
Abstract
Background:
Contralateral donor autografts in anterior cruciate ligament (ACL) reconstruction (ACLR) may act as an alternative to conventional ipsilateral donor grafts but are rarely used clinically because of the lack of evidence on patient outcomes and concerns around additional morbidity.
Purpose:
To investigate the effect of contralateral versus ipsilateral autograft use in ACLR on patient outcomes.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
The MEDLINE, Embase, and Cochrane Central Register of Controlled Trials databases were searched from inception to October 2022 for comparative studies assessing the clinical or functional outcomes of ipsilateral versus contralateral autograft harvest in primary or revision ACLR. Given the heterogeneity of the included studies, data were summarized using descriptive statistics.
Results:
Included were 11 studies representing 1638 patients with a mean follow-up of 49 months. The mean time to return to sport was shorter in patients treated with a contralateral bone–patellar tendon–bone (BPTB) autograft in 2 of 3 studies that evaluated this outcome after primary ACLR and in the only study that evaluated this outcome after revision ACLR. Some studies found improved strength recovery in the contralateral ACL-reconstructed knee. Otherwise, there was no significant difference between contralateral and ipsilateral ACLRs on subjective or objective postoperative clinical outcome scores. Most studies reported minimal donor site morbidity. Clinical adverse events including postoperative graft rerupture and infection were low in both contralateral and ipsilateral ACLRs and were not significantly different.
Conclusion:
Contralateral ACL autograft harvest may lead to earlier return to sport when patients undergo BPTB ACLR. However, clinical outcomes, morbidity, risk of rerupture, and risk of donor knee injury were not significantly different in this review.
Ligamentous injury is the most common cause of knee pathology, with the anterior cruciate ligament (ACL) most frequently implicated. 5 Rates of primary ACL reconstruction (ACLR) to resolve such injuries continues to increase year by year.10,20 Graft selection plays an important role in primary and revision ACLR given its impact on donor site morbidity and risks of graft rupture.
Hamstring tendon (HT) autograft is most commonly selected followed by bone–patellar tendon–bone (BPTB) autograft for primary and revision ACLR. 13 The donor site morbidity of BPTB grafts is greater than that of HT autografts, although they demonstrate greater rotational stability and lower rerupture rates. 12 BPTB grafts have greater anterior knee pain, but in certain populations may have a reduced risk of rerupture. 31 Allograft is another option, but it is typically reserved for relatively older patients or ones with lower sport demands, as they have been reported to have the greater failure rates.6,31
In our surgical centers, the majority of donor autografts are extracted from the ipsilateral injured knee, with a minority of operations harvesting grafts from the contralateral uninjured knee. This may be because of the surgical flow ease, potential challenges of recovery from bilateral lower extremity surgery, and epidemiological data exhibiting increased rates of contralateral ACL tears after primary ACLR.1,14 The rate of such contralateral ACL ruptures was also increased in female patients who underwent contralateral graft harvest. 1
Contralateral grafts have typically been used as an alternative to ipsilateral grafting in the event of insufficient tendon harvest, graft contamination, or limited ipsilateral graft availability in the revision setting. 2 However, utilizing the autograft from the uninjured knee may lead to favorable clinical outcomes and rehabilitative progress by distributing morbidity between the 2 knees and thus decreasing the morbidity in the reconstructed knee.
The purpose of this review was to summarize the current evidence investigating the postoperative clinical outcomes of contralateral versus ipsilateral donor autograft in primary and revision ACLRs. Our hypothesis was that donor autograft harvested from the contralateral uninjured knee would lead to improved donor site morbidity, as the surgical insult is spread across 2 knees, with similar clinical outcomes and similar return-to-sport time to conventional ACLR.
Methods
Search Strategy and Study Eligibility
This systematic review was performed in adherence with the PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analyses) guidelines. 18 The Embase, MEDLINE, and Cochrane Central Register of Controlled Trials electronic databases were systematically searched from inception to October 12, 2022, for articles comparing the use of contralateral donor autograft and ipsilateral donor graft in ACLR. A combination of the following search terms were utilized to perform the search: “anterior cruciate ligament,”“reconstruction,”“contralateral,”“opposite,” and/or “uninjured.” The complete search strategy is summarized in Appendix Table A1.
The inclusion criteria were (1) primary or revision ACLR, (2) ACLR utilizing donor autograft from the contralateral uninjured knee, (3) postoperative clinical outcomes reported, (4) comparative studies, (5) human studies, and (6) studies published in the English language. The exclusion criteria were (1) comparator group utilizing a different autograft option (ie, BPTB vs HT vs quadriceps tendon), (2) technical reports, (3) review studies, (4) conference abstracts, and (5) in-progress clinical trial abstracts.
Study Screening and Assessment of Reviewer Agreement
Two reviewers (J.S.S. and E.Y.) independently screened the abstracts and titles of the articles imported. Discrepancies between reviewers at any stage of screening were resolved after discussion. References in included papers were screened for additional studies not included in the initial review. Interrater reliability was assessed at all stages of screening using the kappa (κ) statistic. 16
Quality Assessment
Two reviewers (J.S.S. and E.Y.) independently assessed the quality of the included articles. Nonrandomized studies were assessed using the Methodological Index for Non-Randomized Studies (MINORS) score, whereas randomized studies were examined using Version 2 of the Cochrane risk-of-bias tool for randomized trials (RoB 2).25,26 After independently assessing study quality, the 2 reviewers discussed their scores until consensus was reached.
Statistical Analysis
Data were independently extracted by 2 reviewers (J.S.S. and E.Y.) using Covidence systematic review software (Veritas Health Innovation) and Google Sheets. The main outcomes assessed in this review were postoperative clinical and rehabilitative outcomes. Subjective outcomes that were extracted and analyzed included the Lysholm score, International Knee Documentation Committee (IKDC) subjective score, and Tegner activity level. Objective clinical outcomes included the Lachman test, pivot-shift test, side-to-side difference in anterior translation, and objective IKDC grade. Rehabilitative outcomes included measurements of knee strength (flexion and extension), donor site morbidity, and return-to-sport time. Secondary outcomes included operation duration and adverse events. Data were summarized using descriptive statistics, but meta-analysis was not performed as the data were too heterogeneous.
Results
Results of Literature Search
The literature search identified 3275 studies, of which 1310 duplicates were removed. The titles and abstracts of 1939 studies were assessed, and 1963 were excluded. In total, 24 studies were advanced to full-text review, and of these, 13 studies § met the inclusion and exclusion criteria for data extraction (Figure 1). The interreviewer agreement was strong at both the title/abstract (κ = 0.916; 95% CI, 0.833-0.998) and full-text (κ = 0.923; 95% CI, 0.776-1.000) review stages.

PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analyses) flowchart of systematic search engaged for studies regarding use of contralateral graft for anterior cruciate ligament reconstruction.
Study Quality
The characteristics of the included studies are summarized in Table 1. Of the 13 included studies, 3 studies3,8,17 were of level 1 evidence, 5 studies15,24,28-30 were of level 2, 4 studies4,7,11,21 were of level 3, and 1 study 19 was of level 4 evidence. The mean MINORS score for the 7 nonrandomized studies was 17 of a possible 24. The overall risk of bias for the 4 randomized studies that were assessed using RoB 2 demonstrated some concerns, with 1 article having a high risk of bias in selection of reported data. 8
Characteristics of the Included Studies a
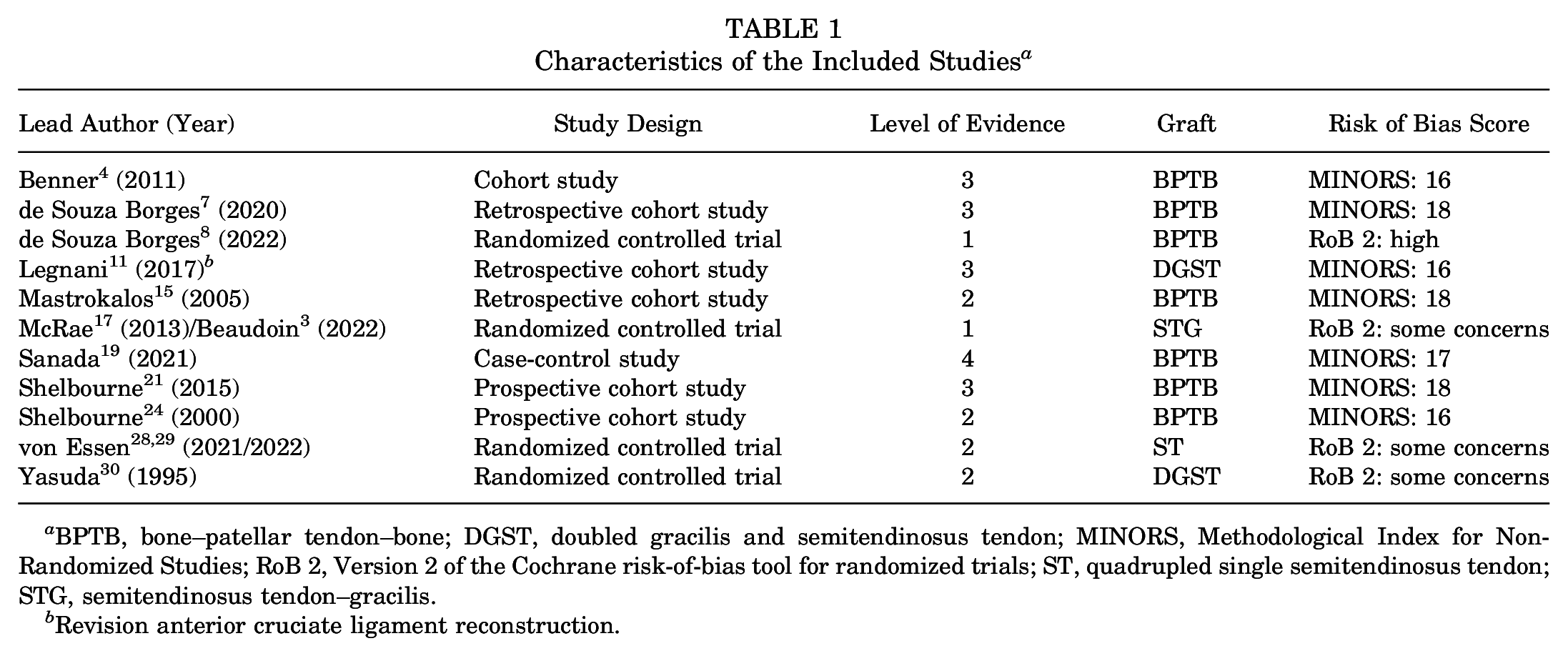
BPTB, bone–patellar tendon–bone; DGST, doubled gracilis and semitendinosus tendon; MINORS, Methodological Index for Non-Randomized Studies; RoB 2, Version 2 of the Cochrane risk-of-bias tool for randomized trials; ST, quadrupled single semitendinosus tendon; STG, semitendinosus tendon–gracilis.
Revision anterior cruciate ligament reconstruction.
Study and Intervention Characteristics
Six studies3,17,11,28,29,30 used HT, and 7 studies4,7,8,15,19,21,24 used BPTB autografts for ACLR. Of those that used HT autografts, 1 study 30 investigating primary ACLR and 1 study 11 assessing revision ACLR used a doubled gracilis and semitendinosus tendon. Two groups of included studies (McRae et al 17 /Beaudoin et al 3 and von Essen et al28,29) included 2 articles that reflected the same study cohort with different measured outcomes and/or different timelines; therefore, they were combined when reporting outcomes. The combined studies by McRae et al 17 and Beaudoin et al 3 used semitendinosus tendon–gracilis, and the studies by von Essen et al28,29 used a single semitendinosus tendon that was quadrupled (Table 1). The mean reported follow-up time among all studies was 49 months. Among the 11 studies, 10 focused on primary ACLR, while 1 study 11 focused on revision ACLR. For this reason, all data presented are for primary ACLR unless otherwise specified.
The included studies consisted of 1638 patients overall. The patient characteristics are presented in Table 2. All comparisons were between the ipsilateral injured (ie, reconstructed) knee and the contralateral injured knee or the ipsilateral noninjured (nonreconstructed) knee and the contralateral graft knee.
Characteristics of the Included Patients (N = 1638) a

Dashes indicate the data were not reported. BPTB, bone–patellar tendon–bone; C, contralateral; DGST, doubled gracilis and semitendinosus tendon; I, ipsilateral; ST, quadrupled single semitendinosus tendon.
Mean or mean ± SD.
Revision anterior cruciate ligament reconstruction.
Subjective Outcomes
Subjective clinical outcomes are presented in Table 3. Overall, no significant differences were found in the various subjective scores recorded.
Subjective Clinical Outcomes in Primary ACLR a

Data are presented as mean or mean ± SD unless otherwise indicated. Dashes indicate the data were not reported. ACLR, anterior cruciate ligament reconstruction; C, contralateral; I, ipsilateral; IKDC, International Knee Documentation Committee.
Median values.
IKDC Subjective, Lysholm, and Tegner Scores
Two studies21,28 (235 patients) examined the IKDC subjective scores after final follow-up and found no differences between the groups. The 2021 study by von Essen et al 28 evaluated the score at several follow-up intervals, reporting no differences at each follow-up. Only 1 study 28 examined the Lysholm score in both contralateral and ipsilateral ACLRs and demonstrated no differences at any follow-up. Four studies3,15,19,28 assessed Tegner activity level postoperatively in primary ACLR, with no significant differences between the ipsilateral and contralateral groups at all time points measured.
Other Subjective Outcome Scores
In terms of the Cincinnati Knee Rating System, Mastrokalos et al 15 demonstrated mean scores of 82 and 83.7 in the ipsilateral and contralateral groups, respectively, in a sample of 100 patients with no significant differences. McRae et al 17 assessed Anterior Cruciate Ligament–Quality of Life scores at 3 months, 6 months, 12 months, and 24 months and did not find any differences at any time point.
Objective Clinical Outcomes
IKDC Objective Grade
There was no significant difference found in IKDC objective grade between the ipsilateral and contralateral groups in the one study 17 that examined such outcomes after 24 months (95 patients).
Lachman and Pivot-Shift Tests
Two studies19,28 (120 patients) examined the Lachman and pivot-shift tests at final follow-up of the knee that underwent ACLR. Lachman grade 0 was achieved in 61 of 63 (96.8%) patients in the ipsilateral group and 62 of 65 (95.4%) patients in the contralateral group when combining these 2 studies. Pivot-shift grade 0 was achieved in 55 of 63 (87.3%) and 60 of 65 (92.3%) patients in the ipsilateral and contralateral groups, respectively. Overall, there were no significant differences observed between the 2 groups in either of the studies.19,28
Anterior Translation
Seven studies15,17,19,21,24,28 evaluated anterior translation in primary ACLR. There were no differences reported in any of the studies other than that of Shelbourne and Urch, 24 which found that the mean side-to-side differences in anterior translation were 1.72 ± 1.59 mm and 1.77 ± 1.41 mm in the ipsilateral (211 patients) and contralateral (402 patients) groups, respectively (P = .0361).
Extension and Flexion Strength
Five studies19,21,24,29,30 compared extension strength postoperatively as compared with the noninjured leg preoperatively (Table 4). In the reconstructed knee there was significantly greater extension strength found by Shelbourne et al 21 at 2 years postoperatively (P < .01), von Essen et al 28 at 6 and 12 months (P < .05, no means reported), and de Souza Borges et al 8 at 4 months (P < .0001) when comparing the contralateral reconstructed knee versus the ipsilateral reconstructed knee. When comparing the ipsilateral noninjured knee and the contralateral graft knee, Sanada et al 19 found in the early postoperative period (4-6 months and 12 months) that there was increased extension strength in the ipsilateral noninjured knee.
Postoperative Strength After Primary ACLR a


Data are presented as mean ± SD. Rows shaded in gray indicate hamstring tendon graft was used; otherwise, bone–patellar tendon–bone graft was used. Dashes indicate the data were not reported. Statistically significant difference between groups: *P < .05, **P < .01, ***P = .001. ACLR, anterior cruciate ligament reconstruction; C, contralateral; I, ipsilateral.
Four studies19,28-30 compared flexion strength of the injured knee with the noninjured leg preoperatively (Table 4). When comparing the contralateral reconstructed knee and the ipsilateral reconstructed knee, von Essen et al 28 found significantly greater isokinetic torque on the contralateral reconstructed knee at 6, 12, and 24 months (P < .05, no means reported). When comparing the contralateral graft knee and the ipsilateral noninjured knee, von Essen et al 29 found significantly greater isokinetic torque in the noninjured leg (P = .001). While this significance disappeared at 12 and 24 months, there was a trend toward greater strength in the noninjured leg.
Return to Sports
Three studies,15,19,24 all of which used a BPTB autograft, evaluated return to sport after primary ACLR (Table 5). Sanada et al 19 and Shelbourne and Urch 24 found that those in the contralateral group returned to sport significantly sooner than those in the ipsilateral subgroup.
Return to Sport After Primary ACLR a

Data are reported as mean or mean ± SD. Statistically significant difference between groups: *P < .01, **P = .012. ACLR, anterior cruciate ligament reconstruction.
Mastrokalos et al 15 also evaluated time from surgery to activities of daily living and found that patients returned at a mean of 5.2 weeks for the ipsilateral group and 4.9 weeks for the contralateral group.
Morbidity
Donor site morbidity due to graft harvesting was assessed by 7 studies4,7,8,15,19,21,28 (924 patients with contralateral harvest), of which 2 used HT autograft and 5 used BPTB autograft. Assessment of morbidity was heterogeneous and included symptomatic assessment, use of questionnaires, anesthetic requirements, or pain scores. Four studies8,21,30 (791 patients) reported minimal pain or disability secondary to graft harvest. The 2022 study by von Essen et al 29 found of those who underwent contralateral ACLR, from 66% to 73%, 25% to 33%, and 0% to 6% of patients had none, mild, and moderate pain, respectively, at their donor site at 6 to 24 months of follow-up. No patients had severe pain at any follow-up. Mastrokalos et al 15 evaluated 48 patients who underwent contralateral ACLR with BPTB autograft and found that 85.4% of donor knees were symptomatic at a mean follow-up of 31.7 months. Overall, 58.3%, 70.9%, and 70.8% of patients reported local tenderness, kneeling pain, and knee walking pain, respectively.
Rerupture Rate
Four studies3,15,19,24 evaluated rerupture rate, with no significant differences found. In the ipsilateral group, there were 5 reruptures (340 patients) in the reconstructed knee and 4 reruptures (234 patients) in the noninjured knee. In the contralateral group, there were 4 reruptures (547 patients) in the reconstructed knee and 2 ruptures (499 patients) in the donor knee.
Infection
Several studies8,15,17,19,24,28 recorded adverse events, with no infections reported in either the ipsilateral or contralateral group. Benner et al 4 evaluated outcomes specifically in patients with postoperative infections after ACLR. They reported 9 postoperative infections in a sample of 2553 ipsilateral ACLRs and 4 postoperative infections in a sample of 2811 contralateral ACLRs. The difference was not statistically significant.
Operation Time
Only von Essen et al 28 (137 patients) compared operation duration between groups. The authors reported mean operating times of 74 ± 15 minutes in the ipsilateral group and 83 ± 14 minutes in the contralateral group, with no significant difference between the groups.
Revision ACLR
Only 1 study 11 evaluated revision ACLR. Legnani et al 11 assessed patients who underwent revision ACLR with a HT autograft with 22 and 23 patients utilizing ipsilateral and contralateral grafts, respectively. There were no differences in IKDC subjective score, Tegner activity level, Lachman sign, pivot shift, or anterior laxity. However, return to sport occurred at means of 14.3 months and 9.8 months in the ipsilateral and contralateral groups, respectively (P < .001).
Discussion
This systematic review demonstrated that patients who underwent contralateral knee donor autograft for ACLR may have quicker times to return to sport. However, regardless of the graft used, there were minimal differences in subjective or objective clinical outcomes using an autograft from the ipsilateral or contralateral leg. Therefore, these results indicated that contralateral ACLR is a viable alternative to the traditional ipsilateral technique given that there was no increase in knee morbidity, risk of contralateral knee injury, or risk of graft rerupture.
One of the most common concerns reported in the literature as to why surgeons do not complete a contralateral ACLR is donor site morbidity and, subsequently, the second leg being injured.19,21,24 Subjective and objective clinical outcomes that evaluated both the patient holistically and the individual knee (ipsilateral and contralateral) had largely equivalent outcomes. The studies that specifically assessed donor site morbidity and pain found that there was minimal long-term pain and disability secondary to the graft harvest. Only Mastrokalos et al 15 found that a large proportion of patients (85%) had symptomatic donor knees in the long term; however, this was similar to their results with ipsilateral ACLR. It seems reasonable to conclude that donor site morbidity likely poses a low risk for having a substantial clinical impact, but given the heterogeneity of the studies, more research would be beneficial.
Another potential reason for not undergoing contralateral ACLR is concern regarding issues with rehabilitation. Regarding strength outcomes, most studies report no difference in extension or flexion strength at any of the time points recorded.
Regarding the use of BPTB autografts, 1 study 19 found that there was decreased extension strength at both 5 and 12 months of follow-up in the donor BPTB contralateral knee when compared with the noninjured knee in patients undergoing ipsilateral knee donor ACLR, while 2 studies of a combined 425 patients demonstrated increased extension strength in the contralateral reconstructed knee when compared with the ipsilateral reconstructed knee.19,21 Regarding the use of HT autografts, there was no difference found in strength outcomes other than the 2 studies by von Essen et al.28,29 They found that the ipsilateral reconstructed knee was weaker than the contralateral reconstructed knee at 6 to 24 months of follow-up and at 6 to 12 months of follow-up in flexion and extension, respectively. Furthermore, the ipsilateral noninjured knee was stronger than the contralateral graft knee at the 6-month follow-up.
It seems likely that there is a negative effect that graft harvest has on extension and flexion strength in BPTB and HT autografts, respectively. Even in studies that did not find significant group differences, there was a trend toward this outcome. However, this negative effect may be more pronounced in the reconstructed leg, as the donor knee can begin immediately focusing on strengthening without limitation in the graft knee, while the reconstructed knee can focus on range of motion instead of attempting to balance both goals in one knee.21-24
This potentially improved rehabilitation may also be demonstrated by the earlier return to sport shown in studies comparing contralateral vs ipsilateral grafts in BPTB autografts.11,19,24 Only Shelbourne and Urch 24 assessed competitive athletes as a separate subgroup and found that the results were consistent with those receiving the contralateral graft returning to sport earlier. This outcome was not evaluated in those receiving a HT autograft. In patients for whom early return to sport is important, these results may lead surgeons to consider a contralateral graft when using BPTB autografts.
Lastly, a final reason as to why contralateral grafts may not be used is secondary to a concern regarding increased operative time. Only von Essen et al 28 evaluated it as an outcome, finding no statistically significant difference but a trend toward increased operative time in contralateral ACLR (mean, 83 vs 74 minutes).
Revision ACLR has an incidence for 1% to 4% at 5 years 27 and has consistently inferior outcomes when compared with primary ACLR. Failed ACLR is generally defined as anterior laxity ≥6 mm but may include significant pain and stiffness, or rerupture of the graft. 9 In revision scenarios, previous bone tunnels may need to be completely redrilled if malpositioned with the graft remaining in situ. If that is not possible, the tunnels need to be assessed and may require several additional modes of fixation. Allografts have previously been a very common choice in revision ACLR but have more recently been avoided given increased rerupture rates. 27 For this reason, contralateral autografts may commonly be considered in revision scenarios as ipsilateral graft sources are already used. Only Legnani et al 11 evaluated this population, with a small sample size and a nonrandomized design. They demonstrated equivalent IKDC subjective and objective clinical outcomes in both the contralateral and ipsilateral groups, with earlier return to sport in the contralateral group. While these results are interesting, further research in revision scenarios is certainly required.
Strengths and Limitations
The strengths of our review include the large number of patients included in several studies, many of which were completed quite recently. We also evaluated many subjective and objective outcomes, which all indicated that contralateral ACLR is likely equivalent to ipsilateral ACLR. However, our review was limited by the availability of only a few high-quality level 1 and level 2 studies. There were also concerns of heterogeneity between autograft options, although all studies used BPTB or HT. However, this issue was further compounded by the fact that the HT autografts varied in the studies (either quadrupled semitendinosus tendon, semitendinosus tendon–gracilis, or doubled gracilis and semitendinosus tendon). Furthermore, although quadriceps tendon autografts are gaining in popularity, there were no studies that examined contralateral quadriceps ACLR. Given the heterogeneity in study outcomes, we were only able to report descriptive statistics. Lastly, none of the studies stratified results on concomitant injuries such as meniscal tears, chondral defects, and additional ligament damage or included patients who underwent anterolateral ligament reconstruction alongside ACLR, which further limited our ability to apply these results to specific patient populations.
Conclusion
Contralateral ACL autograft harvest may lead to earlier return to sport when patients undergo BPTB ACLR. There may be an improvement in strength recovery in the reconstructed knee when using a contralateral graft. However, clinical outcomes, morbidity, risk of rerupture, and risk of donor knee injury have not been shown to be significantly different. The results of this study will allow surgeons to make well-informed evidence-based decisions on whether harvesting of autograft from the contralateral knee is a viable option for ACLR.
Footnotes
Appendix
Search Strategies Utilized During Systematic Search of Databases for Studies on the Use of Contralateral Donor Autograft in ACLR a

| Set | Search Statement |
|---|---|
| Embase and MEDLINE | |
| 1. | anterior cruciate ligament/ |
| 2. | “anterior cruciate ligament”.ti,ab. |
| 3. | ACL.ti,ab. |
| 4. | 1 or 2 or 3 |
| 5. | operat*.ti,ab. |
| 6. | surg*.ti,ab. |
| 7. | reconstruct*.ti,ab. |
| 8. | 5 or 6 or 7 |
| 9. | 4 and 8 |
| 10. | (contralateral or opposite or uninjured).mp. |
| 11. | 9 and 10 |
| 12. | limit 11 to (human and english language) |
| Cochrane Central Register of Controlled Trials | |
| 1. | anterior cruciate ligament/ |
| 2. | “anterior cruciate ligament”.ti,ab. |
| 3. | ACL.ti,ab. |
| 4. | 1 or 2 or 3 |
| 5. | operat*.ti,ab. |
| 6. | surg*.ti,ab. |
| 7. | reconstruct*.ti,ab. |
| 8. | 5 or 6 or 7 |
| 9. | 4 and 8 |
| 10. | (contralateral or opposite or uninjured).mp. |
| 11. | 9 and 10 |
| 12. | limit 11 to (english language) |
ACLR, anterior cruciate ligament reconstruction.
Final revision submitted July 25, 2024; accepted August 23, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.