
Abstract
Background:
No biomechanical study has established the effect of different graft positions or bone block options on anterior glenohumeral joint stability.
Purpose/Hypothesis:
The purpose of this study was to compare graft choice (distal clavicular vs coracoid autograft for Latarjet) and position on stability of the bone block for anterior glenohumeral instability. It was hypothesized that both grafts would be comparable if flush with the glenoid but that the sling effect of the Latarjet procedure would lead to greater stability in case of graft medialization.
Study Design:
Controlled laboratory study.
Methods:
Eight cadaveric shoulders were included. Defects stabilized using a distal clavicular graft and a coracoid graft were consecutively positioned at 0, 4, and 8 mm medially. The starting position was determined by the humeral head’s being seated at its most medial position on the glenoid surface. Each experiment comprised maximal external rotation and glenohumeral abduction at 60° while applying a constant 50-N medial compressive force to the humerus under all conditions. The conjoint tendon was routed through a split in the subscapularis and loaded with a 5-N weight using a pulley system for all Latarjet trials to simulate the sling effect.
Results:
Regarding the clavicular graft, the stability ratio significantly decreased versus the intact condition at all medial offsets (P = .007 for 0 mm, P < .001 for 4 mm, and P < .001 for 8 mm), and it was significantly lower in the 4-mm versus 0-mm position (P = .008), significantly higher in the 4-mm versus 8-mm position (P < .001), and significantly lower in the 8-mm versus 0-mm position (P < .001). Regarding the coracoid graft, the stability ratio was comparable with intact for the 0-mm position (P = .12), while it was significantly lower in the 4-mm and 8-mm positions (P < .001 for both). The distal clavicular graft at 0-mm offset was comparable with the coracoid graft at 0-mm offset.
Conclusion:
In shoulders with anterior glenoid bone loss, the coracoid and distal clavicular autografts were biomechanically comparable when placed flush with the glenoid. The distal clavicle at 0-mm offset did not restore stability compared with the intact specimen, but the Latarjet at 0-mm offset was not significantly different from the intact condition.
Clinical Relevance:
The Latarjet procedure provides higher stability compared with distal clavicular autograft when medialized.
The prevalence of bony defects on both the glenoid and the humeral side is very high in patients with recurrent anterior shoulder dislocation. 10 Glenoid bone loss has been shown to be the most common factor leading to recurrent shoulder instability and poor functional results after soft tissue repair,3,10,19 and different bone block procedures have been described to address this problem.14,20,21,24,25 The critical amount of glenoid bone loss that warrants a bone block procedure has traditionally been considered over 20%,4,7,19 but more recent studies emerged stating that this threshold could be as low as 13.5%, especially in high-demand patients. 21
Multiple anterior glenoid bone block techniques have been described using either allogenic or autogenic bone graft: the Latarjet or Bristow procedures, 14 iliac crest bone graft, 24 distal tibial allograft, 20 femoral head, 25 and more recently distal clavicular autograft. 23 Multiple studies have reported excellent results with various bone block procedures for anterior shoulder instability.2,5,11,15,22 However, bone block procedures are not universally successful, and graft malpositioning in reference to the remaining intact glenoid is a common cause of failure.1,8 Many believe that the optimal position of the bone block is flush with the glenoid rim. If the bone block is too lateral, it may contribute to the development of osteoarthritis, whereas if it is too medial, it may not be able to prevent recurrent instability.
The optimal position of a transferred coracoid during a Latarjet or Bristow procedure has been investigated. Nourissat et al 16 recommended in one biomechanical study that the bone block should be fixed in the middle of the anteroinferior quarter of the glenoid rim, at 4 o’clock, below the equator. Young et al 28 have suggested that the placement cranial to the equator might increase the sling effect of the conjoint tendon, which may be particularly helpful in patients with hyperlaxity. Despite the relative consensus concerning the optimal position of a transferred coracoid, no biomechanical study to our knowledge has studied whether this position differs for other types of bone block used.
The objective of the study was to compare the effect on glenohumeral stability of a distal clavicular autograft versus a coracoid autograft for the Latarjet procedure. We hypothesized that the effect of both grafts would be comparable if flush with the glenoid but that the sling effect of the Latarjet would lead to greater stability of the coracoid graft in case of graft medialization.
Methods
Specimen Preparation
A total of 8 fresh-frozen cadaveric shoulders of unknown age comprising the scapula and proximal humerus were obtained from the Mayo Clinic anatomical bequest program after institutional review board approval. The specimens were screened to exclude severe glenohumeral arthritis, rotator cuff tears, and joint contracture. Shoulders were dissected such that all superficial and subcutaneous soft tissue was removed except for the conjoined tendon, rotator cuff muscles, and joint capsule. A horizontal split was made in the subscapularis muscle for access to the anterior glenoid. Most of the medial scapular body was removed, with the remaining scapula potted in a rigid urethane resin (Smooth-Cast 300D; Smooth-On Inc) such that the rim of the glenoid that was parallel to the floor. The glenoid length and width were measured using a digital caliper for both the superoinferior and the anteroposterior dimensions. The potted glenoid was then mounted on a testing frame with the glenoid concave surface facing upward (Figure 1). The humeral shaft was potted using the same resin in a hollow tube for fixation to the testing apparatus such that humeral head could be seated on the glenoid.

Specimen mounted to stability test fixture with lateral scapula and proximal humerus potted in resin with loads applied to the subscapularis and the conjoined tendon.
Testing Conditions
Each specimen was tested according to the following 8 conditions: (1) intact/native shoulder (intact); (2) after creation of a 6-mm osseous glenoid defect in the anteroinferior edge of the glenoid 26 (bone defect); (3) stabilization of the defect with a distal clavicular bone block flush with the glenoid surface (0-mm clavicle); (4) stabilization of the defect with a distal clavicular bone block, medialized 4 mm (4-mm clavicle); (5) stabilization of the defect with a distal clavicular bone block, medialized 8 mm (8-mm clavicle); (6) stabilization of the defect using a Latarjet procedure, placing the coracoid bone block flush with the glenoid surface (0-mm Latarjet); (7) same as condition 6 but medialized 4 mm (4-mm Latarjet); and (8) same as condition 7 but medialized 8 mm (8-mm Latarjet).
The distal clavicular bone block was harvested after dividing the acromioclavicular capsule; the osteotomy was performed just lateral to the inferior insertion of the coracoclavicular ligaments. The graft was then aligned such that the acromioclavicular joint cartilage was parallel with the surface of the glenoid cartilage at the site of the glenoid bony defect and such that it did not extend inferiorly past the inferior edge of the glenoid. This was considered the 0-mm clavicular condition.
The coracoid graft for the Latarjet procedure was harvested by performing a coracoid osteotomy just lateral to the coracoid notch with the conjoint tendon remaining attached. The graft was aligned on the site of the glenoid bony defect such that it did not extend inferiorly past the inferior edge of the glenoid, with the lateral edge of the graft creating a continued contour of the glenoid. This was considered the 0-mm Latarjet condition.
All bone blocks were fixed in place using 2 No. 4-40 machine screws passing from the anterior (graft side) through the graft and through the glenoid neck, extending out the posterior side. A matching nut was then used to fix each screw and the graft in place (Figure 2). After the first 0-mm offset graft was aligned, 2 pilot holes for the mounting screws were drilled. Two more sets of pilot holes were then drilled 4 mm and 8 mm medial to the 0-mm offset holes (Figure 3). This allowed accurate positioning of the graft inferiorly on the glenoid. Using this machine screw, nut, and pilot-hole method prevented bone stripping and progressively poorer purchase that standard bone screws would have had after repeated graft mountings without compromising the graft fixation strength or rigidity for the duration of this study.

Schematic of 1 of the 2 screws used to fix the graft to the glenoid.

Example of how pilot-hole locations for the (A) 4-mm and (B) 8-mm offset grafts were made based on the hole used for the 0-mm offset graft.
Due to the irreversible changes associated with conditions 1 (intact) and 2 (bone defect), these conditions were always tested first and in numerical order. Then, all of the clavicular graft conditions (0-, 4-, and 8-mm medial offsets) were run before the Latarjet conditions (0-, 4-, and 8-mm medial offsets) so that the coracoid would remain in place during the clavicular graft conditions. Within these specifications, the order of the bone block placements was randomized. For each condition listed above, specimens underwent a joint stability test, described below.
Joint Stability Assessment
Joint stability was assessed using a custom-fabricated joint stability testing machine capable of recording the 3-dimensional (3D) forces and moments across the joint via a 6-component load cell (model 45E15A-E24ES-A; JR3) as well as the 3D position of the humerus relative to the glenoid using linear potentiometers (LCPL Open Frame Linear Potentiometer; State Electronics). The joints were mounted to the machine such that the humerus was in a position of maximal external rotation and glenohumeral abduction of 60°. The system applied a constant, 50-N medial compressive force via a pneumatic actuator to the humerus under all conditions. The starting position was determined by the humeral head’s being seated at its most medial position on the glenoid surface. A 20-N load was applied to the subscapularis for all conditions via a suture in the subscapularis tendon that was routed parallel to the muscle’s native line of action and pulled via a pneumatic actuator. The conjoint tendon was routed through a split in the subscapularis and loaded with a 5-N weight using a pulley system for all Latarjet trials to simulate the sling effect. The magnitude of these loads followed the study of Yamamoto et al. 27 Starting from this centered/medialized position, the humeral head was translated in the anterior direction at a rate of 2.0 mm/s at a distance of 14 mm. Reaction forces, anteroposterior glenoid displacement, and lateral humeral displacement data were recorded at a sample rate of 100 Hz.
Data Analysis
The force analysis was based on a normalized displacement proportional to the glenoid length. A 10-mm anterior displacement distance was used for the widest glenoid (25.8 mm), with the displacement distances for all other glenoids scaled down proportionately based on their glenoid width. The compression and translational reaction forces occurring at these normalized displacement positions were used to compute the stability ratio. The stability ratio was computed as the anterior translational force divided by the medial compressive force and was reported for each glenohumeral condition tested. The stability ratio at the normalized 10 mm of displacement was extracted from the data for analysis.
Statistical Analysis
A repeated-measures analysis of variance (ANOVA) was performed to compare the stability ratio at the normalized 10 mm of displacement between the 8 shoulder conditions, with appropriate Greenhouse-Geisser corrections applied based on the results of Mauchley sphericity tests. A Tukey honestly significant difference (HSD) post hoc test was performed in the event of statistically significant differences between conditions (P < .05).
Results
Overall Results
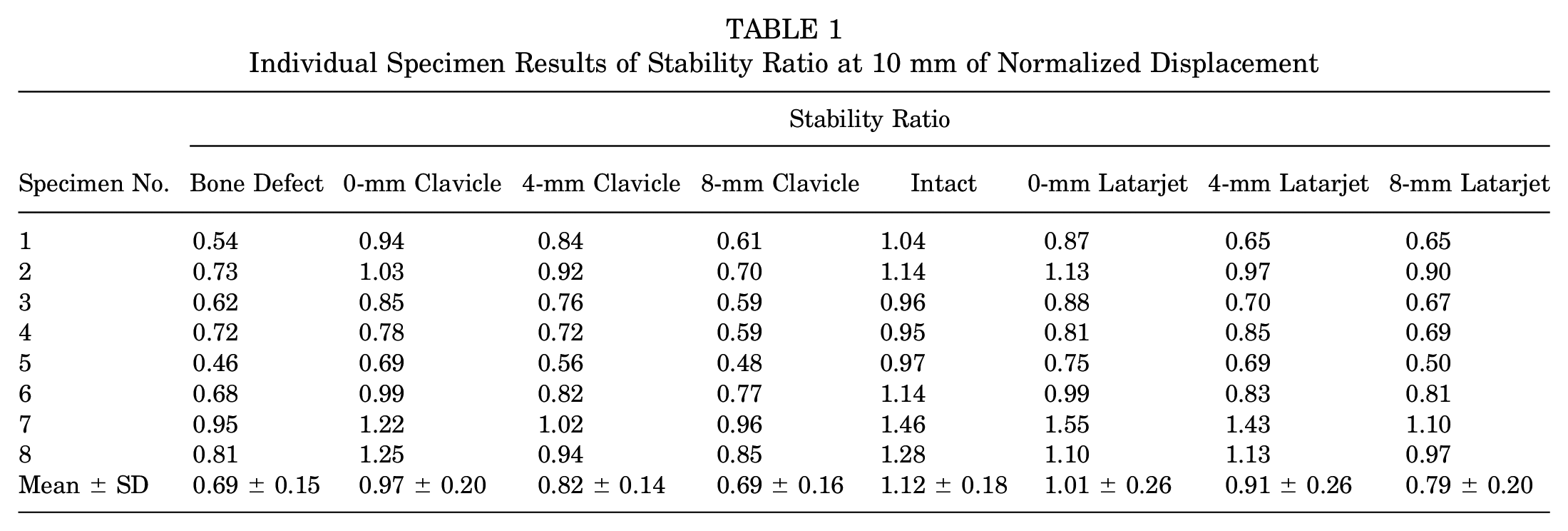
The mean results of the stability ratio at a normalized displacement of 10 mm for each shoulder condition are included in Figure 4. Figure 4A shows the mean value of each condition, including the intact condition, and the y-axis shows the stability ratio (tangential force/compression force). Figure 4B includes the stability ratio for each shoulder specimen normalized to its own intact condition, with the y-axis indicating the stability ratio as a percentage of the intact stability ratio. Table 1 summarizes the results obtained. There was a statistically significant effect of study condition (P < .001; repeated-measures ANOVA), with post hoc results of the Tukey HSD analysis between study conditions shown in Table 2.

(A) Stability ratio at 10 mm of normalized displacement and (B) stability ratio at 10 mm of normalized displacement with each specimen normalized to its own intact condition. The boxes represent the IQR, the black line represents the median, and the whiskers represent the range. Statistically significant differences (P< .05) versus the following conditions: a bone defect, b 0-mm clavicle, c 4-mm clavicle, d 8-mm clavicle, e intact, f 0-mm Latarjet, g 4-mm Latarjet, h 8-mm Latarjet.
Individual Specimen Results of Stability Ratio at 10 mm of Normalized Displacement
Statistical Results From Tukey HSD Post Hoc Analysis a
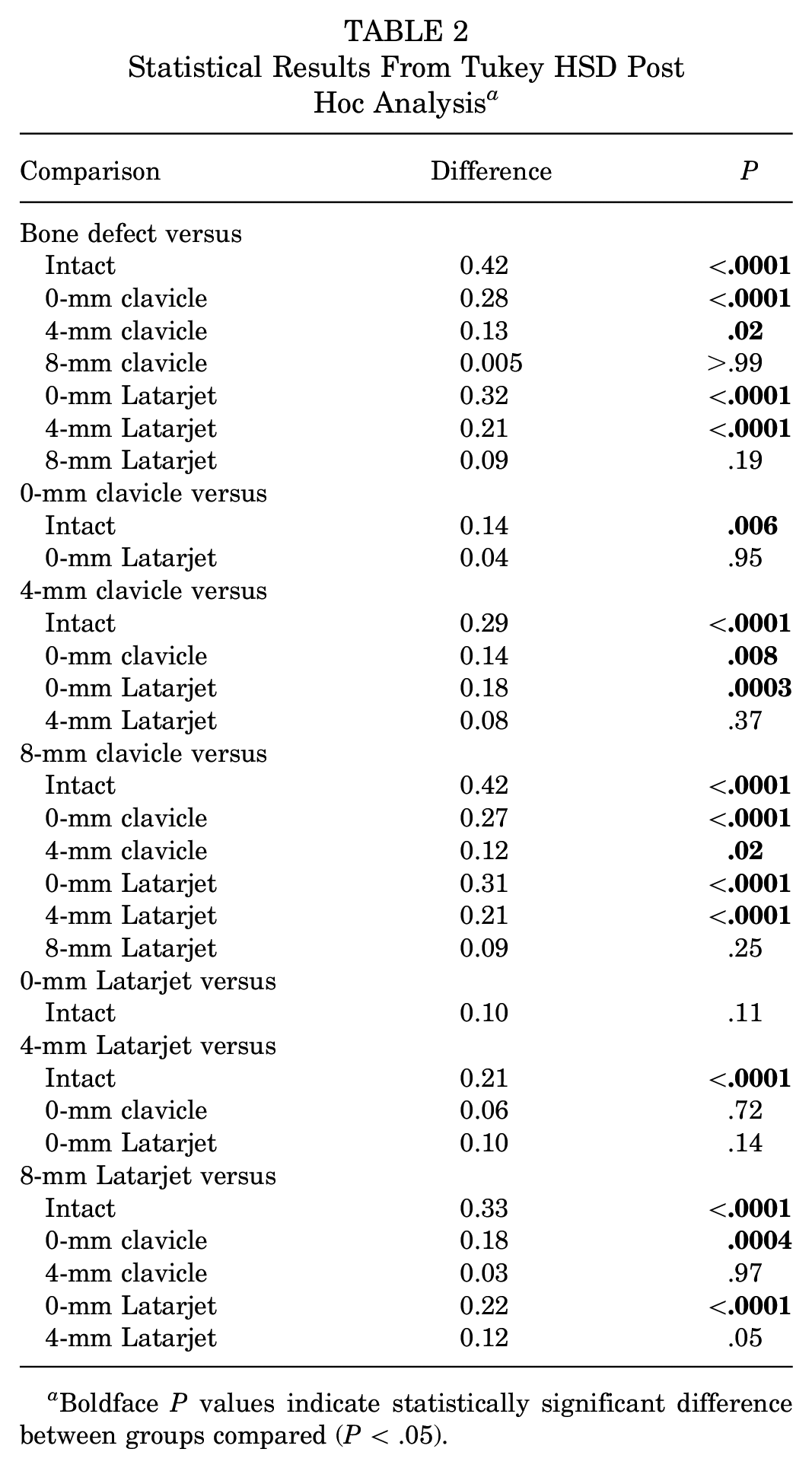
Boldface P values indicate statistically significant difference between groups compared (P < .05).
Individual plots of the stability ratios for each of the 8 cadaveric specimens are available in Supplemental Material Part 1, available separately. In addition, results of trials run with no subscapularis loading are shown in Supplemental Material Part 2.
The mean stability ratios of the specimens are shown in Figure 5A, and the stability ratios relative to an intact glenohumeral joint are shown in Figure 5B.

(A) The mean stability ratio of all the specimens depending on the position of each bone block and (B) the mean stability ratio of the specimens relative to an intact glenohumeral joint.
Distal Clavicular Autograft
The 0-mm and 4-mm clavicular conditions showed statistically significant increases in the normalized stability ratio relative to the bone defect condition (P < .001 and P = .02, respectively), while the 8-mm clavicular graft showed no significant difference when compared with the bone defect condition (P = .26). Clavicular grafts at all offsets showed a statistically significant decrease in the stability ratio versus the intact condition (P = .007 for 0-mm offset, P < .001 for 4-mm offset, and P < .001 for 8-mm offset). Within the clavicular graft conditions, the 4-mm offset had a significantly lower stability ratio versus the 0-mm offset (P = .008) and a significantly higher stability ratio than the 8-mm offset (P < .001). The 8-mm clavicular offset graft had a significantly lower stability ratio than the 0-mm offset (P < .001).
Coracoid Autograft
Compared with the intact condition, there was no significant difference in the normalized stability ratio between the coracoid graft in the 0-mm Latarjet condition (P = .12), while the stability ratios in the 4-mm and 8-mm Latarjet conditions were significantly lower (P < .001 for both). Relative to the bone defect condition, the stability ratios for both the 0-mm and the 4-mm Latarjet conditions were significantly greater (P < .001 for both), while there was no difference in the 8-mm Latarjet condition (P < .20). Within the Latarjet conditions, the stability ratio of the 4-mm offset position was not significantly different versus the 0-mm (P = .14) or 8-mm (P = .053) positions; however, the stability ratio of the 8-mm offset was significantly lower versus the 0-mm position (P < .001).
Distal Clavicular Versus Coracoid Graft
There was no significant difference in the normalized stability ratio between the clavicular and Latarjet conditions when comparing equal offset positions (P = .96 for 0-mm offsets, P = .38 for 4-mm offsets, and P = .26 for 8-mm offsets). The stability ratio was not significantly different between the 0-mm clavicular and 4-mm Latarjet conditions (P = .73). The 4-mm clavicular condition had a significantly lower stability ratio versus the 0-mm Latarjet condition (P < .0001); however, there was no significant difference versus the 8-mm Latarjet condition (P = .98). The 8-mm clavicular graft had a significantly lower stability ratio than both the 0-mm and the 4-mm Latarjet conditions (P < .001 for both).
Discussion
The results of the study indicate that compared with the intact glenoid, the distal clavicular graft did not restore stability at any position, whereas the coracoid graft in the 0-mm Latarjet condition was not significantly different from that of the intact glenoid, although offset medial placement of the Latarjet graft did not restore stability in comparison with the intact condition. However, there was no significant difference in stability ratio between the 0-mm Latarjet and 0-mm clavicular conditions. Thus, findings showed that coracoid autograft is preferable over distal clavicular autograft for restoring shoulder stability and that the graft should be positioned flush with the glenoid for maximal restoration of stability.
The outcome of bone reconstruction of the anteroinferior glenoid rim in patients with recurrent anterior instability may vary depending on the graft used and how accurate graft positioning is at the time of surgery. Traditional coracoid transfer procedures according to the Latarjet technique are considered by many the gold standard, with a number of benefits, including autograft nature, local harvesting, and the additional stability provided by the transferred conjoined tendon. Use of a distal clavicular autograft is appealing as well: it is still an autograft harvested locally and it provides cartilage, for a true osteoarticular autograft. In addition, the risk of injury to the musculocutaneous nerve is theoretically decreased. However, the Latarjet procedure seems to be more forgiving since it seems to better restore stability if placed flush with the glenoid rim.
Of the various surgical techniques described for reconstruction of the anterior glenoid rim, the coracoid graft and iliac crest graft are the most popular choices. The coracoid graft is harvested within the same incision and has the theoretical advantage of the sling effect that provides a dynamic stability. 27 The iliac crest autograft has excellent clinical results, but donor-site morbidity remains an issue. 15 Osteochondral allografts, such as the distal tibial allograft, provide a source of articular cartilage, but their cost and availability worldwide remain areas of concern. The distal clavicular autograft, described by Tokish et al, 23 has the advantage of being a source of articular cartilage with minimal additional increase in donor-site morbidity, but it lacks the dynamic stability of the sling effect provided by the Latarjet.
Few studies have compared the results of distal clavicular autograft with the coracoid autograft.9,12,18 Petersen et al 18 compared contact area and contact pressure differences between both grafts and found that the distal clavicle better reproduces contact pressure of the native glenoid. In addition, Kwapisz et al 12 showed that distal clavicular autograft provides a broader radius of reconstruction than that of a coracoid graft. Despite these differences, the current study shows that these 2 grafts have comparable stabilizing effect when they are positioned flush to the glenoid, but only the coracoid autograft seems to restore stability in comparison with the intact side. The sling effect of the conjoined tendon does not seem to significantly increase the stabilizing effect of the coracoid bone block over the distal clavicle.
These results are consistent with a 2019 clinical study from Moroder et al 15 in which no clinical differences were found between iliac crest and coracoid autografts, suggesting that the stabilizing effect of the conjoined tendon may not have a major effect on the stability conferred by bone-grafting procedures. Nevertheless, Giles et al 6 showed in a biomechanical study comparing the stability provided by a coracoid graft with and without conjoint tendon that glenohumeral stability was improved by the sling effect. Similarly, Yamamoto et al 27 showed that the mean contribution of the sling effect to stability was 51% to 62%. In the present study, we found that a slight medialization of a coracoid graft (4-mm medial offset) had no significant effect on glenohumeral stability, but it did not restore stability in comparison with the intact state, whereas a 4-mm medialization of the distal clavicular graft significantly decreased its stabilizing effect. This could be explained by the dynamic sling effect of the conjoint tendon, which may compensate excessive medialization of the bone block to some extent, as this appears to be no longer true when the graft is too medialized (8-mm medial offset). In theory, in the Latarjet procedure the sling effect provides dynamic support by the repositioning of the conjoint tendon, supporting the inferior humeral head. Patte and Debeyre 17 suggested that the Latarjet stabilizes the shoulder effectively by the triple-locking effect. Therefore, the results of the current study suggest that the sling effect does not provide any additional stabilizing effect when the bone block is positioned perfectly flush to the glenoid rim (as shown by Moroder et al 15 ). However, the sling effect could compensate the loss of stabilizing effect due an imperfect medial positioning of the bone graft.
Although the distal clavicular graft appears to have the advantage of using the articular cartilage of the acromioclavicular joint, slight medialization of the graft was found to significantly decreased its stability ratio in comparison with a perfectly aligned graft (0-mm medial offset). In addition, the distal clavicle is believed to have lower bone density in comparison with the coracoid graft 13 and has variable form and morphology. Larouche et al 13 argued that type 1 clavicles with a square morphology presented the best articular reconstruction characteristics, whereas type 3 clavicles were less likely to be effective. Of note, there are few long-term clinical and functional results regarding reoperation rate, functional outcomes, and donor-site morbidity for distal clavicular grafts.
Limitations
The study has several limitations. First, no standardized graft osteotomy was performed, and the thickness and length of the distal clavicular grafts was not recorded, although no graft was too large to cause superior or inferior overhang. Second, we investigated the effect of medialization of the bone block on the stability ratio, and all grafts were placed at the equator, even though Nourissat et al 16 showed a higher glenohumeral stability when grafts were placed below the equator at 4 o’clock. Third, although forces were applied, no muscle forces were present, and the study was conducted in a single-arm position. Finally, this was a biomechanical study, and further clinical studies are warranted to compare the outcomes of the 2 grafts and to identify the relative indication of each graft.
Conclusion
In shoulders with anterior glenoid bone loss, the Latarjet procedure and transfer of an osteoarticular distal clavicular autograft were biomechanically equivalent in restoring stability against anterior translation, provided both grafts were placed flush with the glenoid, although only the Latarjet procedure showed comparable stability ratio with the intact condition. Medialization of 4 mm provided acceptable restoration of shoulder stability when a Latarjet procedure was used, but not for a distal clavicular autograft, although neither option restored stability when compared with the intact condition. As such, the Latarjet procedure may be more forgiving to mild medial mispositioning, possibly due to the added effect of the conjoined tendon on shoulder stability.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671251320369 – Supplemental material for Latarjet Coracoid Transfer Versus Distal Clavicular Autograft for Anterior Shoulder Instability With Glenoid Bone Loss: A Biomechanical Comparison of 2 Graft Reconstructions in Various Medial Positions
Supplemental material, sj-pdf-1-ojs-10.1177_23259671251320369 for Latarjet Coracoid Transfer Versus Distal Clavicular Autograft for Anterior Shoulder Instability With Glenoid Bone Loss: A Biomechanical Comparison of 2 Graft Reconstructions in Various Medial Positions by Ibrahim M. Haidar, Jean-David Werthel, Alexander W. Hooke, Joaquin Sanchez-Sotelo and Alexandre Hardy in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted September 17, 2024; accepted September 19, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the French Society of Arthroscopy. J.S.-S. has received consulting fees from Acumed, Exactech, Stryker, and Wright Medical; nonconsulting fees from Acumed, Stryker, and Wright Medical; and royalties from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Mayo Clinic Biospecimens Subcommittee (reference No. 21-001152).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.