
Abstract
Background:
Despite published guidelines describing on-field rehabilitation (OFR) frameworks for soccer, available evidence for practitioners who work with players with anterior cruciate ligament reconstruction (ACLR) is limited.
Purpose:
To document the activity and workloads completed by a large cohort of amateur and professional soccer players during OFR following ACLR after completing their indoor rehabilitation and to establish their return to competition (RTC) outcomes.
Study Design:
Case series; Level of evidence, 4.
Methods:
OFR measurements/activities, global positioning system (GPS), and heart rate data were collected from 100 male 11-a-side soccer players with ACLR undergoing a criteria-based rehabilitation process, concluding with a 5-stage OFR program. Consent was obtained directly from the players involved in this study before completing a follow-up questionnaire to document RTC outcomes. Differences between the level of play (professional and amateur) and 5 OFR stages were investigated using separate linear mixed models.
Results:
A minimum 9-month follow-up was possible for 97 players (97%), with a median time of 2.3 years after ACLR and 84% RTC, with higher rates in professionals (100%) than amateurs (80%). Ten (10%) players sustained an ACL reinjury. Professionals completed more OFR sessions (20.6 ± 7.7 vs 13.2 ± 7.7; P < .001) over a shorter period (44.7 ± 30.3 vs 59.3 ± 28.5 days; P = .044) and achieved higher workloads mostly in the high-intensity GPS metrics in each OFR stage. Typical external workload outputs in the final OFR stage aligned with team training demands for the total distance (TD) (106%), high-intensity distance (HID) (104%), peak speed (PS) (88%), acceleration distance (ACC) (110%), and deceleration distance (DEC) (48%), but they were lower compared with match play demands (TD: 44%; HID: 51%; PS: 82%; ACC: 63%; and DEC: 26%).
Conclusion:
High RTC rates were reported in those players who participated in OFR after indoor rehabilitation. Completion of all five OFR stages almost prepared them for team training demands; however, workloads remain low compared to match play.
Keywords
Anterior cruciate ligament (ACL) rupture and subsequent reconstruction (ACLR) is a detrimental injury, resulting in long lay-off times for both amateur3,31 and professional soccer players.35,50 Virtually all injured players undertake ACLR (99%) to facilitate return to competition (RTC), 50 but only 81% of amateur patients resume some kind of sporting activity, 33 typically in >12 months, 4 with only 55% returning to competitive sports.3,31 In contrast, professional soccer players exhibit higher RTC rates, with nearly all (97%) returning within 12 months.16,50 Young amateur players (<25 years old) returning to high-level competitive sports carry the highest risk of reinjury,34,39,52 ranging from 6% to 29%, with most reinjuries occurring within 2 years from RTC.21,39,51 Professionals are not immune to reinjury, as 18% reinjure the ACL within 4.3 (interquartile range [IQR], 4.6) years after ACLR.16,50
To improve functional outcomes, rehabilitation and RTC processes should be criteria-based2,6,45 and players should transition through rehabilitation stages and across a return-to-sport continuum consisting of on-field rehabilitation (OFR), return-to-team training (RTT), RTC, and return to performance (RTPerf). RTC refers to the participation in competitive matches after the injury, but not necessarily at the same or higher preinjury level of performance. 11 OFR is thought to be the vital bridge between in-clinic medically managed rehabilitation and RTT environment with coaching/performance staff.5,9 Recently, 2 conceptual OFR frameworks for soccer have been published, both involving 5 stages of progressively increasing activity: the 4 pillars framework by Buckthorpe et al 9 and the control to chaos continuum by Taberner et al. 45 While both frameworks appear conceptually sound, they are based on expert opinion9,10,45 and single-case study 46 applications. There is a need to investigate these anecdotal frameworks through experimental evidence 29 and via larger case series. 5
While current frameworks highlight the importance of training load management and sufficient physical fitness preparation to safely RTC,7,9,12,45 there is scarce information regarding the workloads that players accumulate during OFR before medical release for RTC. It is recommended to monitor and manage training loads during the OFR phase to facilitate the successful reintegration of the soccer player into team training, with minimal risk of reinjury.11,45 Technologies capable of recording objective data—such as the global positioning system (GPS)—should be implemented to quantify the physical demands of OFR training sessions when possible.2,5,12,44 Despite published clinical commentaries, 10 it is unclear which GPS metrics are relevant for determining the readiness of players with ACLR to RTC and for supporting practitioners in planning and adjusting workloads during the OFR via a GPS data-informed process. This study aimed to document the OFR activity and workloads completed by a large cohort of soccer players with ACLR during an OFR period, providing data depending on the level of play and comparing OFR activity and RTC between amateur and professional players.
Methods
Inclusion/Exclusion Criteria, Participants, and ACL Rehabilitation Pathway
A total of 100 male 11-a-side soccer players who were undergoing rehabilitation to return to competitive soccer after primary or secondary ACLR between 2018 and 2022 were included in this study (Table 1). Only players attending rehabilitation at the Bologna (Italy) or London (United Kingdom) clinics of the Isokinetic Medical Group (FIFA Medical Centre of Excellence) were included in this study. Additional inclusion criteria were as follows: (1) clearance from the surgeon and sports medicine physician to RTC; and (2) the player’s ambition to return to competitive 11-a-side soccer.
Player Characteristics, Types of ACL Injury, and Grafts Selected for ACL Surgery and OFR Measurements a
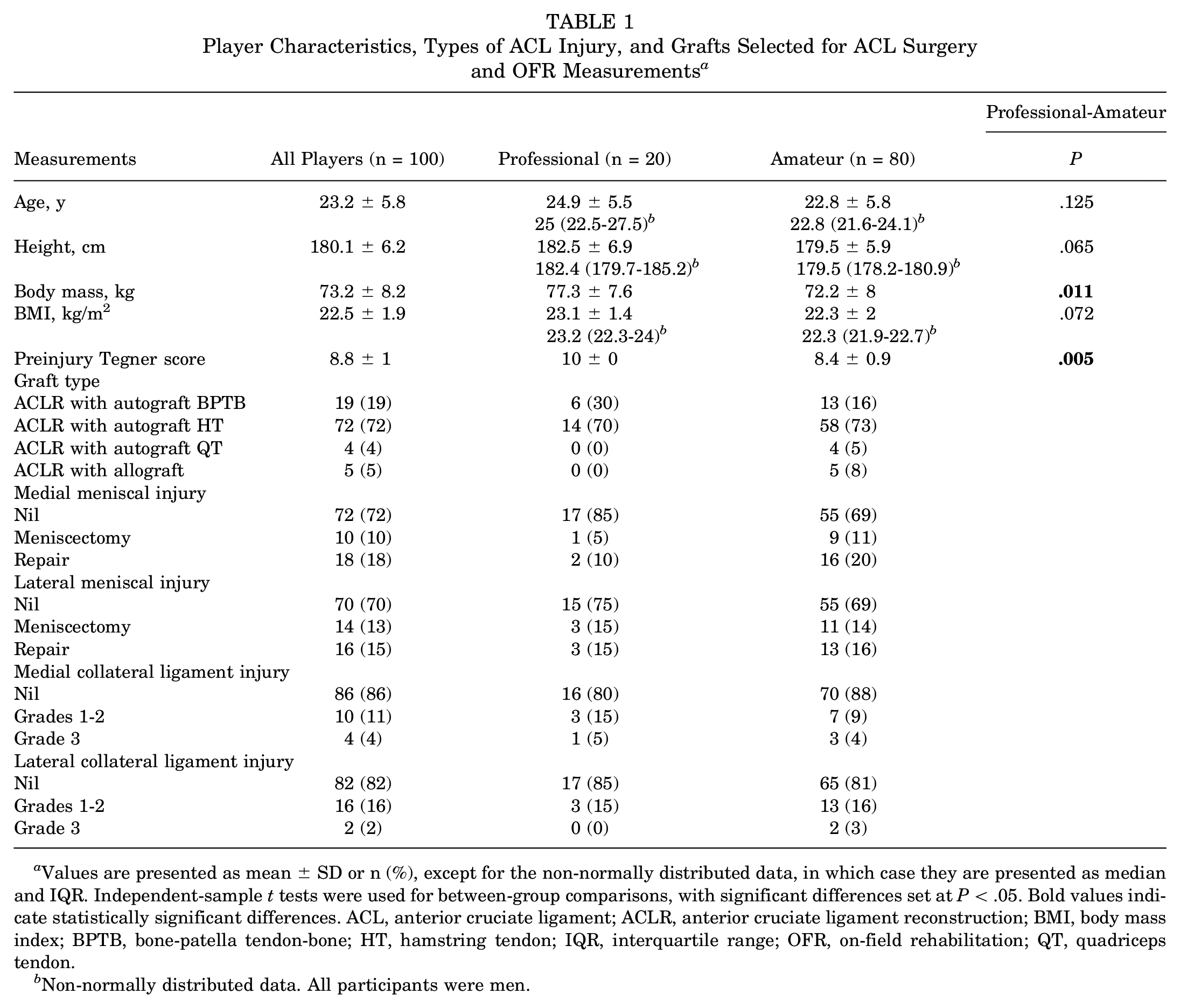
Values are presented as mean ± SD or n (%), except for the non-normally distributed data, in which case they are presented as median and IQR. Independent-sample t tests were used for between-group comparisons, with significant differences set at P < .05. Bold values indicate statistically significant differences. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; BPTB, bone-patella tendon-bone; HT, hamstring tendon; IQR, interquartile range; OFR, on-field rehabilitation; QT, quadriceps tendon.
Non-normally distributed data. All participants were men.
OFR Period
Players were transitioned through a criteria-based rehabilitation process, culminating in a 5-stage OFR program (see Appendix), 10 in which 4 important elements (movement quality, physical conditioning, soccer-specific skills, and training load) of a high-quality OFR approach were implemented. 9 External workloads—defined as “the physical work prescribed in the training plan” 27 —were progressively incremented over the 5 OFR stages via different individual or group soccer and running-type drills while considering an increased complexity of the qualitative aspect of the sessions. The stage-to-stage transition was driven by a continuous comparison between different drills subjected to the player and the way the knee and soft tissues responded to the given loads along with defined stage-specific criteria. 10 The OFR sessions were delivered on a regular 11-a-side outdoor grass soccer pitch (100 × 50–m, grass) supervised by 2 soccer rehabilitation coaches with >5 years of experience in rehabbing professional and amateur soccer players from different types of soccer-related injuries.
Player’s Monitoring
External and internal workloads were monitored via GPS technology (Catapult S5 and S7; Catapult Sports; sampling rate 10 Hz) and accompanying heart rate (HR) monitor (Polar H10), respectively. The GPS brand and unit were considered valid and reliable for research. 8 The GPS unit’s model was upgraded over the years, but the brand and the sampling rate remained consistent. 36 The players wore the same unit for each OFR session in an appropriate tight-fitting vest between their shoulder blades at the thoracic spine level to reduce between-unit measurement errors. 49 The vest’s snug fit ensures accurate data collection by minimizing undesired movements. 30 The HR monitor was secured to the chest via an elastic strap and connected with the GPS unit via Bluetooth to record HR data. Participant’s maximum HR (HRmax) was calculated as the age-predicted maximum using the Tanaka formula 47 and set from the player’s profile on Catapult Openfield software before the beginning of the OFR period. If a player achieved a higher HRmax during the OFR period, the new HRmax was used to monitor future activities. Published recommendations were followed for in-session data collection and for minimizing errors during the process.36,49
Internal and External Workload Measures
The modified Borg CR-10 scale was used to assess the player’s perceived exertion (RPE) rating within 30 minutes from the end of each OFR session. 28 GPS variables measured and analyzed during each session are summarized in Table 2.
GPS and HR Variables Measured and Analyzed Across the Observed OFR Period a
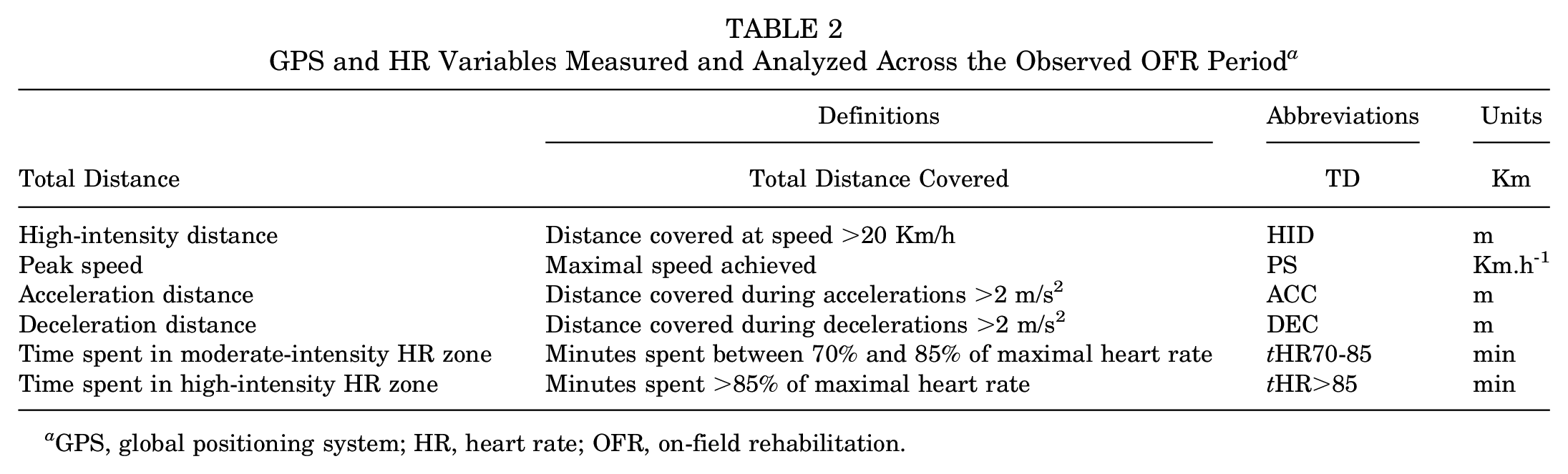
GPS, global positioning system; HR, heart rate; OFR, on-field rehabilitation.
Data Processing
Post-session analyses from Catapult Openfield software included inspection for irregularities of raw traces of velocity from the collected GPS and HR data. Data were filtered using Catapult Openfield software and then exported into a custom-developed anonymized Microsoft Excel sheet Version 16.66.1 (Microsoft), along with players’ characteristics—including age, body mass, height, body mass index (BMI), surgical procedure, level of soccer, Tegner scale, dominant and injured limb, position on the pitch, and injury mechanism. Published recommendations to conduct post-session data analyses were followed.32,49
Follow-up
Follow-ups were conducted over 2 months in 2023 to ascertain RTC outcomes. Players were contacted via email and eventually via telephone to complete a web-based (Jisc Online Surveis Version 2022) and study-specific questionnaire relating to their RTC outcomes. After obtaining their informed consent, the players were directed to the survey questionnaire, which included questions about their RTC outcomes after ACLR, reasons for not returning to soccer, pre- and postinjury levels of soccer, and whether they sustained an ACL reinjury once they resumed soccer.
Statistical Analysis
Descriptive statistics were used to summarize participant’s characteristics (age, weight, height, BMI, and level of soccer), measurements of the OFR period (total number of sessions completed, number of sessions per week, OFR period duration, time to start OFR, number of sessions completed per OFR stage, duration of each session, and duration of each stage), and internal/external workload variables—RPE, total distance (TD), high-intensity distance (HID), maximal speed achieved (PS), acceleration distance (ACC), deceleration distance (DEC), tHR70-85, and tHR >85. Continuous variables were presented as mean (SD) or median (range) as appropriate according to variable distribution. Discrete variables were presented as absolute numbers and percentages on the number of total observations. Data were visually inspected for normality of distribution with quantile-quantile plots. Separate linear mixed models were conducted to evaluate the 21 dependent variables and the fixed effects of the level of play (professional and amateur) and the 5 OFR stages (stages 1-5). Players were entered as random effects for all analyses, as some of them did not participate in every OFR stage. When fixed factors were significant (P < .05), post-hoc (Sidak) comparisons were conducted to determine differences between standards. The chi-square test of independence was performed to examine the relationship between the RTC rate and those players who reached Stage 5 versus the rest of the cohort. The significance level was set as P < .05 for all null hypothesis testing. All statistical analyses were performed using SPSS Statistics Version 28 (IBM Corp).
Results
Follow-up and RTC Outcomes
A minimum follow-up of at least 9 months was possible for 97 players (97%), with a median follow-up time of 2.3 (IQR, 1.9) years after ACLR (see Table 3). The mean times to RTT (6.9 ± 1.9 vs 8 ± 2.1; P < .001) and to RTC (8.8 ± 2.3 vs 9.5 ± 2.4 months; P < .001) were significantly shorter in professionals than amateurs. While all professional players from this study did RTC, 80% of the amateurs returned to competitive soccer. The main reasons for those amateurs who did not RTC were not being psychologically ready (fear of reinjury) (3%, n = 2), not being physically ready (persistent knee issues) (10%, n = 8), and reasons not related to the knee (8%, n = 6). Ten players (10%) sustained a second ACL injury—5 (50%) to the ipsilateral ACL graft and 5 (50%) to the contralateral native ACL, with a significant difference between professionals and amateurs (1 vs 9 second ACL injury; P < .001). The mean time to reinjury after ACLR was 11.5 ± 5.6 months (range, 4.8-26)—ipsilateral ACL graft injuries occurred in 8.1 ± 2 months (range, 4.8-15.5) and contralateral ACL injuries in 14.9 ± 6 months (range, 8.1-26). Players who reached stage 5 of the OFR program (33%) had higher RTC rates compared with the rest of the cohort (90% vs 71%; P = .016).
Follow-up Questionnaire and RTC Outcomes a

Values are expressed as n (%). ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; RTC, return to competition.
Measurements of the 5-stage OFR Period
OFR accounted for 20% and 25% of the overall rehabilitation duration for professional and amateur players, respectively. Players completed, on average, 15 sessions of OFR over 56 days. Professionals completed more OFR sessions (20.6 ± 7.7 vs 13.2 ± 7.7; P < .001) with higher weekly frequency (3.7 ± 1.2 vs 1.7 ± 0.8 days; P < .001) and over a shorter period (44.7 ± 30.3 vs 59.3 ± 28.5 days; P = .044) than amateurs. The number of days to commence OFR after ACLR was similar between professional and amateur players (162 ± 52 vs 190 ± 80; P = .134). The overall rehabilitation duration—including the period of OFR—was shorter for professionals (206 ± 69 vs 249 ± 85 days; P = .038). Descriptive data and fixed effects pairwise comparisons for the level of play and the 5 OFR stages are presented in Tables 4 and 5. No significant difference was observed between professionals and amateurs in the types of ACL injury and surgical procedures (Table 1).
Fixed Effect Pairwise Comparisons for the 5 OFR Stages and Level of Play Among Soccer Players With ACLR Across the Observed GPS and HR Variables a
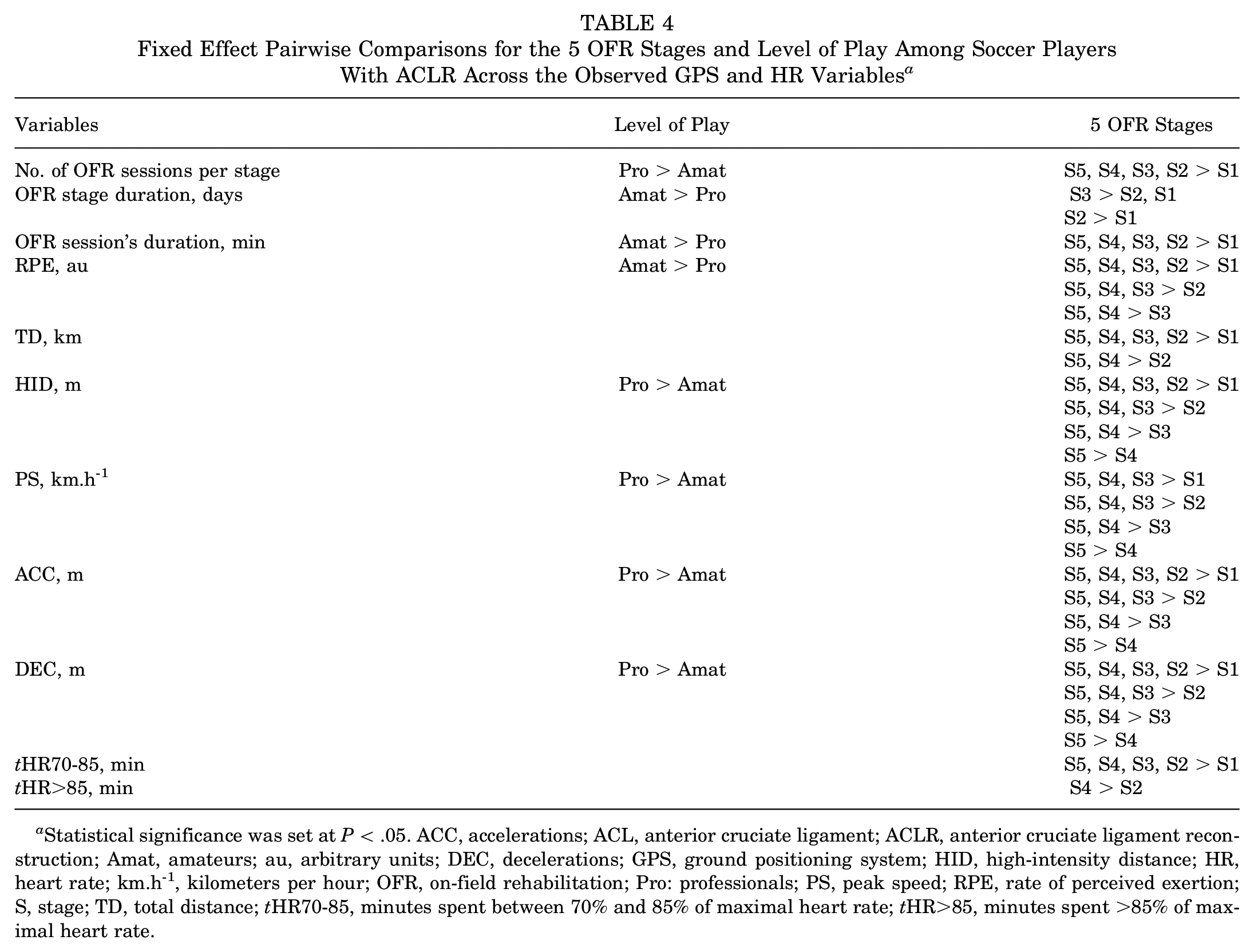
Statistical significance was set at P < .05. ACC, accelerations; ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; Amat, amateurs; au, arbitrary units; DEC, decelerations; GPS, ground positioning system; HID, high-intensity distance; HR, heart rate; km.h-1, kilometers per hour; OFR, on-field rehabilitation; Pro: professionals; PS, peak speed; RPE, rate of perceived exertion; S, stage; TD, total distance; tHR70-85, minutes spent between 70% and 85% of maximal heart rate; tHR>85, minutes spent >85% of maximal heart rate.
Between-Group Comparison of the Observed GPS and HR Variables Across the 5-Stage OFR Period a

For athletes with ACLR, both professional and amateur, data are presented as mean ± SD, except for the number of players in each OFR stage. Statistical significance was set at P < .05. ACC, accelerations; ACL, anterior cruciate ligament; All, all players; Amat, amateurs; DEC, decelerations; GPS, ground positioning system; HID, high-intensity distance; HR, heart rate; km.h-1, kilometers per hour; OFR, on-field rehabilitation; RPE, rate of perceived exertion; Prof, professionals; PS, peak speed; TD, total distance; tHR70-85, minutes spent between 70% and 85% of maximal heart rate; tHR>85, minutes spent above 85% of maximal heart rate.
External and Internal Workload Variables
All workload metrics significantly increased throughout the OFR stages (P < .05), and professional players completed more workload for each GPS variable, except for TD, tHR70-85, and tHR>85 (Tables 4 and 5). TD significantly increased from stage 1 to stage 2 (P < .001) but then plateaued toward stage 5 in both amateurs and professionals. The HID remained significantly higher in professional players at stages 3 (P < .001), 4 (P < .001), and 5 (P < .001), and similar increments across the last 2 stages were noticed in amateurs (30%) and professionals (24%). The PS consistently increased for each OFR stage (P < .001), with professionals achieving significantly higher values than amateurs (P < .001). The ACC and DEC linearly progressed across OFR, but the ACC distance was 2-fold higher than the DEC in each stage. The ACC showed a statistically significant difference between levels of play during most of the OFR stages (P < .05), except for stage 1. On the contrary, professionals completed significantly more DEC than amateurs only in stages 3 and 5 (P < .05). tHR70-85 doubled across the OFR period in both groups; however, increments were significant from stage 1 to stage 2 only (P < .001). The tHR>85 increased only for amateurs, even though changes across stages were nonsignificant.
Discussion
This is the first study to document GPS workloads and session quantity according to stages of OFR activity, with outcome data on a large cohort of ACLR soccer players monitored in a controlled rehabilitation setting. The cohort was comprehensively characterized and followed up (97%), with reports across various domains—including RTC outcomes, measurements of the 5-stage OFR period, external and internal workload variables, and second ACL injury. The results demonstrated higher RTC rates to preinjury levels of soccer for those players, among the 100 players investigated, who reached stage 5 of the OFR program by completing more OFR sessions and cumulating more workloads across the investigated GPS variables after a criteria-based rehabilitation process.
RTC Outcomes
Our cohort’s RTC rates at the same preinjury level for amateurs are notably high compared with the published literature 3 (80% vs 55%-65%), with professionals also showing excellent outcomes, which is in line with the published data by the Union of European Football Associations. 50 Collectively, we report similar outcomes to King et al 33 who documented an 81% RTC rate after primary ACLR in competitive level 1 athletes. Superior outcomes for professionals versus amateurs are likely a function of early diagnostics, referral to experienced surgeons, daily expert-led rehabilitation, and large financial motivation for the player to RTC.23,24,50 Improved amateur’s RTC outcomes in our study versus published literature 2 might relate to rehabilitation factors, as those players (26%) who reached stage 5 of the OFR program, completing more sessions and workloads, reported higher RTC rates (86%) compared with the rest of the cohort. However, it remains unclear whether increased OFR workloads enhanced physical and psychological readiness for RTC or whether it was the level of play or the number of OFR sessions that determined higher RTC rates.
OFR Activity
The OFR duration for the overall rehabilitation process was aligned with previous research from our group, 17 both for professional and amateur players. Most players (43%) did not reach stage 5 and stopped at earlier stages and thus did not complete the full OFR process. Buckthorpe et al 10 suggest that the stage 5 activity of their OFR framework reflects training simulation and can be performed in a controlled environment (eg, OFR) or as part of modified training with the team. Professionals tended to perform more OFR and progress to later stages, which could have contributed to superior outcomes, among other factors.23,50
Workload Across the 5-Stage OFR Period Versus Soccer Training and Match Demands
Most GPS variables were logically progressed across the 5 OFR stages, aligned with a published clinical commentary. 10 Differences across metrics were observed in terms of progression and based on suggested values (see Appendix), literature-reported training,29,41,42,48 and match demands.22,26,40,42,48
The plateau in TD suggests that it is not a useful metric for RTC decision-making or for progressing through OFR. Training TD varies depending on the day of the microcycle, the player’s position and status, the phase of the soccer season, and the league. 42 In our study, TD in stages 3 to 5 was similar to the reported team training demands (range, 3.1-6.5 km), even though values achieved in stage 5 remained suboptimal with respect to match demands in professional40,42,48 and amateur 38 players (44% of match play). Conversely, the HID continued to increase across OFR stages, and values completed by our cohort of professionals and amateurs in stages 4 and 5 were in line with weekly training loads (range, 109-338 m).20,22,42,48 However, only 51% was restored regarding match demands, in both noninjured professional20,22,42,48 and amateur 38 players, suggesting that a further period of progressive accumulation of the HID is needed for both groups before RTC.
Professional soccer players typically reach match PS values 14 between 31 and 34 km.h-1. During the fifth stage of OFR, recorded PS values were lower than match play 19 and midweek team training speeds19,20 reported in elite players, 48 as well as below recommendations from Buckthorpe et al 10 at stages 4 and 5 of OFR (>30 km.h-1), suggesting that players may have achieved <90% of their PS during OFR. The lack of preinjury PS data in most cases led to reporting only absolute values.
Intense horizontal decelerations—typically performed during pressing, tackling, or other situational patterns—are among the most common inciting events preceding noncontact and indirect contact ACL injuries in soccer. 15 Thus, the ability to decelerate is essential for players and a potential vaccine against ACL injuries. 37 In soccer training, low ACC and DEC intensities occur more frequently than higher intensities, 26 with little differences in the number of events performed and meters covered, 41 but the high-intensity DEC distance is normally 3 times greater than the acceleration distance during matches. 26 When compared with the reported training41,48 and match play DEC data,26,42,48 the DEC distance was markedly shorter than the ACC distance in our study (ACC: 110% of training and 63% of match play; DEC: 48% of training and 26% of match play), indicating that players are underprepared for the DEC demands of soccer after OFR. Although the precise reason for this is not clear, it could be due to the OFR program design and length or the decreased capacity of players with ACLR to execute high-intensity braking activities on the pitch. Deceleration ability is partly linked to quadriceps strength, 37 suggesting that lower DEC workloads could affect RTC and reinjury risk, considering the ACL injury mechanism. 15 Further research to understand the impact of this reduced DEC workload on RTC outcomes with a larger sample size is needed.
Consistent with existing research, 18 our work showed that the level of play does not affect physiological responses. Indeed, our cohort of amateurs spent similar time in moderate and high-intensity HR zones than professionals across the 5 OFR stages. tHR70-85 and tHR>85 at stage 5 were less than typical training microcycles42,43,48 and match play demands40,48 in professional players. Because of the absence of pitch-based cardiovascular (CV) testing before RTT and then RTC, it remains unclear whether the investigated cohort was exposed to sufficient CV conditioning during the OFR period. Considering the reduced maximal aerobic capacity observed in soccer players with ACLR 6 months after surgery, 1 further research is necessary to fully understand the CV adaptations from this training modality and the adequate amount of training required to restore the player’s CV profile before resuming competitive soccer. 17
Clinical Implications, Methodological Considerations, and Areas for Future Research
Despite OFR being an optimal rehabilitation environment to transition soccer players with ACLR from gym-based rehabilitation to the soccer team, this study showed that OFR facilitates RTT preparation but does not fully prepare the players for the workload demands of full team training. Only some metrics were restored with respect to team training, highlighting the need for further training (eg, modified training) before full integration with the team training practices and before RTC. Future studies involving more statistically powered cohorts of players will be essential to investigate the optimal number of OFR sessions and workloads per level of play before clearing players with ACLR to RTT and then to the competition, with a lower risk of reinjury.
Limitations
A major limitation of our study is the absence of information on post-OFR training activities, as we could not monitor players once back with the team, leaving us uncertain about the volume and intensity of training completed upon RTT and RTC. Because of the lack of preinjury GPS data in most players, we compared our OFR workload data with the available literature on soccer training and match demands. However, further research should examine the workload throughout the return to sport continuum. 11
In this study, the 5-stage OFR program by Buckthorpe et al 10 was utilized to advance players through stages in a clinical rehabilitation setting. Given the existence of alternative OFR frameworks for soccer, 45 players with ACLR may progress differently for RTT and RTC in a club environment, depending on the team’s adoption of published OFR frameworks or utilization of individual team frameworks. Future research is essential to explore OFR frameworks in club settings and assess the GPS workloads of ACLR players managed by club-based practitioners.
The substantial dataset, which comprises a homogeneous group of professional and amateur 11-a-side male soccer players, represented the main strength of this study. Given the different training 13 and match demands22,25 of women’s soccer, our findings are most likely not applicable to female players returning to soccer after ACLR, highlighting that more research in this field is required.
Clearance from the surgeon, along with the sports medicine physician, was a relevant entry criterion for this study. Because different surgeons operated on the players involved in this study, we did not have surgeon-specific RTC criteria. Future studies should consider specific criteria from surgeons to RTC.
Conclusion
High RTC rates were reported in those ACLR players who participated in a period of OFR after indoor rehabilitation. Completion of all five OFR stages almost prepared them for team training demands; however, workloads remain low compared to match play.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671251320093 – Supplemental material for High Return to Competition Rate After On-Field Rehabilitation in Competitive Male Soccer Players After ACL Reconstruction: GPS Tracking in 100 Consecutive Cases
Supplemental material, sj-pdf-1-ojs-10.1177_23259671251320093 for High Return to Competition Rate After On-Field Rehabilitation in Competitive Male Soccer Players After ACL Reconstruction: GPS Tracking in 100 Consecutive Cases by Filippo Picinini, Francesco Della Villa, Jamie Tallent, Stephen David Patterson, Lorenzo Galassi, Matteo Parigino, Giovanni La Rosa, Gianni Nanni, Jesus Olmo, Matthew Stride, Fabrizio Aggio and Matthew Buckthorpe in The Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank Elena Stanzani for her valuable support in contacting some of the football players based in Italy for follow-ups.
Final revision submitted August 29, 2024; accepted September 26, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This is the first study of a part-time and fully funded PhD program conducted by F.P. (first author) at Isokinetic Medical Group. F.P. collected data as part of his daily clinical responsibilities at Isokinetic Medical Group. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethical committee of St Mary’s University Twickenham (London).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.