
Abstract
Background:
The development of posttraumatic osteoarthritis (PTOA) of the knee after anterior cruciate ligament (ACL) reconstruction (ACLR) leads to additional morbidity in adults.
Purpose:
To determine the 5-year incidence of and risk factors for PTOA diagnoses after primary ACLR in pediatric patients.
Study Design:
Case control study, Level of evidence, 3.
Methods:
A United States-based insurance database was used to identify patients aged ≤16 years who underwent primary ACLR from 2010 to 2019 and had at least 5 years of follow-up data. Patients with multiligament knee injuries, tibial eminence avulsion fractures, congenital/syndromic ACL absence syndrome, juvenile idiopathic arthritis, previous knee osteoarthritis or PTOA diagnoses, or previous knee injuries/surgeries were excluded. Demographic factors and concomitant meniscal and cartilage procedures at the time of primary ACLR were recorded. Delayed ACLR was defined as ≥3 months between initial ACL injury diagnosis and ACLR. We also recorded the presence of subsequent motion restoration reoperations, including lysis of adhesions and/or manipulation under anesthesia, after primary ACLR but before PTOA diagnosis. Risk factors for PTOA were evaluated using multivariable logistic regression.
Results:
Included were 16,935 patients (mean age at surgery, 15.1 ± 1.2 years; 62% women). PTOA was diagnosed in 267 patients (1.6%) within 5 years after ACLR; 148 of these patients (55.4%) were diagnosed within 2 years after ACLR. Independent risk factors associated with PTOA diagnosis included subsequent motion restoration procedures (odds ratio [OR], 5.03 [95% CI, 3.31-8.25]; P < .001), age ≥12 years at the time of ACLR (OR, 4.82 [95% CI, 1.54-29.20]; P = .027), delayed ACLR (OR, 1.87 [95% CI, 1.43-2.43]; P < .001), obesity (OR, 1.40 [95% CI, 1.01-1.94]; P = .046), and male sex (OR, 1.36 [95% CI, 1.06-1.74]; P = .015). Performing concomitant partial meniscectomy, meniscus repair, and cartilage restoration at the time of ACLR was not significantly associated with PTOA.
Conclusion:
The incidence of PTOA diagnoses was low within 5 years after primary ACLR in patients ≤16 years old with no subsequent cartilage, meniscus, and/or revision ligament procedures. The need for subsequent motion restoration procedures, age ≥12 years at the time of ACLR, delayed ACLR, obesity, and male sex were significant risk factors associated with a PTOA diagnosis.
Keywords
Anterior cruciate ligament (ACL) injuries have been associated with an increased risk of developing posttraumatic osteoarthritis (PTOA) of the knee.3,12,20,28 While the primary goal of ACL reconstruction (ACLR) is to restore joint stability, additional benefits of the procedure include minimizing the contact pressures on the menisci and articular cartilage surfaces, which has been suggested to decrease the risk of PTOA compared with ACL-deficient knees.5,6,19 PTOA is most commonly diagnosed with the presence of symptomatic pain combined with radiographic evidence of osteoarthritis (OA).6,20 Despite the positive benefits of ACLR, studies have demonstrated that the incidence of symptomatic PTOA in adults is up to 50% within 20 years of undergoing ACLR.6,20 As such, much effort has been directed toward preventing PTOA through the identification of modifiable risk factors associated with PTOA development, as treatment options remain limited. 28
Several important risk factors have been associated with early PTOA after ACLR—including age (>35 years), obesity, chronic ACL injuries or delayed ACLR, concomitant meniscectomy, meniscal repair, depression, and tobacco use, among several others.6,14,15 While the incidence and risk factors for PTOA have been well reported for adults undergoing ACLR, there are limited studies that have investigated the characteristics associated with PTOA development in pediatric patients undergoing ACLR. Importantly, it is unknown whether the aforementioned risk factors in adults are generalizable to pediatric patients who experience different injury patterns, have different tissue compositions compared with adults, and often demonstrate ligamentous hyperlaxity.8,22 In addition, treatment options for PTOA are even more limited in pediatric patients; therefore, prevention is especially important for this specific patient population. 13
Given the annual rise in pediatric ACLRs and limited studies on PTOA in this population,4,16 defining the incidence of and risk factors for PTOA after pediatric ACLR may be the first step toward prevention in at-risk pediatric patients. As such, the primary purpose of this study was to determine the 5-year incidence of and risk factors for PTOA diagnoses after primary ACLR in pediatric patients.
Methods
Patient Cohort
This study obtained its data from the Mariner 161 PearlDiver Patient Claims Database between 2010 and April 2020. The PearlDiver dataset is a large national administrative claims dataset that contains both inpatient and outpatient insurance claims data from commercial and government insurance from nearly 161 million patients across the United States. Data obtained from the PearlDiver databases do not require institutional review board review, as they output only deidentified population-level data.
Pediatric patients aged ≤16 years at the time of surgery who underwent their first ACLR were identified using Current Procedural Terminology (CPT) code 29888 for ACLR. Age ≤16 years was used in this study because previous adult studies on PTOA have commonly included patients >16 years old in their cohorts.14,31 Only patients in the database who had active insurance coverage for 5 years (60 months) after the primary ACLR were included. Patients were also excluded if they had a concurrent multiligament knee injury, congenital/syndromic ACL absence syndrome, juvenile idiopathic arthritis, patellar fracture, tibial eminence avulsion fracture, previous contralateral and/or ipsilateral knee injury and/or surgery, and any diagnosis of knee OA before the primary ACLR, as identified using CPT and International Classification of Disease (ICD)-9 and ICD-10 codes.
At the time of the primary ACLR, demographic information was extracted for each patient; this included age, sex, presence of obesity (defined as ≥95th percentile body mass index [BMI] for their respective age and sex), 24 and the time between the initial ACL injury diagnosis and the primary ACLR (delayed ACLR was defined as those with ≥3 months or 90 days between the initial ACL injury diagnosis and the ACLR). 1 The number of patients who underwent concomitant meniscal repair, partial meniscectomy, and/or cartilage restoration procedures at the time of the primary ACLR was also recorded.
The presence of subsequent or revision procedures—defined as those that occurred after the primary ACLR—was assessed for each patient. As such, to determine the effects of primary ACLR on the eventual diagnosis of PTOA as well as to control for the laterality of subsequent procedures, patients who underwent revision/subsequent ACLR, cartilage procedures, partial meniscectomy, and/or meniscal repair were excluded because we could not definitively ascertain from the database whether these revision procedures were being performed on the contralateral or ipsilateral knee, which could have produced a confounding effect on the eventual PTOA diagnosis. However, we were able to record the patients who underwent subsequent motion restoration surgery (either manipulation under anesthesia [MUA; CPT code 27570] or lysis of adhesion [LOA; CPT code 29884]) after the primary ACLR but before the diagnosis of PTOA. 14
Since the study cohort only included patients without previous knee injuries/surgeries (on either knee) and excluded patients who underwent subsequent ACLR, cartilage, or meniscal procedures on either knee after the primary ACLR, we believed the assessment of subsequent motion restoration procedures—MUA and LOA—was warranted because these procedures would be more specific for isolated arthrofibrosis within the ipsilateral knee that underwent the primary ACLR compared with the contralateral knee that presumably had no history of previous injury and did not undergo ACLR, meniscal or cartilage procedures during the 5-year study period.
The primary outcome assessed was the incidence of subsequent diagnosis of knee PTOA at 5 years after the primary ACLR. While the specific criteria for diagnosing PTOA were not available in the database, the presence and time of PTOA onset were determined by using ICD-9 and ICD-10 codes for PTOA of the knee that were documented by any provider in a subsequent visit after the primary ACLR, as used in previous studies. 14 It is important to note that ICD-9 and ICD-10 codes differ for primary OA and PTOA of the knee.
Risk Factors for PTOA
Patients were then stratified into 2 cohorts based on the presence or absence of a knee PTOA diagnosis within 5 years after primary ACLR. The following risk factors for PTOA diagnoses were then assessed: male (vs female) sex; obesity (vs no obesity); delayed ACLR (vs acute ACLR); the presence (vs absence) of concomitant meniscectomy; meniscal repair; or cartilage procedures at the time of ACLR; and the presence of a subsequent motion restoration procedure after primary ACLR but before the PTOA diagnosis (vs the absence of a subsequent motion restoration procedure). Pediatric patients aged <12 years are commonly considered prepubescent, are often less skeletally mature, and can require different reconstruction techniques compared with those aged ≥12 years 16 ; therefore, age ≥12 years at the time of ACLR (vs <12 years at the time of ACLR) was assessed as a potential risk factor for PTOA.
Statistical Analysis
Patient characteristics were compared between those with and without subsequent PTOA diagnoses after primary ACLR using the chi-square test for categorical variables and the independent t test for continuous variables. Multivariable logistic regression was performed to determine independent factors associated with increased odds of a PTOA diagnosis within 5 years of ACLR. Odds ratios (ORs) with 95% CIs were determined for each risk factor. Multivariable logistic regression included the following variables in the analysis: sex (male or female); obesity; age ≥12 years; concomitant procedures at the time of ACLR (partial meniscectomy, meniscal repair, and/or cartilage restoration); subsequent motion restoration surgery after ACLR; and delayed ACLR. Survival analysis was performed >5 years after primary ACL as the start point, with the primary endpoint being the presence of PTOA diagnosis. Univariable analysis and multivariable logistic regression were performed in PearlDiver Bellwether’s RSuite software (PearlDiver Inc). Figures were created using GraphPad Prism 10 (GraphPad Software). The significance for both univariable and multivariable analysis was determined based on the 2-tailed P≤ .05.
Results
After excluding 3222 patients from analysis because of undergoing subsequent ACLR, meniscectomy, or meniscal repair on either side, data from 16,935 pediatric patients (mean ± SD age at the time of surgery, 15.1 ± 1.2 years; 62% women) who underwent primary ACLR were included in the analysis. The age distribution for the entire cohort at the time of primary ACLR was as follows: 161 (0.9%) patients were ≤10 years old, 407 (2.4%) were 11 to 12 years old, 3358 (19.8%) were 13 to 14 years old, and 13,009 (76.9%) were 15 to 16 years old.
At 5 years after primary ACLR, 267 (1.6%) pediatric patients were diagnosed with PTOA. Of these 267 patients, 148 (55.4%) were diagnosed within 2 years after ACLR. The survival curve with regard to PTOA after primary ACLR is depicted in Figure 1. The baseline characteristics for the PTOA and no-PTOA cohorts are described in Table 1.
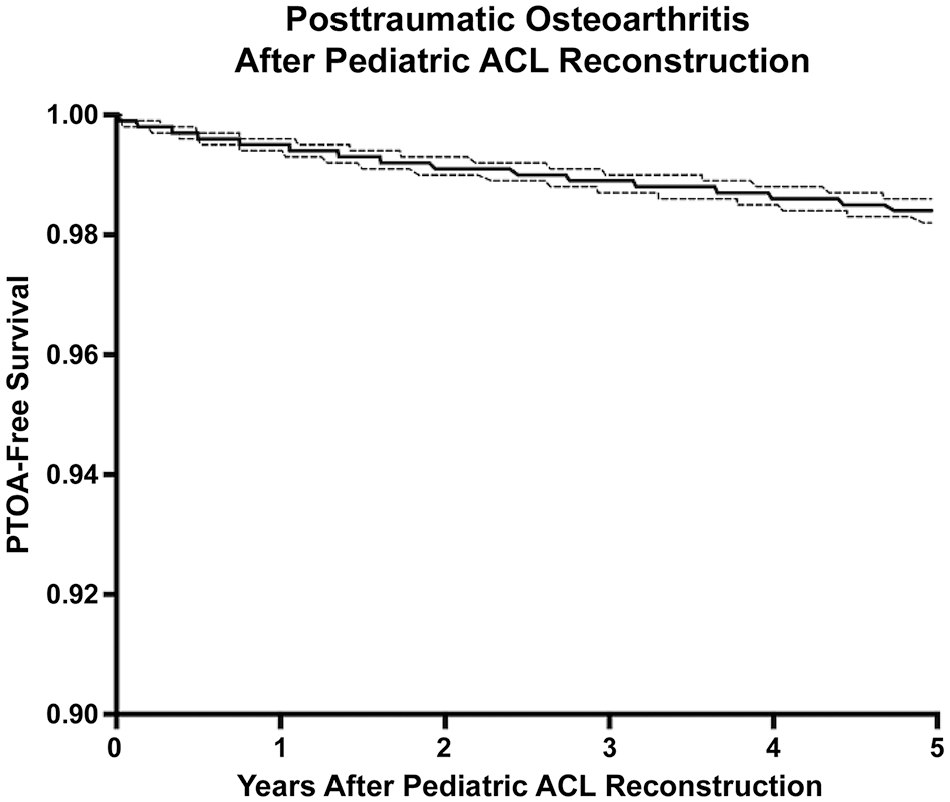
A survival curve of the first 5 years after primary ACLR and subsequent PTOA diagnosis. Note that the Y-axis in the current figure bottoms out at 0.90 (instead of 0) to better highlight the shape of the curve. The dotted lines indicate the 95% CI. ACLR, anterior cruciate ligament reconstruction; PTOA, posttraumatic osteoarthritis.
Comparison of Baseline Characteristics at the Time of ACLR for Pediatric Patients With and Without a Subsequent PTOA Diagnosis a

Data are presented as mean ± SD, %, or n (%). P values were computed using univariate analysis; the bold P value indicates a statistically significant difference between groups (P≤ .05, 2-tailed). ACLR, anterior cruciate ligament reconstruction; PTOA, posttraumatic osteoarthritis.
The PearlDiver database blinds the values that have <10 patients to protect patient data.
Risk Factors for PTOA After Pediatric ACLR
Subsequent motion restoration procedures (OR, 5.03 [95% CI, 3.31-8.25]; P < .001), age ≥12 years old at the time of ACLR (OR, 4.82 [95% CI, 1.54-29.20]; P = .027), delayed ACLR (OR, 1.87 [95% CI, 1.43-2.43]; P < .001), obesity (OR, 1.40 [95% CI, 1.01-1.94]; P = .046), and male sex (OR, 1.36 [95% CI, 1.06-1.74]; P = .015) were independent risk factors significantly associated with a PTOA diagnosis 5 years after ACLR (Table 2).
Risk Factors Associated With Increased Odds of a PTOA Diagnosis 5 Years After Primary ACLR a

Data are presented as n (%) unless otherwise indicated. P values were computed using multivariable logistical regression; bold P values indicate statistical significance (P≤ .05, 2-tailed). ACLR, anterior cruciate ligament reconstruction; OR, odds ratio; PTOA, posttraumatic osteoarthritis.
The PearlDiver database blinds the values that have <10 patients to protect patient data.
Discussion
The most important findings of the present study are as follows: (1) the incidence of PTOA was 1.6% within 5 years after primary ACLR in those who were ≤16 years old at the time of the index procedure, with no subsequent cartilage, meniscal, and/or revision ligament procedures; and (2) important risk factors that conferred an increased likelihood of PTOA development in this specific patient population were the need for subsequent motion restoration procedures, age ≥12 years at the time of ACLR, delayed ACLR ≥3 months, obesity, and male sex.
The incidence of PTOA within 5 years after ACLR has been well reported in the adult patient population,3,6,9,13,14,17,20,28,30 although the present study is one of the first to our knowledge to describe this incidence in a pediatric population. Indeed, the overall incidence of PTOA in pediatric patients who underwent primary ACLR was low at 1.6%. Cinque et al 6 performed a meta-analysis of 38 studies and reported that the pooled 5-year incidence of radiographic PTOA was 11.3% (range, 6.4%-19.1%) after ACLR in adults. Similarly, a recent study that utilized a large administrative database reported a 5-year PTOA incidence of 6.1% of adults, with a mean age of 32.2 years at the time of ACLR. 14 As such, the 5-year incidence of PTOA in pediatric patients appears to be lower than those reported for adults. While older age is a primary risk factor associated with the development of PTOA, 6 the possibility also exists that children and adolescents in the studied age range could be underreporting their symptoms, which could result in fewer diagnoses of pediatric PTOA. 13 Providers may be unaware that children can develop PTOA and may also be reluctant to expose children to radiographs, which could affect the reported incidence of PTOA in this specific patient population. As such, the present study may be diagnostically limited from the use of the presence or absence of PTOA from ICD-9 and ICD-10 codes without radiographic and clinical data on each patient. Future high-quality trials are necessary to better define the incidence of PTOA after ACLR in pediatric patients.
In the present study, we found that 8.2% of pediatric patients who were eventually diagnosed with PTOA underwent at least 1 motion restoration procedure (LOA and/or MUA) after their primary ACLR and that these patients were 5 times more likely to be diagnosed with PTOA compared with those who did not undergo this procedure. Arthrofibrosis has been reported to occur in up to 8.3% of pediatric patients after ACLR in the literature, suggesting concordance between these findings.11,25,26 This postoperative complication can lead to a loss of extension of the knee, which can increase the contact pressures on the articular surface within the joint. While arthrofibrosis is a relatively common complication after pediatric ACLR,10,11 its association with the development of PTOA is understudied in pediatric patient populations. Clinically, previous evidence has suggested that PTOA is more severe in adults with arthrofibrosis compared with adults without this complication after ACLR.18,23 Mayr et al 23 demonstrated this finding in 144 adult patients with post-ACLR arthrofibrosis who underwent arthroscopic LOA within months to years after their ACLR, reporting that 100% of these patients had radiographic evidence of Kellgren-Lawrence grade ≥2 osteoarthritis at a mean follow-up of 18.7 years. One should be aware of this risk factor in pediatric patients who require MUA or LOA after ACLR, as it demonstrated one of the strongest associations with PTOA; therefore, further clinical research should be directed toward optimizing interventions that could further prevent, treat, and better manage postoperative arthrofibrosis, as it may play a role in the development of PTOA after ACLR in pediatric patients.
Delayed ACLR, defined as ≥3 months between the time of ACL injury and ACLR, is associated with an increased risk of developing PTOA in adult patients1,6,15; however, this association between injury chronicity and PTOA is not well understood in the pediatric population. In the present study, 70% of pediatric patients diagnosed with PTOA had ≥3 months between the initial ACL tear diagnosis and ACLR compared with 55.4% in the cohort without PTOA. Moreover, we found that pediatric patients with delayed ACLR ≥3 months were 1.87 times more likely to be diagnosed with PTOA after ACLR compared with those without delayed ACLR. Early ACLR is recommended in pediatric patients, as children with delayed ACLR sustain significantly more meniscal tears and articular cartilage injuries due to an increased number of instability events compared with those with acute or subacute ACLR (<3 months between injury and ACLR).1,2,10,24 These findings may provide additional support for early pediatric ACLR, as delayed surgery not only increases the risk of meniscal and cartilage injuries but perhaps the development of PTOA in pediatric patients.
Study findings also indicated that obesity was a significant risk factor and was present in 16.5% of pediatric patients with PTOA compared with 13.5% in the non-PTOA cohort. Obesity is harder to define in a pediatric population since children go through different growth and puberty stages. Thus, the definition used in this study was a BMI of >95th percentile for the patient’s respective age and sex group, as defined by the United States Centers for Disease Control and Prevention, which has also been used in previous studies.24,27 Obesity is a known risk factor for OA in adults and has been associated with significantly higher rates of meniscal tears and chondral lesions at the time of ACLR in pediatric patients.24,27,29 In the present study, pediatric patients who were obese at the time of their ACLR were 1.41 times more likely to be diagnosed with PTOA within 5 years of ACLR compared with patients with normal BMIs. In these specific at-risk children, clinicians may consider focusing efforts on weight loss interventions. In addition, children and adolescents have been shown to have significantly reduced activity levels and increased weight gain after ACLR, 21 which could further increase the risk of developing PTOA in at-risk obese children.
There was no significant difference in the rate of concomitant partial meniscectomy (39.3% vs 34.8%) or meniscal repair (25.1% vs 22.3%) at the time of ACLR between pediatric patients with or without PTOA diagnoses. These rates are in relative agreement with those reported for 2000 to 2016 by Cruz et al, 7 who demonstrated that newly trained sports surgeons performed concomitant meniscal repairs in 27% of pediatric ACL injuries and meniscectomy in 31%. However, the finding of no association with PTOA is surprising, as meniscectomy is a known risk factor that has been associated with the development of PTOA at long-term follow-ups in adults.6,28 Many of the studies on PTOA in the adult literature have reported data with a 10- to 20-year follow-up period. Given the young age of the present cohort, it is possible that our 5-year follow-up is insufficient to capture the adverse manifestations of concomitant meniscal procedures in terms of altered tibiofemoral contact pressures and resultant chondral damage. Future studies may use these findings as a catalyst to investigate the long-term outcomes in pediatric patients who undergo concomitant meniscal procedures at the time of ACLR and their association with the development of PTOA, as the present data are confined to a 5-year postoperative surveillance period.
Limitations
As with all studies that utilize national insurance databases, the results can be affected by ICD-9 and ICD-10 codes and CPT codes and are reliant on physician entry. The ICD-9 codes do not include laterality (right vs left); thus, PTOA diagnosis of the contralateral knee or ipsilateral knee that underwent primary ACLR could not be definitively determined. However, the methodology used to control for this potential limitation—excluding patients with a previous history of knee injury on either knee and any patients who underwent meniscal and/or cartilage procedures on either knee after the primary ACLR—favors the operative knee that underwent the primary ACLR. The presence of a PTOA diagnosis was a binary outcome and radiographic data were not available, which could have provided more accurate information on the presence and severity of PTOA. Clinical information—such as graft choice, the use of lateral extra-articular tendinosis, and the location of PTOA (medial or lateral and patellofemoral or tibiofemoral)—were not available. Furthermore, obesity was only assessed at the time of surgery and can often change frequently in adolescents during the postoperative period. Having a longer follow-up period may have revealed more risk factors that were associated with PTOA diagnoses and captured more patients who were eventually diagnosed with PTOA. Last, the activity level of each patient and their respective postoperative rehabilitation protocols should be considered in future clinical studies that investigate the development of PTOA in pediatric patients and could not be captured with the present database.
Conclusion
The incidence of PTOA diagnoses was 1.6% within 5 years after primary ACLR in pediatric patients who were ≤16 years old and who had no subsequent cartilage, meniscal, and/or revision ligament procedures. The need for subsequent motion restoration procedures, age ≥12 years at the time of ACLR, delayed ACLR ≥3 months, obesity, and male sex were significant risk factors associated with a PTOA diagnosis. These findings may help identify at-risk pediatric patients and can act as a catalyst for developing future clinical studies that focus on preventive interventions for pediatric PTOA.
Footnotes
Final revision submitted July 25, 2024; accepted September 5, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.C. has received consulting fees from Arthrex, ConMed Linvatec, Ossur, and Smith & Nephew. A.E.J. has received grant support and education payments from Arthrex. R.F.L. has received research support from Arthrex and Linvatec and consulting fees from Ossur and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.