
Abstract
Background:
Surgical positioning can affect both perioperative and postoperative complication rates. It is unclear whether beach-chair versus lateral decubitus positioning affects outcomes in patients undergoing arthroscopic anterior shoulder stabilization surgery.
Purpose:
The purpose of this study was to compare recurrent instability, complications, and patient-reported outcomes between patients who underwent arthroscopic anterior shoulder stabilization in the beach-chair versus the lateral decubitus positions. It was hypothesized that recurrent instability, complications, and patient-reported outcomes would not be affected by surgical positioning.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The authors reviewed the medical records of patients who underwent shoulder stabilization (Current Procedural Terminology codes 29806 and 29807) from 2015 to 2019. Patients were included only if anterior instability was confirmed, arthroscopic surgery was performed in response to shoulder instability, and a minimum of 2 years of follow-up data were available. Data collected for eligible patients included perioperative and postoperative complications, recurrent instability, reoperation, and revision. Patients also completed surveys for the American Shoulder and Elbow Surgeons (ASES) score, Single Assessment Numeric Evaluation (SANE) score, Oxford Shoulder Instability (OSI) score, and a return to any level of sport (RTS) questionnaire.
Results:
Overall, 294 patients (162 lateral decubitus and 132 beach-chair positions) were included, with an average follow-up of 2.4 ± 1.6 years. There were no significant differences in demographics between groups, nor were there differences in the rates of postoperative dislocations, subjective instability, reoperations, revisions, or complications. There was a trend toward a higher revision rate in the beach-chair group (beach-chair, 6.1% vs lateral decubitus, 1.9%; P = .069). There was no significant difference between groups regarding RTS rates or postoperative ASES, SANE, and OSI scores at 3.3 ± 1.1 years postoperatively.
Conclusion:
Surgical positioning for arthroscopic anterior shoulder stabilization did not significantly affect recurrent instability, complications, and patient-reported outcomes. Both beach-chair and lateral decubitus positioning provided good outcomes for anterior shoulder stabilization, with an overall recurrent dislocation rate of 7.8% at a mean of 3.3 years after surgery.
The rate of shoulder dislocations is approximately 23 to 24 dislocations per 100,000 person-years, with anterior shoulder instability significantly more common than posterior shoulder instability. 7,8,17 Patients who sustain an initial anterior shoulder dislocation, as a general average, have a 39% chance of developing recurrent instability. The odds are 13 times greater for patients younger than 40 years and 3 times greater for men. 13 Arthroscopic shoulder stabilization has been shown to effectively treat anterior shoulder instability, decreasing recurrence rates to between 10% and 17%. 5,16 However, significant risk factors such as younger patient age, participation in competitive sports, off-track Hill-Sachs lesions, and glenoid bone loss increase the chances of recurrent instability after surgery. 16
Surgical positioning can affect perioperative and/or postoperative complication rates for many reasons, including proximity to nerves, issues with positioning, and surgical access. 11,14 The beach-chair and lateral decubitus positions are the 2 most common positions for shoulder arthroscopy, and each offers its own unique advantages and disadvantages for surgeons. 6,9,10,14,15 Beach-chair positioning allows for an easier transition to open surgery if necessary, has a quicker setup time, and also has a lower incidence rate of neuropathies, relative to lateral decubitus. 3,6 However, lateral decubitus positioning has a similar surgery duration, easier visualization of the labrum, and greater circumferential access to the joint. 3,6,10 A recent study found that patients who underwent Bankart repair arthroscopic anterior shoulder stabilization in the lateral decubitus position more frequently received ≥4 anchors and had more anchors placed in the inferior glenoid than patients in the beach-chair position. Despite these intraoperative differences, the type of surgical position is often selected according to each individual surgeon’s preference, with no clear superiority in postoperative outcomes between positions.
Several review articles have been published comparing the beach-chair and lateral decubitus positions for shoulder arthroscopy, 2,3,9,12,14,15 with 1 systematic review comparing these positions specifically for anterior shoulder stabilization surgery. 3 However, the data from that review come from pooling of noncomparative retrospective studies. No large retrospective cohort study has been published to compare recurrent instability, complications, and patient-reported outcomes between patients who undergo arthroscopic anterior shoulder stabilization in beach-chair versus lateral decubitus positioning.
The primary purpose of this study was to compare recurrent instability, complications, and patient-reported outcomes between patients who underwent arthroscopic anterior shoulder stabilization in the beach-chair versus the lateral decubitus positions. We hypothesized that recurrent instability, complications, and patient-reported outcomes would be similar between the 2 positions.
Methods
This study was exempt from institutional review board approval. We reviewed a list of patients aged 18 to 55 years who underwent arthroscopic shoulder stabilization (Current Procedural Terminology codes 29806 and 29807) from 2015 to 2019 at a single multicenter institution. Patients were included in the study if anterior instability was confirmed, arthroscopic surgery was performed in response to shoulder instability, and a minimum of 2 years of follow-up data were available. Patients were excluded for multidirectional instability, revision shoulder stabilization surgery, open surgery, significant glenohumeral osteoarthritis, concomitant rotator cuff repair, concomitant subacromial decompression, or isolated superior labral anterior-posterior (SLAP) repair. Patients with engaging Hill-Sachs lesions were indicated for concomitant remplissage and were also excluded from this study. Patients were excluded if surgery was not performed because of shoulder instability or if patient surgical positioning could not be confirmed.
Patient positioning was decided by the surgeon and was not randomized. Overall, 15 surgeons preferred to utilize the lateral decubitus position for all shoulder stabilization procedures, and 10 surgeons preferred the beach-chair position. All surgeons were fellowship trained in either shoulder and elbow or sport medicine. Routine venous thromboembolism prophylaxis was not provided to patients in this study cohort.
Data Collection
Patients were screened for eligibility while collecting pre- and perioperative data from the patient clinic notes and operative reports. Pre- and perioperative data collected included age, sex, body mass index, laterality of surgery, hand dominance, mechanism of injury, history of shoulder dislocation, concomitant procedures, number of anchors used, surgery duration (time from first incision to close), and perioperative complications.
Postoperative complications collected by screening postoperative patient encounters were subjective instability, shoulder dislocation, infection, nerve damage/injury, deep vein thrombosis/pulmonary embolism, significant shoulder pain and swelling, and reoperation/revision. Shoulder pain or swelling was considered a postoperative complication only if a subsequent arthroscopy or manipulation under anesthesia was performed. Revision was considered any shoulder stabilization reoperation, such as revision Bankart repair, capsulorrhaphy, or Latarjet procedure. Subjective instability was considered patient-reported apprehension, a subluxation event, or a dislocation event.
Patients were also contacted via REDCap (Vanderbilt University) to complete patient-reported outcome surveys, including postoperative complications and reoperations, the American Shoulder and Elbow Surgeons (ASES) score, Single Assessment Numeric Evaluation (SANE) score, Oxford Shoulder Instability (OSI) score, and a return to any level of sport (RTS) questionnaire. ASES and SANE scores range from 0 (poor) to 100 (healthy), while OSI scores range from 0 (poor) to 48 (healthy). No minimal clinically important differences are available for these scores regarding patients with anterior shoulder stabilization at a minimum 2-year follow-up. A general survey asking about postoperative complications and future ipsilateral shoulder surgery was also included to confirm the findings from postoperative encounter screening. Only patients who responded “yes” to the question, “Were you participating in a sport prior to your shoulder injury?” were included in the RTS analysis. These patients were subsequently asked, “Were you able to return to sport after surgery?” Possible answers were “yes, same/higher level”; “yes, lower level”; “no, not interested”; “no, could not return due to shoulder pain/instability”; “no, the opportunity was no longer available”; and “no, but returned to play a different sport.”
Statistical Analysis
Demographics, perioperative data, and postoperative outcomes were compared between patients who underwent surgery in beach-chair versus lateral decubitus positioning. Similar analyses were also performed comparing male versus female patients and younger (<25 years) versus older (≥25 years) patients. The age of 25 years was selected as a cutoff because age younger than 25 years is commonly clinically used as a risk factor for failed nonoperative treatment of shoulder instability, and this age cutoff provided sufficient sample sizes for both age groups in the current study. Mann-Whitney tests were used to calculate P values for nonparametric data. The chi-square or Fisher exact tests were used to calculate P values for categorical data. P values less than .05 were deemed significant. A multivariate regression analysis was performed with surgical position (beach-chair vs lateral decubitus), age, sex, number of anchors placed, and history of shoulder dislocations (acute vs chronic) as independent variables and recurrent instability as the dependent variable. All statistical analyses were done using RStudio (Version 3.6.3).
Results
There were 294 patients included in this study, 162 patients who underwent surgery in the lateral decubitus position and 132 in beach-chair position, with an average follow-up of 2.4 ± 1.6 years. Patients were on average 28.3 ± 9.4 years of age, and there were 227 (77.2%) men. Of the 294 patients, 215 (73%) had more than 2 years of clinical follow-up, and 175 (60%) patients completed surveys for the RTS questionnaire and ASES, SANE, and OSI scores at least 2 years postoperatively. There were no significant demographic differences between groups, and 2-year follow-up rates also did not differ (lateral decubitus, 72% vs beach-chair, 75%; P = .514) (Table 1).
Comparison of Preoperative Data Between Patients Who Underwent Shoulder Stabilization Surgery in the Beach-Chair Versus Lateral Decubitus Position a

a Categorical data are presented as No. (%), and continuous data are presented as mean ± SD. ASES, American Shoulder and Elbow Surgeons; BMI, body mass index; SANE, Single Assessment Numeric Evaluation.
Beach-chair positioning was associated with an increased number of anchors used (4.0 vs 3.3 for lateral decubitus; P = .001) (Table 2). All other perioperative variables, such as concomitant SLAP repair, surgery duration, and perioperative complications, were similar between groups. The only perioperative complication occurred in a 41-year-old man who underwent surgery in the lateral decubitus position. He experienced venous oozing during the removal of arthroscopic equipment from the anterior-inferior portal, and hemostasis occurred with electrocautery and placement of sutures.
Comparison of Perioperative Data Between Patients Who Underwent Shoulder Stabilization Surgery in the Beach-Chair Versus Lateral Decubitus Position a

a Categorical data are presented as No. (%), and continuous data are presented as mean ± SD. Boldface P value indicates a statistically significant difference between groups (P < .05). SLAP, superior labral anterior-posterior.
Postoperatively, no patients in either study cohort developed an infection or a venous thromboembolism. Beach-chair positioning had an increased revision rate but this trend was not significant (6.1% beach-chair vs 1.9% lateral decubitus position; P = .069) (Table 3). Rates of postoperative subjective instability, reoperations, revisions, neuropathy, and all complications also did not differ between groups (all P > .05). Overall, 23 (7.8%) included patients experienced a redislocation. In the lateral decubitus cohort, 3 of 12 patients who experienced a redislocation had experienced only 1 acute redislocation, while 5 patients had experienced several (2-5) redislocations and 4 patients had experienced frequent (≥6) redislocations. In the beach-chair cohort, 5 of 11 patients who experienced a redislocation had experienced only 1 acute redislocation, while 4 patients had experienced several (2-5) redislocations and 2 patients had experienced frequent (≥6) redislocations.
Revision shoulder stabilization procedures in the lateral decubitus cohort included 1 Latarjet procedure and 2 revision Bankart repairs, while revision procedures in the beach-chair cohort included 4 Latarjet procedures and 4 revision Bankart repairs. Further details about each patient who required a revision shoulder stabilization procedure are available in Appendix Table A1.
Comparison of Postoperative Outcomes Between Patients Who Underwent Shoulder Stabilization Surgery in the Beach-Chair Versus Lateral Decubitus Position a

a Categorical data are presented as No. (%), and continuous data are presented as mean ± SD. ASES, American Shoulder and Elbow Surgeons; OSI, Oxford Shoulder Instability; RTS, return to any level of sport; SANE, Single Assessment Numeric Evaluation.
There were no significant differences between groups regarding rates of returning to any level of sport as well as postoperative ASES, SANE, and OSI scores at an average of 3.3 ± 1.1 years of follow-up (all P > .05). RTS rates for contact athletes and overhead athletes also did not significantly differ between lateral decubitus and beach-chair positions.
Comparing 227 male and 67 female patients, all peri- and postoperative outcomes were similar except that men had an increased number of anchors placed (3.8 in men vs 3.3 in women; P = .039) (Appendix Tables A2 and A3). When comparing patients aged <25 versus ≥25 years, the younger patients had significantly shorter surgery durations (62.5 vs 72.4 minutes, respectively; P = .048) and higher rates of postoperative redislocations (12.8% vs 3.3%, respectively; P = .005), while all other peri- and postoperative outcomes were similar between age groups (Appendix Tables A4 and A5).
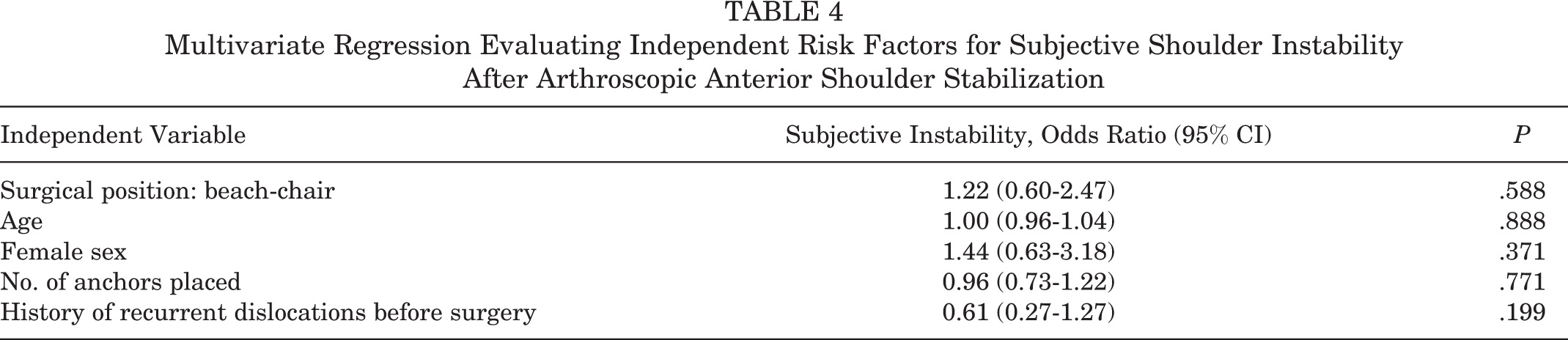
Multivariate regression analysis of surgical position, age, sex, number of anchors placed, and shoulder dislocation history showed that none of these variables were independently related to recurrent instability in the 48 included patients who developed recurrent anterior shoulder instability (Table 4).
Multivariate Regression Evaluating Independent Risk Factors for Subjective Shoulder Instability After Arthroscopic Anterior Shoulder Stabilization
Discussion
Our hypothesis was confirmed, as recurrent instability rates, complication rates, and patient-reported outcomes were similar between groups. Patients who underwent anterior shoulder stabilization in the beach-chair position had a trend toward increased revision rates compared with patients in the lateral decubitus position, but this difference did not reach statistical significance.
A large systematic review pooled the recurrence rates of 3668 patients with arthroscopic anterior shoulder instability from 64 studies. 3 They found that the lateral decubitus position provided a significantly lower recurrent instability rate for patients with anterior shoulder instability than the beach-chair position (8.5% vs 14.6%, respectively; P = .004). 3 However, no comparative studies were included in that systematic review, which significantly limited the strength of the conclusions drawn. In comparison, the present comparative study found no difference between beach-chair and lateral decubitus positions for redislocation and subjective instability rate. The previous systematic review may have found higher recurrence rates than the redislocation rates observed in the current study because the severity of recurrent instability could not be evaluated in the systematic review, so it is unclear whether the differences in recurrent instability observed were because of apprehension, subluxation, or Frank dislocation. 3 Whenever possible, subjective instability and redislocation should be evaluated in isolation, as recurrent instability as a whole may include a spectrum of instability from apprehension to dislocation. 3,4 The present comparative study provided an evaluation of redislocation rates separate from subjective instability to clarify the severity of postoperative instability. Evaluating redislocations and subjective instability separately showed that younger patients were more likely to redislocate their shoulder after surgery. However, the frequency of subjective instability did not differ between younger and older patients, and age was not an independent risk factor for subjective instability.
Lateral decubitus positioning is believed to allow better access to the glenohumeral joint, easier visualization of the labrum, and greater circumferential access to the joint. 3,6,10 This is supported by the findings of a recent cross-sectional study comparing the number and location of anchors used between beach-chair and lateral decubitus positions for arthroscopic anterior shoulder stabilization. 1 The authors found that anchors were placed in the 6-o’clock portion of the glenoid more than 2 times as frequently when patients were in the lateral decubitus position, and a larger number of anchors were placed with lateral decubitus positioning as well. 1 Despite the differences in anchor utilization, the current study found no differences in redislocation or subjective instability rates between beach-chair and lateral decubitus positions. However, beach-chair positioning was associated with a greater number of anchors placed than lateral decubitus in this cohort. Although our data set on number of anchors used is much smaller than the data presented by Baron et al, 1 the drastic difference in results shows that there may be significant surgeon bias when evaluating perioperative factors such as number and location of anchors. A randomized study design would be optimal to clarify perioperative differences between beach-chair and lateral decubitus positioning; however, surgeon preferences and total surgical volume within each position significantly limit the feasibility and validity of such a clinical trial.
This is the first comparative study to our knowledge to evaluate patient-reported outcomes between patients who underwent arthroscopic anterior shoulder stabilization in the beach-chair versus lateral decubitus position. The current study found no significant differences in ASES, SANE, or OSI scores between beach-chair and lateral decubitus positions. Similarly, Frank et al 3 performed a systematic review evaluating Rowe and Constant-Murley scores across 39 and 22 studies, respectively, and found that patient positioning did not affect these scores in patients with anterior shoulder stabilization. Overall, it appears that surgeons do not need to alter their preferred patient positioning for anterior shoulder stabilization, as patients can expect similar clinical and patient-reported outcomes whether undergoing surgery in the beach-chair or lateral decubitus position.
Limitations
There are several limitations to this study. First, this study was not randomized, and thus surgeon bias may have affected perioperative variables and postoperative outcomes. Second, the prevalence of significant Hill-Sachs and bony Bankart lesions, as well as the amount of glenoid or humeral head bone loss, was not evaluated. However, significant glenoid bone loss is often considered a contraindication for arthroscopic treatment of anterior shoulder instability, 4 and patients with 15% to 20% bone loss were excluded from arthroscopic stabilization surgery in our cohort. Third, the RTS and patient-reported outcome analyses were limited by a 60% patient follow-up rate; however, a large sample size of responses was still observed. Fourth, we provided various answer options evaluating why athletes did not RTS, which may have lowered our RTS rates relative to similar studies since patients may not have returned based on choice rather than because of their shoulder. Fifth, the postoperative outcomes in this study may have been affected by 79 (26.9%) patients being lost to 2-year follow-up and only 175 (60%) patients completing patient-reported outcome measures. Sixth, this study may have been underpowered to evaluate differences in recurrent instability. A post hoc power analysis was performed, finding that a sample of 28,480 patients (14,240 per group) would be required to detect a significant difference in redislocation rates, and a sample of 724 patients (362 per group) would be needed to observe a significant difference in revision rate. However, the limited number of patients with revisions (n = 11) may limit the validity of the post hoc power analysis findings. Seventh, we did not have data on preoperative sport participation for all included patients because of the nature of retrospective medical-record review, and thus did not include information or analyses on sport participation. Last, the location of anchor placement was not evaluated because of infrequent reporting and the lack of validity in self-reported anchor placement location from the operative report. The validity of anchor data in the operative reports may also have affected our assessment of the number of anchors used, which could explain why our findings are contrary to prior studies. 2 A prospective study design that confirms data collection on anchor placement would strengthen the present analysis.
Conclusion
Surgical positioning for arthroscopic anterior shoulder stabilization did not significantly affect recurrent instability, complications, and patient-reported outcomes. Both beach-chair and lateral decubitus positioning provided good outcomes for anterior shoulder stabilization, with an overall recurrent dislocation rate of 7.8% at a mean of 3.3 years after surgery.
Footnotes
Final revision submitted February 7, 2022; accepted February 25, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.B.F. has received education payments from Liberty Surgical, consulting fees from Medical Device Business Services, and speaking fees and honoraria from Vericel. B.J.E. has received research support from Arthrex, DePuy, Linvatec, Smith & Nephew, and Stryker; education payments from Arthrex, DePuy, and Smith & Nephew; and consulting fees from Arthrex. S.H. has received education payments from Liberty Surgical and hospitality payments from Arthrex and Smith & Nephew and has stock/stock options in Johnson & Johnson. M.E.B. has received grant payments from Arthrex, education payments from Arthrex and Smith & Nephew, and hospitality payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Thomas Jefferson University (study No. 21E.514).