
Abstract
Background:
Whether periacetabular osteotomy (PAO) improves hip microinstability in patients with symptomatic hip dysplasia remains poorly understood.
Purpose:
To assess the femoral head translation with static postural change, considered a potential indicator of hip microinstability, comparing dysplastic hips before and after PAO with normal hips.
Study Design:
Descriptive laboratory study.
Methods:
A total of 26 patients (30 hips) with hip dysplasia underwent PAO, and 18 healthy individuals (18 hips) were eligible. Using a 3-dimensional–to–2-dimensional registration technique, femoral head translation before and after PAO was quantified as the displacement of the center of the femoral head relative to the center of the acetabulum between supine and standing positions. Morphological factors on supine anteroposterior pelvic radiographs before and after PAO correlated with the femoral head translation, particularly lateral translation, were examined.
Results:
Femoral head translation decreased after PAO (1.5 ± 0.4 mm vs 1.0 ± 0.4 mm; P < .001) but remained larger than in controls (1.0 ± 0.4 mm vs 0.7 ± 0.3 mm; P = .01). The more severe the hip dysplasia before PAO was, the greater the femoral head translation. However, the femoral head translation improved after PAO with sufficient acetabular correction. The acetabular roof obliquity (ARO) showed the strongest correlation with lateral translation of the femoral head from the supine to standing position before PAO. In contrast, no correlation was found after PAO.
Conclusion:
This study demonstrates that the severity of hip dysplasia influences hip microinstability, that PAO mitigates hip microinstability with adequate acetabular correction, and that PAO does not normalize hip stability because of residual joint incongruity. In patients with a larger ARO, the femoral head has more lateral translation in the standing position. Therefore, weightbearing postural radiographs are crucial for understanding hip biomechanics in hip dysplasia and refining surgical corrections during PAO.
Clinical Relevance:
PAO can make the hip more stable in hip dysplasia, but not as stable as the normal hip. In hip dysplasia, pre-PAO standing radiographs should be evaluated due to their accurately representing the femoral head position relative to the acetabulum.
Keywords
The hip is generally considered inherently stable, but the femoral head does move in relation to the acetabulum.4,33 While the congruent bony architecture of the hip is important to its stability, recent studies have shown that the surrounding soft tissues involving the acetabular labrum, ligamentum teres, and capsular structures are also important.3,9,36,38 Patients with hip dysplasia have not only insufficient coverage of the femoral head but also an incongruent joint, which can cause a larger discrepancy in the distance between the acetabular center and the femoral head center.7,15,27,28 Furthermore, many of these patients have features of generalized joint laxity.2,47 These patients may also experience injuries from trauma, sports injuries, or joint insults in daily life that cause bony deficiency or soft tissue damage. This can lead to abnormal hip motion with pain, which is defined as symptomatic microinstability.16,33 The morphological features to diagnose hip microinstability in patients with hip dysplasia have been discussed in many studies, but the best way to assess hip microinstability remains unclear.30,32,44,45
The periacetabular osteotomy (PAO) is a versatile procedure that enables reorientation of the acetabulum along all 3 dimensions in patients with hip dysplasia. PAO can increase the acetabular coverage of the femoral head, increase the contact area, and decrease joint contact pressures.8,19 PAO has also been proven to reduce or eliminate subjective hip instability symptoms according to subjective and objective assessments involving patient-reported outcome measures and clinical examinations, and consequently improve the natural course of the hip.5,25,29,46 However, no data are available on the extent of improvement in joint microinstability after PAO, while data are available on joint microinstability in static and dynamic situations before PAO.34,35
Previous studies have suggested that radiographs obtained in the supine position may not provide the functional position of the femur relative to the acetabulum, and that weightbearing radiographs are potentially more informative to evaluate hip deformity.31,39,42 The abnormal mechanical environment in dysplastic hips, including increased joint contact pressure and overloading of the anterosuperior acetabulum, presents a potential issue when the individual hip is in a weightbearing position rather than in a supine position. A recent study has shown that during transition from the supine to the standing position, the femoral head shifts slightly laterally relative to the acetabulum. 34 This lateral shift will result in reduced acetabular coverage of the femoral head, for example, reduced lateral center-edge angle (LCEA), decreased joint contact area, and increased joint contact pressures.18,39 As a result, patients with a femoral head moving laterally in the standing position may exacerbate early osteoarthritis (OA) progression. Therefore, determining the morphological characteristics associated with lateral translation of the femoral head in the standing position is invaluable for surgeons to understand the underlying mechanisms by which PAO improves hip biomechanics and to refine the surgical correction during PAO.
In this study, we measured 3-dimensional (3D) femoral head translations from supine to standing postures, considered a potential indicator of hip microinstability, and compared joint kinematics between dysplastic hips before and after PAO with normal hips. Using 3D-to–2-dimensional (2D) model-to-image registration, we sought to determine the following: (1) the location of the femoral head center relative to the acetabular center, (2) the femoral head translation from supine to standing postures, and (3) the hip morphological factors related to the observed translations.
Methods
Participants
This study was approved by our institution’s internal review board, and patient consent was obtained. A retrospective cohort study of patients with hip dysplasia was conducted using prospectively collected data from our institution's PAO database, performed by expert hip surgeons (Y.N., S.H., and M.F.) from August 2012 to January 2019. The medical records of a consecutive cohort of 68 patients (76 hips) with frank and borderline hip dysplasia (LCEA <25°) were reviewed.12,49 No patients were simultaneously treated for intra-articular lesions at the time of PAO. They underwent supine and standing anteroposterior (AP) pelvic radiography and pelvic computed tomography (CT) before and after PAO. Exclusion criteria were (1) insufficient image records, (2) previous surgery of the analyzed hip, (3) previous spinal surgery, (4) osteoarthritic change in either joint, and (5) neuromuscular disorders. Among patients with hip dysplasia, 41 patients (45 hips) and 1 patient (1 hip) were excluded due to insufficient image records and advanced OA based on the exclusion criteria, respectively (Figure 1A). In total, 26 patients (1 male and 25 female) had a mean age of 35.9 ± 13.0 years, and their general information is shown in Table 1. Eight patients with bilateral hip dysplasia who had previously undergone PAO on the contralateral hip were included.

Flowcharts of (A) patient selection and (B) normal volunteer selection.
Demographic Data in Hip Dysplasia and Control Groups a

Values are presented as mean ± SD or n (%).
For the control group, the records of 42 healthy volunteers collected in previous studies were reviewed after they were confirmed as having no history of disease or articular symptoms in their hips by medical interviews.13,20 They underwent imaging examinations (supine and standing AP pelvic radiography and CT). Among the control group, 13 individuals without sufficient image records and 11 individuals whose LCEA was outside the normal range (25° < LCEA < 40°) in either hip were excluded (Figure 1B). Thus, 18 individuals (2 male and 16 female) were included in the control group (Table 1).
Three-dimensional Model Reconstruction
CT was performed on all participants using standard protocols (Aquilion; Toshiba).11,49 Medical imaging software (Mimics Version 18.0;) was used for segmentation of the entire pelvis and femur from digital images (Digital Imaging and Communications in Medicine format). The resulting 3D bone surface models were smoothed with wrapping functions, applying a gap closure distance and a minimum defect size of 0.2 mm to eliminate surface roughness. This process resulted in largely preserved native anatomic shapes (Figure 2A). 14 These bone models were then aligned to a standardized coordinate system using the anterior pelvic plane (APP) (3-matic software; Materialise).13,49 The origin of the pelvic models was determined as the center of a best-fit sphere to the acetabular lunate surface. The x-axis of the pelvis was defined as a line passing through the origin and parallel to the line connecting the bilateral anterior superior iliac spines. 10 The y-axis was defined as a line on the APP passing through the origin and perpendicular to the x-axis, and the z-axis was defined as a line passing through the origin and perpendicular to the APP (Figure 2B). The femoral position was standardized by aligning the coordinate system of the International Society of Biomechanics recommendation, and the origin was determined as the center of a best-fit sphere to the femoral head.13,49 The positive directions for x, y, and z axes were defined as medial to lateral, inferior to superior, and posterior to anterior, respectively. The radii of the best-fit spheres for the acetabulum and femoral head were calculated.

(A) Representative surface model of the pelvis and femur in a patient with hip dysplasia. (B) Representative surface model with coordinate system applied. The coordinate system of the pelvis model was standardized according to the anterior pelvic plane, and the origin was determined as the center of a sphere that best fits the acetabular lunate surface. The coordinate system of the femoral model was standardized according to the coordinate system described by the International Society of Biomechanics, and the origin was determined as the center of a sphere that best fits the femoral head surface.
Radiographic Evaluation
Supine and standing AP pelvic 2D images were obtained in all participants. Supine 2D images were obtained from radiographs in all participants(30 dysplastic hips and 18 control hips), while standing 2D images were from radiographs in 6 dysplastic hips and all controls (18 hips) and from flat-panel x-ray detectors (Ultimax-I; Toshiba) in 24 dysplastic hips. The flat panel x-ray detector was set on an image area of 420 mm (height) × 420 mm (volume) and 0.274 mm × 0.274 mm/pixel resolution preoperatively and postoperatively. In both supine and standing 2D images, the rotation of the lower limbs was standardized by positioning both patellae in the exact front. The following morphological parameters were measured from supine AP pelvic radiographs before and after PAO: LCEA, acetabular roof obliquity (ARO), Sharp angle, extrusion index, anterior and posterior wall indexes, femoroepiphyseal acetabular roof (FEAR) index, Shenton line, and upsloping lateral sourcil.32,37,40,43,45
Kinematic Analysis
We used open-source software (JointTrack; www.sourceforge.net/projects/jointtrack) to assess the kinematics of the hip joint by performing a 3D-to-2D model-to-image registration (Figure 3).1,10,17,35 In summary, this process entailed overlaying graphically projected bone models onto the radiographic images and manipulating them within a virtual 3D environment until their projections corresponded to the appearance of the patients’ anatomy. The bone model outline was iteratively adjusted to match the radiographic projection, and subsequently registration was fine-tuned using global or local numeric optimization techniques. Notably, the measurement software generated a 3D representation of the pelvic and femoral bones, offering the operator contextual information to facilitate the avoidance of apparent bone overlap. The calculated translations were expressed as the movement of the femur relative to the pelvis, with reference to APP. Specifically, femoral head translation was quantified as the displacement of the center of the femoral head relative to the center of the acetabulum in each image. This technique for hip analysis demonstrated precision levels of 0.2 mm in coronal plane translation, 0.5 mm in AP translation, and 1.6° for rotational measurements,10,35 showing no difference in high accuracy between continuous and simple images.17,21
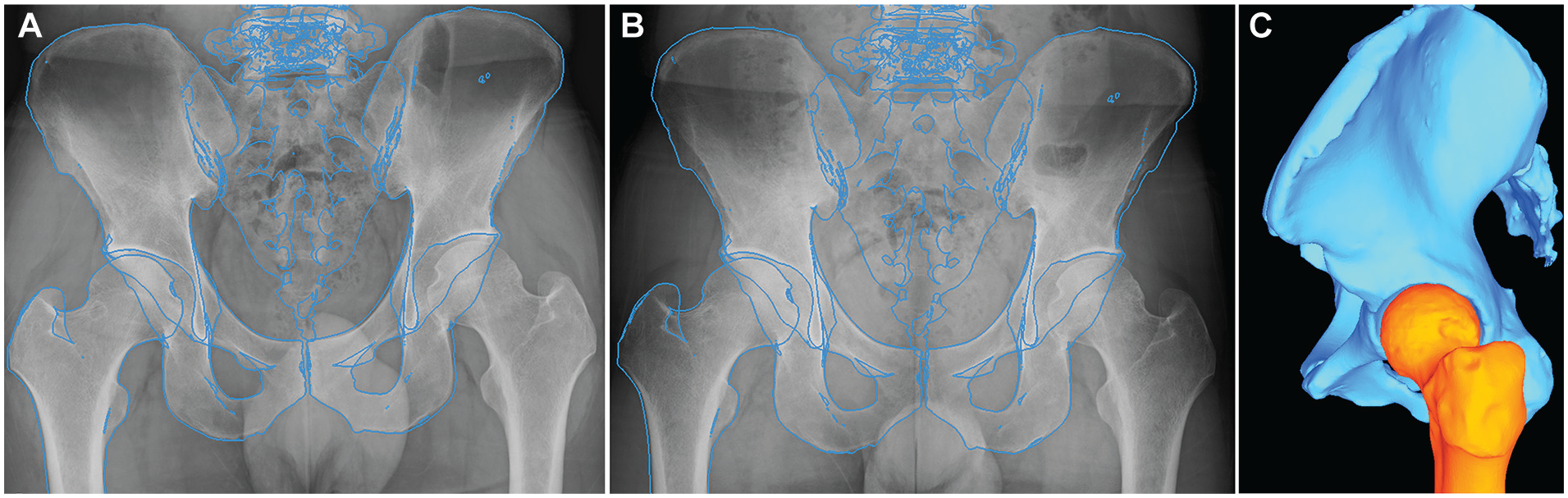
The surface models of the pelvis and femur are superimposed with radiographic images, using the 3-dimensional–to–2-dimensional model-to-image registration technique. The edge of the 3-dimensional models is image-matched to the (A) supine and (B) standing pelvic radiographs while observing (C) a user-adjustable view providing any aspect and zoom of the current joint configuration.
Statistical Analysis
Throughout the statistical analysis, we used parametric or nonparametric tests based on normality (Shapiro-Wilk test) and homoscedasticity (f test). Regarding the demographic data, the Fisher exact test was used to compare categorical parameters between dysplastic and control hips, while the Student t test or Wilcoxon rank-sum test was used to compare continuous parameters. Concerning the morphological parameters, the Dunnett or Steel test with the normal hip as a control was used to compare dysplastic hips before and after PAO with the normal hip. Regarding the location of the femoral head center relative to the acetabular center and the femoral head translation, the paired t test or Wilcoxon signed-rank test with a Bonferroni correction was used to compare continuous parameters before and after PAO, whereas the Student t test or Wilcoxon rank-sum test with a Bonferroni correction was used to compare dysplastic hips before and after PAO with the normal hip. The correlation between 2 continuous parameters was evaluated using the Pearson or Spearman correlation coefficient. Statistical significance was set at P < .05. Statistical analyses were performed using JMP Version 16.0 (SAS Institute).
Results
PAO normalized ARO and FEAR index in patients with hip dysplasia compared with the controls. However, LCEA and posterior wall index were greater than those in the controls, whereas ARO, Sharp angle, extrusion index, and anterior wall index were smaller than those in the controls (Table 2).
Comparison of Radiographic Parameters in Supine Position Between Hip Dysplasia Before and After PAO and Controls a

Values are presented as mean ± SD, median (range), or n (%). PAO, periacetabular osteotomy.
Before PAO versus control.
After PAO versus control.
Femoral Head Center Relative to Acetabular Center
In the supine position, the distance of the femoral head center relative to the acetabular center in hip dysplasia did not change before and after PAO (2.1 mm [range, 0.3-5.6 mm] vs 2.4 mm [range, 1.0-4.9 mm]; P = .78). The distance in controls was smaller than that in dysplastic hips before and after PAO (control vs before PAO: 1.0 mm [range, 0.2-1.5 mm] vs 2.1 mm [range, 0.3-5.6 mm], P < .001; control vs after PAO: 1.0 mm [range, 0.2-1.5 mm] vs 2.4 mm [range, 1.0-4.9 mm], P < .001) (Figure 4A).

The box plots of the distance of the femoral head center relative to the acetabular center between patients with hip dysplasia before and after periacetabular osteotomy (PAO) and controls in the (A) supine and (B) standing positions. *P < .05 for hip dysplasia before PAO versus control; *P < .05 for hip dysplasia after PAO versus control.
Similar to the supine position, in the standing position, the distance of the femoral head center relative to the acetabular center in hip dysplasia did not change before and after PAO (2.2 mm [range, 0.6-6.7 mm] vs 2.4 mm [range, 0.9-4.5 mm]; P > .99). The distance in controls was smaller than in dysplastic hips before and after PAO (control vs before PAO: 0.8 mm [range, 0.1-1.3 mm] vs 2.2 mm [range, 0.6-6.7 mm], P < .001; control vs after PAO: 0.8 mm [range, 0.1-1.3 mm] vs 2.4 mm [range, 0.9-4.5 mm], P < .001) (Figure 4B).
Femoral Head Translation
In patients with hip dysplasia, the femoral head translation from the supine to the standing posture was larger before PAO than after PAO (1.5 ± 0.4 mm vs 1.0 ± 0.4 mm; P < .001), but larger after PAO than that in controls (1.0 ± 0.4 mm vs 0.7 ± 0.3 mm; P = .01) (Table 3). The mediolateral (x) component of the translation in the postural change was not different between dysplastic hips and controls (before PAO vs control: –0.1 ± 0.8 mm vs 0 ± 0.4 mm, P > .99; after PAO vs control: –0.1 ± 0.4 mm vs 0 ± 0.4 mm, P > .99). Before PAO, 23.3% (7/30) of the femoral heads translated laterally from the supine to standing postures, whereas 76.7% (23/30) of the femoral heads translated medially. The superoinferior (y) translation component in the postural change was more superiorly before PAO than in controls (0.5 ± 0.5 mm vs 0.1 ± 0.4 mm; P = .02), but no longer significant after PAO (0.2 ± 0.4 mm vs 0.1 ± 0.4 mm; P = .65), and the anteroposterior (z) translation component in the postural change was more anteriorly before PAO than after PAO (1.0 ± 0.4 mm vs 0.7 ± 0.5 mm; P < .001), and more anteriorly after PAO than that in controls (0.7 ± 0.5 mm vs 0.2 ± 0.4 mm; P = .002) (Table 3, Figure 5).
Distance of the Femoral Head Translation From the Supine to Standing Position Between Hip Dysplasia Before and After PAO and Controls a
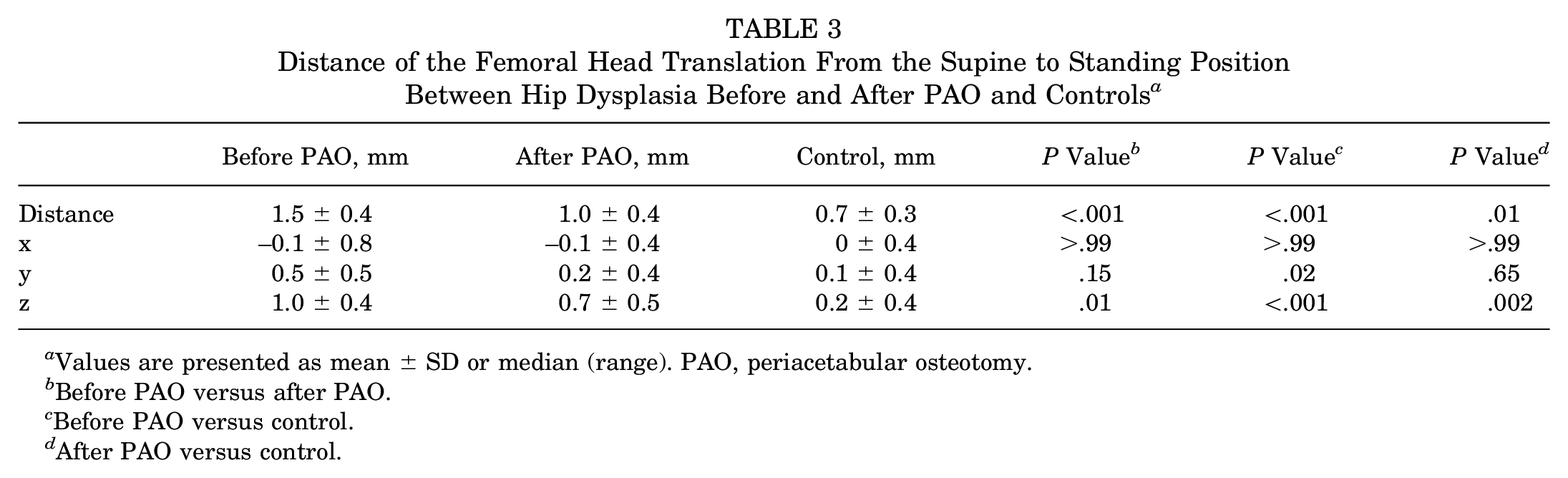
Values are presented as mean ± SD or median (range). PAO, periacetabular osteotomy.
Before PAO versus after PAO.
Before PAO versus control.
After PAO versus control.
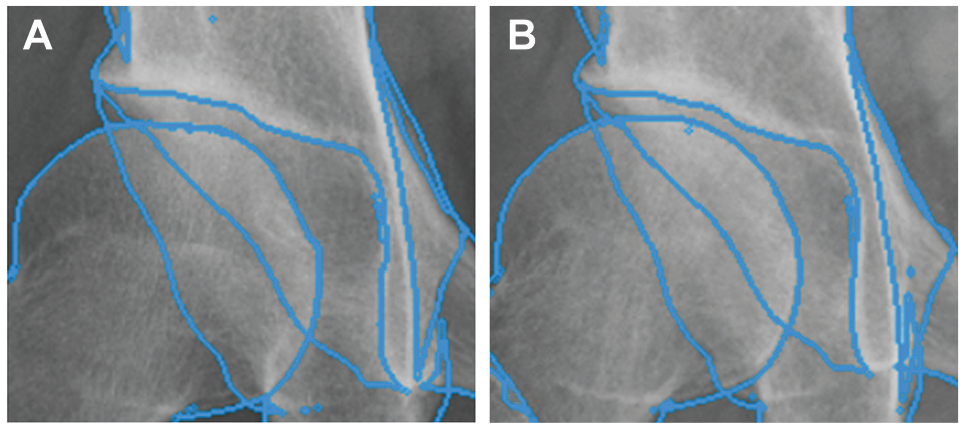
Close-up images of the hip with 3-dimensional–to–2-dimensional model-to-image registration on the (A) supine and (B) standing radiographs in a representative case of hip dysplasia before periacetabular osteotomy. The femoral head translates medially, superiorly, and anteriorly quite slightly in the transition from the supine to standing position, which may not be perceived by the unaided human eye.
Morphological Factors Related to Hip Translations
Before PAO, the femoral head translation was negatively correlated with the LCEA and positively correlated with the ARO, Sharp angle, extrusion index, and difference in radius of the best-fit sphere for the acetabulum and femoral head (Table 4). The mediolateral (x) translation component was most strongly correlated with ARO (Table 5). After PAO, femoral head translation was negatively correlated with the LCEA and positively correlated with the ARO, FEAR index, and difference in radius of the best-fit sphere for the acetabulum and femoral head (Table 4). In the controls, the femoral head translation was not correlated with morphological parameters (Table 4).
Correlations Between the Femoral Head Translation From the Supine to Standing Position and Parameters of Hip Dysplasia Before and After PAO and Controls a

PAO, periacetabular osteotomy.
Pearson or Spearman correlation coefficients.
Correlations Between the Mediolateral (x) Component of the Femoral Head Movement From the Supine to Upright Position and Parameters of Hip Dysplasia Before and After PAO and Controls a

PAO, periacetabular osteotomy.
Pearson or Spearman correlation coefficients.
Discussion
To date, there are no reports assessing hip microinstability before and after PAO in patients with hip dysplasia. In this study, we quantified hip microinstability in static changes between the supine and standing positions before and after PAO in patients with dysplastic hips in comparison with normal hips. We found that femoral head translation after PAO in dysplastic hips decreased but remained larger than in normal hips. The more severe the hip dysplasia before PAO was, the greater the femoral head translation. However, the femoral head translation improved after PAO with sufficient acetabular correction. Overall, femoral heads tended to translate quite slightly medially, superiorly, and anteriorly both before and after PAO in transition from the supine to standing position, showing no difference in the longitudinal and transverse directions between before and after PAO. In contrast, anterior translation was significantly less after PAO than before PAO. The ARO showed the strongest correlation with lateral translation of the femoral head from the supine to standing position before PAO. In contrast, no correlation was found after PAO.
Joint congruency is an essential prognostic predictor when performing PAO.22,27 The 3D curvature mismatch between the acetabulum and femoral head in patients with hip dysplasia is known to be greater than that of participants with normal hips. 15 Similar to previous reports, the current study demonstrated that the difference in the distance between the acetabular and femoral head centers in hip dysplasia before PAO was larger than that in the normal hip, regardless of the posture. In addition, we have revealed for the first time that the difference in distances remained unchanged even after PAO. This might be a predictable outcome because the articular surfaces of the acetabulum and femoral head did not change after PAO. A previous study demonstrated that the 2D difference in the distance between the acetabular and femoral head centers was an independent risk factor for OA progression. 27 Just as 2D differences were associated with OA progression, further studies are needed to determine if 3D differences found in this study are also predictive of OA progression.
The hip can exhibit microinstability if the ball-and-socket joint are not congruent, which is called “play.” If the curvature mismatch ratio and the center discrepancy distance between the acetabulum and femoral head are large, there is potential play in the joint, leading to a less constrained, unstable joint. 15 Sato et al 35 have shown that maximum dynamic translation of the femoral head, particularly superoinferior translation, during the gait cycle was greater before PAO in dysplastic hips than that in normal hips, and the superoinferior translation, like their report, was observed for the static postural changes in this study. Sakai et al 34 described a 1.5-mm translation of the femoral head between the supine and standing positions in patients with hip dysplasia, similar to observations in the current study. Thus, our results have demonstrated small translations of the femoral head via static postural changes in symptomatic hip dysplasia, cannot be perceived by the unaided human eye, and may be a potential indicator of hip microinstability.
In this study, 76.7% (23/30) of the dysplastic hips had a medial translation of the femoral heads when changing from the supine to standing position; consequently, femoral medial translations can lead to increasing acetabular coverage of the femoral head and contact area and decreasing joint contact pressure. Combined with the superior translation shown above, this means that the femoral heads of those patients translated superomedially from the supine to standing position. It was assumed that the translation was due to the joint forces exerted by the load in the standing position from the ligamentous and soft tissue laxity in the supine position. On the other hand, the remaining 23.3% (7/30) of the dysplastic hips had a lateral translation of the femoral heads when changing from the supine to standing position. We also found that dysplastic hips with lateralized translations in the standing posture were well predicted by a larger ARO. Sakai et al 34 found that dysplastic femoral heads translated laterally by a mean of 0.3 mm in the standing position, and the mean ARO of those hips was 25.2°. Femoral lateral translations lead to decreasing acetabular coverage of the femoral head and increasing joint contact pressure, which can consequently exacerbate OA progression. 18 Therefore, the results of this study support previously reported findings that the weightbearing position is more suitable for evaluating hip deformity and planning PAO because the accurate functional orientation of the femur in relation to the acetabulum can be determined.31,39,42 Pullen et al 31 noted that lateral coverage in the standing position is smaller than that in the supine position, which depends on the change in sagittal pelvic tilt, mostly posterior pelvic tilt. Based on the results of this study, this may depend on the lateral translation of the femoral head as well. Thus, preoperative radiographic evaluation in the standing position is needed in patients with hip dysplasia, particularly those with a larger ARO.
In this study, we found that more severe preoperative hip dysplasia increased femoral head translation and that adequate postoperative correction reduced femoral head translation. With regard to the actual correction via PAO, all morphological parameters except for anterior coverage were equivalent or overcorrected compared with the normal hip. Despite the almost normalized morphology, PAO improved femoral head translation in the static postural changes but did not lead to normalization. It is possible that the residual play of the femoral head due to joint incongruity has an adverse effect, supported by the fact that the discrepancy between the acetabular center and the femoral head center in the present study remained unchanged even after PAO. Consequently, it may have influenced the results of the longest 30-year follow-up study to date, in which the joint preservation rate was 29%. 22 However, this study reaffirmed the importance of adequate acetabular correction during PAO to improve joint microinstability. Given the fact that the patients who are eligible for PAO are highly active young people who engage in sports and other activities, new innovations need to be considered in the future to make PAO a better surgery that preserves the hip for a lifetime, rather than making it a surgery for prolonging the hip's degenerative course.
Limitations
There are several study limitations that must be discussed. First, we could not evaluate the relationship between hip microinstability before and after PAO and intra-articular lesions like a labral tear because we did not concomitantly try to perform arthroscopy and repair those lesions at the time of PAO. Intra-articular lesions have been shown to affect hip microinstability before PAO,3,9,36,38 whereas it is unclear whether those lesions affect hip microinstability after PAO. Previous studies have shown that the presence of a labral tear was not predictive of OA progression or conversion to THA after PAO, and good clinical results are obtained in most patients without addressing the labral tear.6,24,26 Therefore, we believe that the acetabular correction via PAO reduces the mechanical overload on the labrum and is expected to improve hip microinstability, and no simultaneous labral repair is required at the time of PAO. However, further study is needed to clarify the relationship between hip microinstability before and after PAO and intra-articular lesions. Second, we did not include measurements in the standing position because there was concern that some 2D standing images acquired from fluoroscopic images did not have pelvic rotation aligned with the front, which could lead to significant measurement errors. 23 Further studies should include parameters measured in the standing position, given that the location of the femoral head center may affect the measurements. Third, the sample size was relatively small. Fourth, we evaluated femoral head translation only in the static postural change. Patients with hip dysplasia often develop pain during dynamic activities, including activities of daily living and sport, and instability can be problematic. Capturing this requires dynamic in vivo analysis to determine activity-dependent kinematics, although this remains technically challenging. However, static postural change between supine and standing postures does indicate hip microinstability, providing a useful surrogate for dynamic activity-specific measures. Finally, the mean age at surgery (35.9 years) is relatively old, which may affect hip instability and postoperative survival rate. However, our cohort includes only Tönnis grade 0 or 1 participants with hip instability. Moreover, even in patients >40 years of age, favorable postoperative outcomes have been reported.6,29,41,48 Therefore, we believe that the effect of age on our study results is negligible.
Conclusion
Our results demonstrate that the severity of hip dysplasia has an effect on hip microinstability before PAO, and that PAO can help alleviate hip microinstability by correcting the acetabulum during surgery, but that it may be challenging to restore normal hip biomechanics because joint incongruity remains unchanged. According to our findings that the femoral head is likely to exhibit a lateralized translation in standing postures in patients with a larger ARO, we believe weightbearing postural radiographs are an invaluable tool for surgeons to comprehend the underlying mechanisms by which PAO improves hip biomechanics and to refine the surgical correction during PAO.
Footnotes
Acknowledgements
The authors thank Takeshi Utsunomiya, MD, Ryosuke Yamaguchi, MD, and Taishi Sato, MD (Department of Orthopaedic Surgery, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan) for their invaluable advice for this study.
Final revision submitted August 9, 2024; accepted September 26, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by research grants from the Uehara Memorial Foundation and the International Research Fund for Subsidy of Kyushu University School of Medicine Alumni. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Florida (IRB202301147).