced patella.
Imaging Characteristics
All patients had severe trochlear dysplasia with presence of supratrochlear spurs, with mean spur height of 6.2 mm (range, 5 to 8.3 mm). Eight of the knees were classified as Dejour B and 13 as Dejour D. No difference in amount of trochlear dysplasia between groups (P = .66). Preoperatively, the mean LTI was −1.8 (range, −22 to 9), the mean TT-TG was 19.4 (range, 8.6 to 32), and the mean CDI was 1.37 (range, 1 to 2.09). Analyses of imaging findings found no difference in preoperative LTI and CDI among the 2 groups (P = .97 and P = .22, respectively), but the preoperative TT-TG was significantly different (15.0 vs 24.3; P < .001). One patient lacked sufficient radiographs to calculate patellar height and was excluded from CDI analysis. Preoperative imaging findings and analyses are reported in Table 2.
Preoperative Imaging Findings a

Preoperative summary statistics and analysis between TTO and No TTO groups. Bold indicates statistically significant. LTI, lateral trochlear inclination; TT-TG, trochlear tubercle–trochlear groove; TTO, tibial tubercle osteotomy.
Postoperatively, the mean CDI was 0.97 (range, 0.8-1.17), which was a statistically significant decrease from the preoperative value of 1.37 (range, 1-2.09) (P < .0001). This was further evaluated in the group that underwent TTO and the group that did not, which both saw statistically significant postoperative decreases in the CDI. The TTO group’s initial CDI mean was 1.47 and the postoperative mean was 0.95 (P < .001). The non-TTO group’s initial CDI mean was 1.26 and the postoperative mean was 0.99 (P = .003). There was no statistical difference between the CDI of the TTO and non-TTO group pre- or postoperatively when compared with each other. Analysis of preoperative versus postoperative CDI is shown in Table 3.
Preoperative and Postoperative Patellar Height a

Effect of MPFLR plus trochleoplasty with or without TTO on CDI and its normalization of patella alta. Bold indicates statistically significant. CDI, Caton-Deschamps index; MPFLR, medial patellofemoral ligament reconstruction; TTO, tibial tubercle osteotomy.
n is different because 1 patient lacked a sufficient lateral knee radiograph because of a severely displaced patella.
Postoperative Period and PROs
PROMs were completed at mean follow-up of 3.3 years (range, 2-6 years), with no difference in follow-up duration between groups. The mean postoperative Pedi-IKDC was 87.9% (range, 50%-100%), Kujala 90.5% (range, 68%-100%), and Lysholm 90.9% (range, 56%-100%). The PROMs did not differ significantly when comparing the patients who underwent TTO with those that did not. PROMs and analysis are reported in Table 4. Furthermore, no patient reported any postoperative episodes of patellar instability at final follow-up. Five patients returned to the operating room postoperatively: 4 for manipulation under general anesthesia, 1 for wound dehiscence.
Postoperative Patient-Reported Outcomes at Minimum 2-Year Follow-up a

Postoperative patient-reported outcome measure summary statistics and between-group analysis of variance analysis (TTO vs no TTO) at a mean follow-up of 3.3 years. Scores are reported as percentages. Pedi-IKDC, Pediatric International Knee Documentation; TTO, tibial tubercle osteotomy.
Discussion
In our study, the trochleoplasty was performed in conjunction with MPFLR and LRL for each case. TTO was added when the TT-TG was >20 mm. While some research has suggested that isolated trochleoplasty is appropriate, it only addresses 1 domain of patellofemoral stability and increases the risk of requiring a return to the operating room for further supplementary procedures. This is supported by a recent systematic review that found that an isolated trochleoplasty resulted in a lower Kujala score, increased risk for postoperative redislocations, and return to the operating room compared with a trochleoplasty combined with MPFLR. 25 A second systematic review on adult patients found that trochleoplasty combined with MPFLR and extensor realignment provided high postoperative satisfaction with low postoperative dislocation rate. 2 While these studies supported our approach to addressing patellofemoral instability, our study addressed a younger patient population, exclusively adolescents and young adults.
In our study of 21 knees, the postoperative mean Pedi-IKDC of 87.9% (range, 50%-100%) falls within the range of recently published studies investigating PROMs after MPFLR alone (mean, 76.89%; range, 69.6%-89.2%).10,11,13,24,29,31,35 Included patients also completed the Lysholm and Kujala questionnaires with postoperative means of 90.9% (56%-100%) and 90.5% (68%-100%), respectively. These values were also found to be within the range of the published literature for MPFLR alone: 86.6% (84.3%-89.2%) for Lysholm10,31 and 90.6% (85.9%-95.6%) for Kujala.10,29,31,35 Given that our postoperative PROMs were within the range of the published PROMs for MPFLR alone, it indicates that our outcomes are comparable with reported outcomes from other standard patellar instability surgeries despite our significant level of trochlear dysplasia, but we acknowledge that this comparison is limited due to our lack of preoperative PROMs. Furthermore, no patients in our study reported any postoperative dislocation or subluxation events. Five patients suffered complications: 4 developed arthrofibrosis requiring manipulation under general anesthesia and 1 had a wound dehiscence.
Research has shown that when indicated, a TTO can realign the extensor mechanism, allowing better patellar tracking and reduce patellofemoral pressures, which can decrease degeneration of the articular cartilage. 18 This additional procedure is debated in the literature. Some advocate for it in conjunction with MPFLR while others argue that MPFLR alone is sufficient.26,30 Furthermore, there is debate on whether medialization of the tibial tubercle alone is adequate or if distalization is necessary. 37 Some studies have even indicated that in the setting of patella alta, another indication for TTO, MPFLR can be sufficient for normalizing patellar height.12,20 Our study found that the PROMs of patients who underwent TTO with distalization were not statistically different from the patients who underwent TTO alone. Furthermore, 15 knees had patella alta, and all had a reduction of their CDI postoperatively to within normal range (0.8-1.2). This normalization of the CDI postoperatively was found to be statistically significant for both patients who underwent TTO and patients who did not. However, we theorize that the primary reason for the decrease in the CDI in both the TTO and the non-TTO group is attributed to the reconstruction of the MPFL, as reported previously in the literature. 15 The 5 knees with normal patellar heights remained within the normal range postoperatively, with no knees developing patella baja.
Limitations
A limitation of this study includes its small sample size and being from a single center. Another limitation is its relatively short long-term follow-up with a mean of 3.3 years. In addition, this paper cannot comment on whether the TTO provides a direct benefit in conjunction with a trochleoplasty especially when considering a distalization procedure. We acknowledge that it may be sufficient to perform only an MPFLR concomitantly with a trochleoplasty in cases with abnormal TT-TG distance and/or patellar height as elucidated in recent study. 8 Due to the retrospective nature of the study, the only knee PROMs collected were Pedi-IKDC, Lysholm, and Kujala. In addition, the lack of preoperative PROMs for comparison is a limitation of this retrospective study. Future randomized studies using larger sample sizes, with complete preoperative and postoperative PROMs, should be conducted to validate these results. Finally, there are inherent biases with observational studies as well as cohort studies.
Conclusion
The aim of this study was to report PROs at a minimum of 2-year follow-up in patients who underwent trochleoplasty with or without anteromedialization. Trochleoplasty combined with MFPLR is a solution that remedies both bony and soft tissue pathology in chronic patellar instability in patients with high-grade dysplasia. After analyzing the data, we found that the patients who underwent trochleoplasty had good to excellent PROMS regardless of the inclusion of a TTO or not.
Footnotes
Final revision submitted September 10, 2024; accepted October 7, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.K. has received support for education from Empire Medical. J.A.S. has received speaking fees from Arthrex and support for education from Arthrex and Micromed. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the Children’s Hospital of Orange County In-house Institutional Review Board (IRB No. 1909107).