
Abstract
Background:
Arthroscopic shoulder capsuloligamentous repair can be performed in the beach-chair (BC) or lateral decubitus (LD) position. Patient positioning may influence anchor placement. Limited research exists evaluating these 2 positioning techniques, specifically with respect to anchor position and trajectory.
Purpose/Hypothesis:
The purpose of this study was to perform a cadaveric imaging analysis of arthroscopic anterior shoulder stabilization in the LD and BC positions. It was hypothesized that repairs performed in the LD position would demonstrate more accurate anterior inferior anchor positioning.
Study Design:
Controlled laboratory study.
Methods:
Nine matched pairs of cadaveric shoulders (18 total shoulders) were used. Specimens underwent arthroscopic anterior inferior labral repair using 3 suture anchors placed in the 3:30, 4:30, and 5:30 positions. Repairs were performed by 2 fellowship-trained orthopaedic surgeons each trained in a respective technique. Specimens then underwent computed tomography analysis to evaluate anchor position and trajectories. Target anchor location was determined using a 3-dimensional computed tomography glenoid model, using ImageJ software, with the clockface overlaid onto the glenoid. The 3-o’clock position was set at 0° for reference, with the 3:30, 4:30, and 5:30 anchor positions set at −15°, −45°, and −75°, respectively. One-tailed t tests were used to compare anchor position deviation with target ideals.
Results:
Inferior anchor (5:30) placement was found to be more accurate in the LD position, while superior anchor (3:30) placement was found to be more accurate in the BC position. Specifically, the LD group did not demonstrate statistically significant deviation from the target ideal (−75°) for the 5:30 anchor. The true deviance for the LD group from the 5:30 target angle was between −78.6° and −58.5° (P = .178), while the BC group did not demonstrate statistically significant deviation for the target ideal (−15°) for the 3:30 anchor. The true deviance from the target angle was between −37.9° and 1.79° (P = .732). Both groups demonstrated adequate anchor trajectories.
Conclusion:
Both positioning techniques remain safe and efficacious. The LD position may offer improved inferior anchor placement, and the BC position may offer improved superior anchor placement. Additional studies are warranted to further elucidate the advantages and disadvantages of each position.
Clinical Relevance:
Knowledge pertaining to the accuracy of anchor placement based on patient positioning and anchor location may aid surgeons in choosing operating positions to potentially optimize anchor placement during arthroscopic anterior shoulder stabilization surgery.
Keywords
Despite substantial improvements in both surgical techniques as well as instrumentation throughout the past decade, recurrent glenohumeral instability remains problematic, with rates reported between 10% and 30% after surgical repair.6,11,17,19,23 The goals of shoulder stabilization surgery are to create an anatomic and secure repair with appropriate capsular tensioning while avoiding complications. 9 Failures are inherently challenging problems that negatively impact outcomes and return to activity in a patient population that is generally relatively young and active. Thus, investigators are continuing to search for ways to improve outcomes and lower recurrence rates. Interestingly, despite the exponential increase in publications analyzing anterior shoulder stabilization in the past decade, one factor that continues to be discussed but is poorly understood is patient positioning.
Arthroscopic shoulder stabilization can be performed in either the beach-chair (BC)21,22 or lateral decubitus (LD) position. Surgeon preference and experience, as well as the specific intended procedure, often dictate which position is utilized. With appropriate setup and positioning, both techniques are reliable for arthroscopic anterior stabilization. The BC position offers the advantage of easy conversion to open techniques, while the LD position may allow for lower suture anchor position on the glenoid. As the typical location of injury in the setting of anterior instability is in the anterior inferior glenoid quadrant, the zone of injury is usually between the 3-o’clock and 7-o’clock positions for a right shoulder. For adequate repair, it is critical that the surgeon achieve inferior anchor placement to address the inferior component of traumatic instability. 20 Modified portal placement and new curved drill guide systems have been proposed as ways to improve inferior anchor placement14,18; however, the potential effect of patient positioning and its relationship to anchor position, including anchor trajectory, has not yet been evaluated. Optimal anchor position and trajectory are important to ensure a robust repair with appropriate integrity. Therefore, the purpose of the current study was to compare the suture anchor placement between both techniques and to evaluate glenoid suture anchor trajectory and position on the glenoid face as a function of technique. It was hypothesized that repairs performed in the LD position would demonstrate more accurate anterior inferior anchor positioning.
Methods
Nine fresh-frozen matched pairs of human shoulder cadaveric specimens, including all soft tissue, the scapula, clavicle, and proximal half of the humerus, were obtained from 2 tissue banks (MD and ScienceCare). There were 5 male donors and 4 female donors. The mean donor age was 41.4 years for men and 48.7 years for women. The mean body mass indices were 19.5 and 28.8 for male and female specimens, respectively (Table 1).
Demographic Data of Specimens Used a

BMI, body mass index.
The specimens were thawed to room temperature and the scapulae were mounted in a clamp to position the shoulder in either the BC or LD position before performing arthroscopic anterior labral repair. Matched pairs were randomized with 1 shoulder mounted in the BC position, and the contralateral side mounted in the LD position. One sports medicine fellowship-trained orthopaedic surgeon (R.M.F.) and 1 shoulder and elbow fellowship-trained orthopaedic surgeon (A.S.) performed all procedures with the assistance of an orthopaedic resident. One surgeon performed all stabilizations in the LD group (R.M.F.), while the other surgeon performed all stabilizations in the BC group (A.S.). Each surgeon operated in their preferred position. Three standard arthroscopic portals were used to access the shoulder joint, including a standard posterior portal, a high midglenoid anterior interval portal, and a low midglenoid accessory portal. The shoulders were first arthroscopically examined for preexisting labral pathology and significant glenohumeral arthritis. For all specimens, the focus was on the anterior inferior quadrants of the glenoid and capsulolabral complex, based on previously published instability study models.7,11,16 The anterior inferior quadrant was defined as the inferior half of the glenoid from the 3-o’clock to the 6-o’clock position (right shoulder). An iatrogenic defect was created arthroscopically in the anterior inferior quadrant from the 3-o’clock to the 6-o’clock position using an arthroscopic scalpel (Samurai Blade, Stryker Sports Medicine; Pivot Medical) or labral elevator. Specimens then underwent suture anchor repair with 3 standard single-loaded 2.9-mm suture anchors (OSTEORAPTOR; Smith & Nephew). For each repair, the goal was to place 3 suture anchors arthroscopically at the 3:30 (superior anchor), 4:30 (middle anchor), and 5:30 (inferior anchor) positions (right shoulder). Each anchor position was determined intraoperatively by the respective surgeon. Based on manufacturer guidelines, a 2.7-mm pilot drill hole was placed approximately 1 to 2 mm onto the face of the glenoid, and each respective suture anchor was inserted to the manufacturer-recommended depth.
To assess the anchor’s location, trajectory, and iatrogenic chondral injury, the specimens were then imaged using computed tomography (CT). Three-dimensional (3D) CT scans were obtained of each specimen at a slice thickness of 0.67 mm. ImageJ software (National Institutes of Health) was used to create a 3D model of the specimens and their respective anchors.
Anchor Location
A 3D model of the glenoid was built in ImageJ from the CT scans. A screenshot of the glenoid was then captured in ImageJ. On the glenoid surface, a line was drawn from the superior-most point (12-o’clock position) to the inferior-most point (6-o’clock position.) The midpoint of that line was the center of the clockface. A horizontal line was drawn through the 3-o’clock position, which was the center point to the anterior edge of the glenoid. The anchor location angle was defined as the angle between the center of the clockface and the center of the anchor. The 3-o’clock position was set to 0°. If the anchor was above the 3-o’clock position (ie, toward the 2-o’clock position), it was a positive angle. If it was below the 3-o’clock position (ie, toward the 4-o’clock position), it was a negative angle. The measurements were then standardized by subtracting the absolute value of these angles from the respective target angle. This standardized the measurements as a deviance from target, as there were 3 different target angles depending on the anchor location (Figure 1).

Representative glenoid (right shoulder) demonstrating the 3-o’clock positioning as the reference set to 0°. Any angle superior to this was a positive angle, and any angle below this was considered a negative value. The absolute value for the anchor location was the angle difference between the reference point and the insertion of the specific anchor.
Anchor Trajectory
To measure the anchor trajectory, the 3D model built in ImageJ was imported into SolidWorks CAD software (Dassault Systèmes SE). The insertion angle was defined as the angle between the axis of the anchor and the glenoid face. First, a line was drawn along the axis of each anchor, the “anchor axis,” which is illustrated in Figure 2. A second line was then drawn tangent to the glenoid face passing through the anchor axis and through the center of the glenoid clockface. This line was termed the “tangent line.” The angle between these 2 lines was defined as the “insertion angle” (Figure 2).

Diagram illustrating the anchor axis line and the tangent line, which is tangent to the glenoid face. The angle between these 2 lines is the insertion angle. Lower insertion angles indicate an anchor trajectory that is more parallel to the glenoid face. The insertion angle depicted is 74°.
Statistical Analysis
The anchor location angle and trajectory angle at all 3 locations, superior (3:30; −15°), middle (4:30; −45°), and inferior (5:30; −75°), were compared with descriptive statistics showing the mean and standard deviation. These were also analyzed using 1-sample t tests.
A 1-sample t test was used to allow for comparison against the actual target location, which minimized confounding effects of surgical technique given the small sample size. The absolute angle was used to calculate the means and standard deviations, and a 2-tailed t test was used to compare the LD and BC groups. In addition, the 95% confidence interval of the angle trajectory data was calculated. Statistical significance was determined using a P value of <.05 at a 95% confidence interval.
Results
The means and standard deviations of the anchor location and anchor trajectory are shown in Tables 2 and 3, respectively.
Descriptive Statistics of Anchor Location a
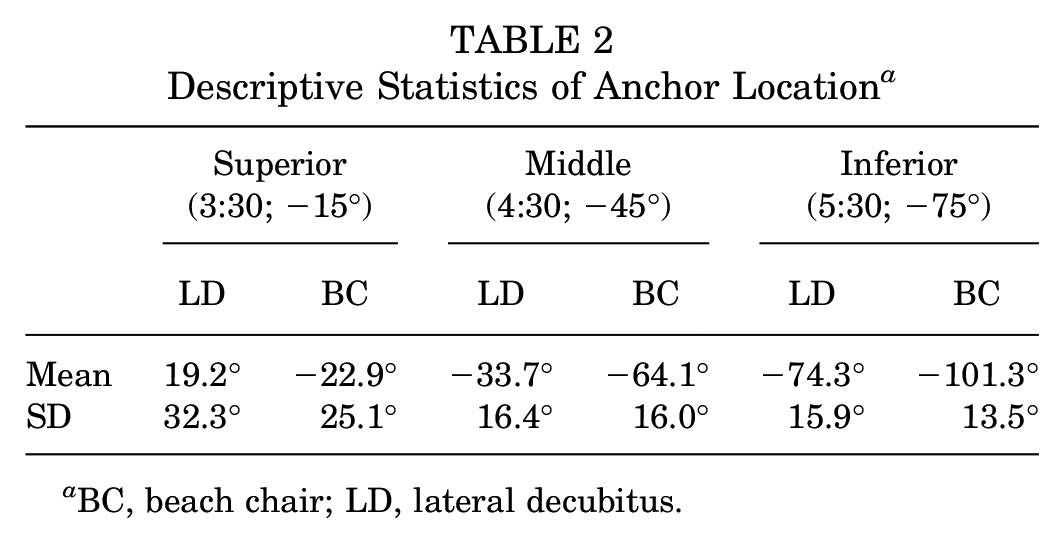
BC, beach chair; LD, lateral decubitus.
Descriptive Statistics of the Insertion Angle a

BC, beach chair; LD, lateral decubitus.
Overall Anchor Location
The location of the anchors was represented by deviance from the target location as described above. The LD overall deviance from the target angles was statistically significant (P = .000156; 95% CI, 8.85°-24.2°). For the BC position, the overall deviance from the target location was also statistically significant (P = .00142; 95% CI, 19.7°-2.4°).
Superior Anchor Location
For the LD superior anchor position (3:30 position), the mean anchor location deviated significantly from the target location of −15° (P = .00914; 95% CI, −6.0° to 31.4°). For the BC superior anchor position (3:30), the mean anchor location did not significantly deviate from the target angle (P = .732; 95% CI, −37.9° to 1.8°).
Middle Anchor Location
For the LD middle anchor position (4:30 position), the mean anchor location deviated significantly from the target location of −45° (P = .0129; 95% CI, −40.7° to −18.2°). The mean middle anchor location also deviated significantly from the target location in the BC position (P = .045; 95% CI, −74.4° to −45.4°).
Inferior Anchor Location
For the LD inferior anchor position (5:30 position), the mean anchor location did not significantly deviate from the target location of −75° (P = .178; 95% CI, −78.6° to −58.5°). For the BC inferior anchor position (5:30 position), the mean anchor location did significantly deviate from the target location (P = .0304; 95% CI, −106.0° to −77.2°).
Overall Anchor Location Trend
Using a Welch 2-sample t test, we found statistically significant evidence to suggest that the true population mean difference in anchor angle deviance between LD and BC was not 0° (P = .0000103). With the 95% confidence interval, the true mean difference in anchor angle deviance was between 16.3° and 38.9°. Practically, this means that LD angles tended to be superior to the target location and BC tended to be inferior to the target location.
Overall Anchor Insertion Angle
The mean insertion angles for each anchor position, with respect to technique, are summarized below in Table 3. The mean insertion angles for the superior anchor were 70.6° and 83.0° for the LD and BC techniques, respectively. For the middle anchor, the mean insertion angles were 86.1° and 88.9° for the LD and BC positions, respectively. The mean insertion angles for the inferior anchor were 93.1° and 106.3° for the LD and BC positions, respectively.
Overall Anchor Insertion Angle Trend
The mean insertion angle tended to increase for both surgical positions from superior to inferior anchor placement. Notably, the insertion angles for both techniques at the 5:30 position were >90°. The insertion angle for the inferior anchor in the LD position was 93.1° and 106.3° in the BC position. Based on glenoid morphology, this suggests that cortical rim perforation is more likely to occur during inferior anchor placement, in both positions, compared with other anchors. The mean insertion anchors for each anchor with the respective 95% confidence intervals are summarized in Figure 3.

Graph representation of the anchor insertion angles and their respective 95% confidence intervals for each anchor location. BC, beach chair; LD, lateral decubitus.
Discussion
When treating anterior shoulder instability, achieving proper inferior anchor placement (5:30 to 6-o’clock positions, right shoulder) is critical for the surgeon to obtain. This anchor placement allows the treating surgeon to anchor the inferior portion of the labrum and inferior glenohumeral ligament, thus stabilizing the inferior component of capsulolabal complex. The most important finding of the current study is that when placing the inferior-most anchor (5:30 position, right shoulder), accuracy may be improved with the patient in the LD position compared with the BC position. Conversely, in the BC position, this study suggests that accuracy of superior anchor placement is improved compared with anchor placement in the LD position. This study also supports that the anchor trajectory insertion angle is more advantageous in the LD positioning for inferiorly placed anchors.
Anchor placement in the current study significantly deviated from the target location, with anchor angle deviance between 16.3° and 38.9°, signifying that the surgeons involved in this study were not able to accurately locate the intended position on the clockface. Similarly, Jong et al 8 looked at surgeons’ perceived glenoid anchor location on the clockface from the posterior portal in BC and LD as well as the anterior superior portal in LD. After randomly placing anchors and later dissecting to find the exact anatomic position, they filmed the glenoid and anchors from the described portals and asked fellowship-trained surgeons to describe the location of the anchors in each video using the clockface technique. Jong et al 8 found that the overall accuracy of identifying exact anchor location was low at 34.0%, but when tolerances moved up by half-hour increments, 0.5, 1.0, and 1.5 hours away, the accuracy went up to 82.4%, 95.4%, and 98.0%, respectively. They also found that the most accurate view was the posterior BC position with a 30° scope compared with the posterior LD position (P = .029). The study by Jong et al 8 looked at the perceived location of anchors placed by others, while our study relies on the surgeon to use anatomic landmarks for accurate placement. This discrepancy in the findings may also be explained in the finding by Jong et al 8 that more experienced surgeons were less accurate in their anchor description, which they felt may be due to the experienced surgeons’ portal location preferences and customary views of the glenoid, which may have differed from the video views provided, leading to a less accurate anchor description.
The findings of this study highlight anchor placement variability from surgeon to surgeon. This brings into question the overall effect of anchor location/accuracy on obtaining a satisfactory outcome. To our knowledge, the concept of “minimally significant variable anchor location,” or rather, the minimal deviance from the desired anchor location that has a significant effect on functional outcomes, has not been investigated. However, it is likely that anchor location variability does have at least some effect on functional outcomes, particularly with the regard to the inferior-most anchor. A 2014 biomechanical study by Frank et al 4 described the importance of the anchor location, particularly the inferior-most anchor location, as a critical component to restore the sling effect of the capsule and stabilize the humeral head on the glenoid. This study suggests the ability to achieve more accurate inferior glenoid anchor placement in the LD compared with the BC position. Conversely, the middle and superior anchors were more accurately placed in the BC position. The authors of this study attributed the improved accuracy of the inferior anchor in the LD position to multiple factors, including traction, which facilitates increased glenohumeral space and improved surgeon ergonomics.
Regardless of position, the anchor insertion angles increased from superior to inferior in the current study. Liu et al 13 determined that an insertion angle <100° was an absolute safe zone for inferior anchor insertion that ensured no cortical perforation. The mean anchor insertion angles for inferior anchor placement in the BC and LD positions in the current study were 106.3° and 93.1°, respectively. These values suggest that the BC position is more likely to result in a perforated inferior anchor and that a more desirable insertion angle, and thus improved biomechanical performance, may be more easily achieved in the LD position.
With the limited clinical evidence in the literature supporting either BC or LD positioning, surgeon preference and experience has been the basis for selecting patient positioning. Both the BC and LD techniques are widely used for treating shoulder instability, and both have demonstrated similar rates of complications. It is important to point out that many complications are unique to each respective technique. Complications such as cerebral hypotension, infarction, cutaneous facial nerve neuropraxia, hypoglossal nerve injury, difficult airway management, and blindness are all rare but uniquely seen only in BC positioning. 12 Each position has known advantages and disadvantages that the treating surgeon must take into consideration to achieve the best outcomes for each patient.5,12 With the LD position, advantages include ease of traction, which increases the working glenohumeral space and optimizes inferior capsulolabral visualization. Additionally, LD facilitates improved cerebral perfusion. 12 With the BC position, advantages include more anatomic viewing (upright glenoid), more facile examination under anesthesia, and easier conversion to an open procedure, if necessary. Disadvantages of the BC position include increased risk of cerebral hypotension and difficulties visualizing the inferior aspect of the capsule and labrum, as well potential peripheral nerve palsies (ie, lateral femoral cutaneous nerve). Similarly, traction-related nerve palsies have also been associated with the LD position as well as brachial plexus injuries. 12 Additionally, LD can pose a greater challenge for anesthesia airway management and has also been linked to a higher number of postoperative thromboembolic events compared with BC, although the overall rate of thromboembolic events in either position is exceedingly low.10,12 In a 2014 systematic review conducted by Frank and colleagues, 5 an evaluation of 64 studies (38 BC position, 26 LD position) including 3668 shoulders (2211 BC, 1457 LD) was performed. Their inclusion criteria consisted of 2-year minimum follow-up and, on average, had >38 months of follow-up between the 2 groups (49.8 ± 29.5 months for BC compared with 38.7 ± 23.3 months for LD). The biggest finding from this review was that recurrent instability rates were significantly lower in the LD group (8.5% ± 7.1%) versus the BC group (14.65% ± 8.4%; P = .002). 5 This initial study was the first to suggest that patient positioning potentially impacted clinical outcomes after anterior shoulder instability surgery. Conversely, in a 2019 systematic review assessing outcomes of posterior instability repair in the BC versus LD positions conducted by Moeller et al, 15 the authors found no meaningful clinical or statistically relevant differences between the groups. Moreover, in a separate study published in 2021, the military group from Walter Reed and the US Naval Academy evaluated 614 patients undergoing arthroscopic Bankart repair in BC versus LD positions. 1 Recurrent instability was observed in 15.6% (24/154) of the LD patients and 15.8% (77/487) of the BC patients. There was no statistical difference in recurrent instability between groups. Notably, after adjusting for confounders, their regression analysis found no association between surgical position and recurrent instability (P = .85).
More recently, in a 2021 cross-sectional study from Baron et al 2 and the MOON Shoulder Group, 714 patients undergoing arthroscopic labral repair in the BC (406 shoulders) versus LD (308 shoulders) positions were evaluated. They found that surgeons utilizing the LD position tended to report on average a 7% greater labral tear size compared with the BC group (123.5°± 49° for BC vs 132.3°± 44° for LD; P = .012). In addition, they also found that the LD position was associated with more anchors placed at the 6-o’clock position and inferior glenoid (22.4% for BC vs 51.6% for LD; P < .001). Lastly, it was also concluded that the LD position was more frequently associated with ≥4 total anchors used for repair, as compared with the BC group (33.5% for BC vs 46.1% for LD; P < .001). 2 It remains unclear if it is technically easier to place anchors lower on the glenoid based on patient position, but perhaps, given the increased accuracy noted of the lower anchor placement in the present study, this could be extrapolated. Additional research is warranted in this area.
Limitations
This study has several limitations that should be noted when interpreting the results. First, this is a cadaveric study with an ex vivo model where iatrogenic labral tears were created. These tears may not represent the same tear patterns and soft tissue injury seen with true anterior shoulder instability. This could potentially lead to different visualization and anatomic cues to position on the glenoid face.
It is important to discuss that this study was conducted by 2 surgeons performing the procedure in BC and LD positions, respectively, which poses potential technical bias between operators. It is possible that the 2 surgeons could have differed in their perception of the 3:30, 4:30, and 5:30 positions. Notably, by performing a single-tailed t test and using a statistical model to compare population “ideals,” the authors believe that technical bias between 2 surgeons was mitigated. However, the amount of excessive traction put on the shoulder, particularly in the BC position (but arguably in both positions), may not be representative of what is actually feasible in real-life operating room environments and certainly makes these laboratory results difficult to extrapolate to the clinical setting. The data and anchor location were interpreted by a single reviewer (T.B.), which limits our ability to discuss the interobserver reliability with our study design and ability to generalize to all data sets. While we used 3:30, 4:30, and 5:30 clockface positions as our target anchor location, we recognize these may not be the ideal anchor locations (or the ideal number of anchors) for all patients with anterior shoulder instability. Individualized anchor locations, as well as number of anchors, for each patient may be needed to repair the chondrolabral junction and appropriately tension the capsule and glenohumeral ligaments. Additionally, anterior cortical perforation was not investigated in this study. Finally, portal placement, particularly transsubscapularis versus low anterior, for insertion of the inferior anchor has been associated with significantly different insertion angles, which may also potentially affect optimal anchor positioning. 3 A standardized low midanterior accessory portal was utilized in this study, and comparison of alternative portal positioning was not performed. While we were able to evaluate the patient position effect on the location and accuracy of specific anchors placed on the anterior glenoid face with standardized portals, additional clinical studies with larger sample sizes are needed to validate our findings.
Conclusion
Arthroscopic shoulder stabilization can be completed safely and effectively with positioning the patient in either the BC or LD position. While the debate on the advantages and disadvantages on patient positioning continues, this study noted that the patient position does influence the accuracy of not only the inferior anchors but also the middle and superior anchors in a standard 3-anchor anterior labrum repair. The LD position may offer improved inferior anchor placement, and the BC position may offer improved superior anchor placement. Further prospective and randomized trials are needed to best determine the clinical correlation of patient positioning on anchor placement, recurrent instability, and overall clinical outcomes.
Footnotes
Final revision submitted July 31, 2024; accepted August 28, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.D.J. has received education payments from Evolution Surgical, Gemini Mountain Medical, and Smith & Nephew. A.L. has received education payments from Gemini Mountain Medical and hospitality payments from Stryker. J.T.B. has received consulting fees from Encore Medical and Smith & Nephew, nonconsulting fees from Smith & Nephew, and education payments from Smith & Nephew. E.C.M. has received consulting fees from DePuy Synthes Products, Zimmer Biomet Holdings, Medical Device Business Services, Pacira Therapeutics, and Flexion Therapeutics; nonconsulting fees from Synthes GmbH; royalties from Zimmer Biomet Holdings; and education payments from Gemini Mountain Medical. A.S. has received consulting fees from Encore Medical and Medacta USA and honoraria from Encore Medical. R.M.F. has received nonconsulting fees from Arthrex, Bodycad USA, and Synthes GmbH; consulting fees from Arthrex; education payments from Gemini Mountain Medical, Arthrex, and Pinnacle; and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.