
Abstract
Background:
Microfracture is the most common procedure for cartilage lesions during medial opening-wedge high tibial osteotomy (MOWHTO), but microdrilling has recently been introduced as an alternative technique.
Purpose:
To compare the clinical, radiologic, and arthroscopic outcomes of microfracture and microdrilling during MOWHTO.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 92 patients who underwent MOWHTO with either microfracture (n = 46) or microdrilling (n = 46), with a minimum follow-up of 24 months. Clinical outcomes included visual analog scale (VAS) for pain, Lysholm score, International Knee Document Committee (IKDC) subjective score, Western Ontario and McMaster Universities index (WOMAC), and objective IKDC grade. Medial femoral condyle (MFC) cartilage repair status was evaluated at 12 months postoperatively using the MOCART (magnetic resonance observation of cartilage repair tissue) 2.0 and the International Cartilage Regeneration & Joint Preservation Society (ICRS) Cartilage Repair Assessment (CRA) grade.
Results:
At 6 months postoperatively, the microdrilling group exhibited higher minimal clinically important difference achievement rates than the microfracture group for VAS pain (63.1% vs 41.3%; P = .04), Lysholm (61.2% vs 41.3%; P = .02), and IKDC subjective score (78.3% vs 45.7%; P = .001). At 12 months postoperatively, the microdrilling group exhibited significantly better VAS pain (33.7 ± 17.6 vs 25.7 ± 18.1; P = .03), Lysholm (57.8 ± 12.2 vs 67.9 ± 21.4; P = .007), and IKDC subjective score (52.9 ± 13.5 vs 61.9 ± 10.4; P = .001) compared with the microfracture group, but this difference was not observed at 24 months. WOMAC scores were superior in the microdrilling group at 6 months (32.1 ± 16.7 vs 48.4 ± 16.2; P = .004), 12 months (25.4 ± 15.4 vs 38.1 ± 17.0; P = .03), and 24 months (21.4 ± 13.9 vs 37.3 ± 14.6; P = .02). MFC cartilage repair status was superior in the microdrilling versus microfracture group (ICRS CRA grade, 8.2 ± 2.2 vs 6.7 ± 2.1 [P = .005]; MOCART 2.0 score, 56.3 ± 12.8 vs 49.7 ± 8.9 [P = .02]). At 24 months postoperatively, the microdrilling group had a higher proportion of IKDC A or B grades (84.8% vs 50.0%; P = .001).
Conclusion:
Combining MOWHTO with microdrilling for MFC defects resulted in earlier clinical recovery and superior functional outcomes over 24 months postoperatively compared with microfracture and demonstrated excellent cartilage repair on postoperative evaluation.
Articular cartilage lesions in the knee pose an unresolved clinical challenge. The avascular nature of articular cartilage limits its inherent regenerative capacity, resulting in poor regenerative cell recruitment at the time of injury and contributing to cartilage defect.11,31 This impaired regenerative capacity is strongly associated with cartilage degeneration and progression to osteoarthritis. Extensive research has been conducted to address full-thickness cartilage lesions.4,5,36,44
Microfracture, a procedure introduced by Steadman 46 in 1997, has become the standard procedure for treating articular cartilage lesions. It involves the creation of small holes in the subchondral bone to release marrow elements, leading to the formation of a fibrocartilage layer. Microfracture is valued for its simplicity, relatively short operative time, cost-effectiveness, and efficacy in managing degenerative joint lesions.24,28,47 Combining medial opening-wedge high tibial osteotomy (MOWHTO) with microfracture is a viable approach in cases of varus malalignment with medial articular cartilage defects, demonstrating positive outcomes in pain reduction and overall clinical improvement in several studies.42,49,50 Despite its benefits, microfracture has been associated with bone brittleness, subchondral cyst formation, and subchondral plate disruption. Long-term animal and human studies have highlighted the susceptibility of the perforation site to damage.2,18,35,40
In recent literature, highly advanced cartilage degeneration in the medial compartment has been mentioned as a risk factor for the survival rate of MOWHTO, and it has been reported that cartilage status, rather than simple chronological age, has a significant impact on patient clinical outcome.17,45 In addition, MOWHTO is increasingly performed due to the aging of the population and the desire to preserve the native knee joint, and the need to combine MOWHTO with an effective cartilage procedure in older age is being considered. The classic microdrilling technique posed more problems due to thermal necrosis of the bone compared with microfracture. However, the recently introduced microdrilling technique uses a smaller diameter drill to create deeper and more numerous holes. Continuous cooled irrigation minimizes thermal necrosis of the adjacent bone, while forming more marrow channels. Preclinical studies have shown this method to produce higher quality and quantity of repaired cartilage.7,22,43
Postoperative evaluation of structural outcomes following cartilage repair procedures involves magnetic resonance imaging (MRI) and arthroscopy. MRI is recognized as the preferred method for assessing postoperative cartilage morphology, boasting a sensitivity of 80% and specificity of 82% in determining the quality of cartilage repair tissue. 41 Additionally, arthroscopic evaluation, which assesses the macroscopic appearance and biomechanical properties of the repair site, serves as an accurate criterion for postoperative assessment.3,20,34
To date, few studies have retrospectively evaluated the effectiveness of microdrilling or microfracture as distinct modalities for managing medial femoral condyle (MFC) cartilage defects in patients undergoing MOWHTO. Furthermore, research on direct comparison of microdrilling and other cartilage procedures is limited. Therefore, our study aimed to compare the clinical, radiologic, and arthroscopic outcomes of microfracture and microdrilling techniques for treating MFC defects in patients undergoing MOWHTO. Our hypotheses were that (1) there would be no significant differences in the clinical outcomes at 6, 12, and 24 months postoperatively between the 2 groups and (2) there would be no significant differences in the MRI findings or arthroscopic cartilage repair status at 12 months postoperatively between the 2 groups.
Methods
Patient Selection
After receiving approval for the study protocol from our institutional review board, we conducted a retrospective review of patient data from individuals who underwent MOWHTO combined with a cartilage procedure performed by a single orthopaedic surgeon (S.-H.K.) at a single institution between September 2010 and May 2021. Indications for MOWHTO were as follows: (1) relatively young and active patients (<65 years old) with medial knee pain refractory to nonoperative treatment for ≥3 months, (2) medial compartment osteoarthritis accompanied by varus deformity (hip-knee-ankle angle >5°), and (3) a relatively good range of motion (motion arc >100° and flexion contracture <15°) without joint instability. Indications for combined marrow stimulation procedure (microfracture or microdrilling) were (1) presence of near full-thickness MFC cartilage defect (International Cartilage Regeneration & Joint Preservation Society [ICRS] grade ≥3B), (2) presence of focal and contained defect suitable for cartilage regeneration, and (3) patient preference for undergoing combined cartilage repair procedures, even if diffuse chondral lesions were present. The microdrilling procedure has been performed since April 2019, when we recognized the need for an advanced bone marrow stimulation technique and decided to apply it clinically. 43
The study inclusion criteria were as follows: (1) ≥24 months of clinical follow-up after MOWHTO with cartilage surgery using either microfracture or microdrilling in MFC defects, (2) MRI follow-up at 12 months postoperatively, and (3) second-look arthroscopic assessment at 12 months postoperatively. The exclusion criteria were as follows: (1) patients with incomplete preoperative or postoperative clinical data, (2) patients who underwent concomitant augmented or cell-based cartilage procedures (autologous chondrocyte implantation and autologous matrix-induced chondrogenesis), and (3) patients who underwent concomitant bony procedures (lateral closing-wedge distal femoral osteotomy).
Out of an initial 282 patients, 143 patients underwent MOWHTO combined with bone marrow stimulation using either microfracture or microdrilling within the period specified. Ultimately, 113 patients were included in the study; these patients were divided into 2 groups: those who underwent microfracture (n = 67) and those who underwent microdrilling (n = 46). After applying a propensity score–matching algorithm considering age, sex, and body mass index (BMI), we selected 46 patients for each group (Figure 1).

Flowchart of patient inclusion and exclusion in this study. MOWHTO, medial opening-wedge high tibial osteotomy; MRI, magnetic resonance imaging.
Surgical Procedure and Rehabilitation
A single orthopaedic surgeon performed all surgeries. Preoperative planning using the Miniaci method 30 ensured proper lower extremity alignment. Diagnostic arthroscopy was conducted prior to the osteotomy to assess the articular cartilage status. Biplanar MOWHTO was performed, with additional microfracture or microdrilling on the MFC lesions. Microfracture followed established techniques, 48 involving debridement of the chondral defect, creation of a stable vertical shoulder, and removal of the calcified cartilage layer. Subsequently, subchondral perforations were made at 3- to 4-mm intervals using an arthroscopic awl (Arthrex) with a width of 2 to 3 mm and a depth of 5 to 8 mm.14,48 For microdrilling, similar cartilage defect preparation procedures were followed as in microfracture. However, drilling holes were created using a 1.5 mm–diameter drill bit (ECT Internal Fracture Fixation Drill Bits; Zimmer Biomet), spaced evenly 1 to 2 mm apart (slightly closer than microfracture holes) and extending 13 to 15 mm deep. Patients were recommended for plate removal if bony union was confirmed at 12 months postoperatively, combined with arthroscopic evaluation of cartilage repair.
Postoperatively, patients were instructed to restrict weightbearing using crutches and to limit range of motion with a hinged brace. The duration of these restrictions varied individually, typically lasting 6 to 8 weeks depending on factors such as the cartilage defect size and containment. 38 During the initial 2 weeks, patients were advised to perform toe-touch weightbearing and passive range-of-motion exercises using a continuous passive motion exercise machine. Passive range of motion was increased by 30° every 2 weeks. Patients progressed to partial (50%) weightbearing for the final 4 weeks of the weightbearing restriction period. After the 6- to 8-week restriction period, patients were instructed to discontinue using the hinged brace and crutches.
Data Collection
Baseline patient characteristics, including age, BMI, sex, and laterality, were collected. All patients had MFC defects, which were categorized based on size, with 4 cm2 serving as the threshold for large defects.8,13 The presence of kissing lesions and multiple lesions was noted. Preoperative alignment was assessed using radiographic parameters, including the hip-knee-ankle angle 15 and load-bearing axis deviation 15 on standing lower extremity images.
Outcome Measures
Comparative analyses of clinical outcomes, radiological measurements, and arthroscopic assessments were conducted between the microfracture and microdrilling groups. Patient-reported outcome measures (PROMs) included the visual analog scale (VAS) for pain, Lysholm knee score, International Knee Documentation Committee (IKDC) subjective score, and Western Ontario and McMaster Universities index (WOMAC), assessed preoperatively and at 6, 12, and 24 months postoperatively. Objective IKDC grades (A, normal; B, nearly normal; C, abnormal; and D, severely abnormal) were recorded at all time points.
A standardized, reproducible, semiquantitative approach for the morphological assessment of cartilage repair based on the MOCART (magnetic resonance observation of cartilage repair tissue) 2.0 knee score of the MFC was performed at 12 months postoperatively, involving 2 radiologists, each of whom measured the 7 variables of the MOCART 2.0 score 41 on MRI; the mean of the 2 total scores was used in the analysis. Subchondral bone was evaluated with 2 subscales of the MOCART 2.0 score: bony defect or bony overgrowth (maximum score, 10) and subchondral changes (maximum score, 20). Additionally, the presence of subchondral edema, subchondral cysts, intralesional osteophytes, and osteonecrosis was investigated.
Arthroscopic assessment was conducted at 12 months postoperatively with fixation plate removal. The status of the cartilage lesions was assessed by 2 orthopaedic surgeons (J.-S.P. and S.-H.J.) according to the ICRS Cartilage Repair Assessment (CRA) grading system, 20 and the mean of the 2 scores was used in the analysis.
Minimal Clinically Important Difference for PROMs
The minimal clinically important difference (MCID) signified the smallest change in a score deemed important to the patient. 16 We attempted to use MCID thresholds derived from microfracture-specific cohorts for relevant PROMs (MCID for IKDC subjective score = 6.3 points at 6 months1,12). If these values were unavailable, we prioritized the pre-established MCID values from previous studies and systematic reviews of cartilage repair surgery and applied them (MCID for VAS pain = 27 points, Lysholm = 10.2 points19,51) to evaluate the clinical outcomes.
Statistical Analysis
All statistical analyses were conducted using SPSS Version 26.0 (IBM Corp). Continuous variables were reported as means with standard deviations and were analyzed using the Student t test or Mann-Whitney U test. Categorical variables were reported as frequencies with percentages and were assessed using the Pearson chi-square test or Fisher exact test. Statistical significance was set at P < .05 for all tests. Comparison of the PROMs (VAS pain, Lysholm, IKDC subjective, and WOMAC scores) between the microfracture and microdrilling groups at 6, 12, and 24 months postoperatively was performed using the Student t test. The distribution of the IKDC objective grades was compared between the 2 groups using the Fisher exact test. To determine the MCID achievement rate for the IKDC subjective, VAS pain, and Lysholm scores, we applied the MCID thresholds from previous studies12,19,51 and compared them using the Pearson chi-square test. In addition, based on load-bearing axis deviation at 12 months postoperatively, each patient was categorized into undercorrected, acceptable, and overcorrected groups, with 62.5% ± 6.25% as the criterion for acceptable correction. A comparison between the microfracture and microdrilling groups of mean MOCART 2.0 score and ICRS CRA grade at 24 months postoperatively was conducted using the Student t test. Finally, a subgroup analysis of objective outcomes according to MFC defect size (≤4 vs >4 cm2) was conducted.
Results
Demographic Data
Baseline characteristics, including age, BMI, sex, and laterality, were comparable between the microfracture and microdrilling groups (P = .09-.82). There were also no significant differences in preoperative radiologic alignment parameters (P = .58-.67), cartilage defect location (P = .10-.98), MFC defect size (P = .74), or MFC defect size distribution (P = .65) (Table 1).
Patient Baseline Characteristics According to Study Group a
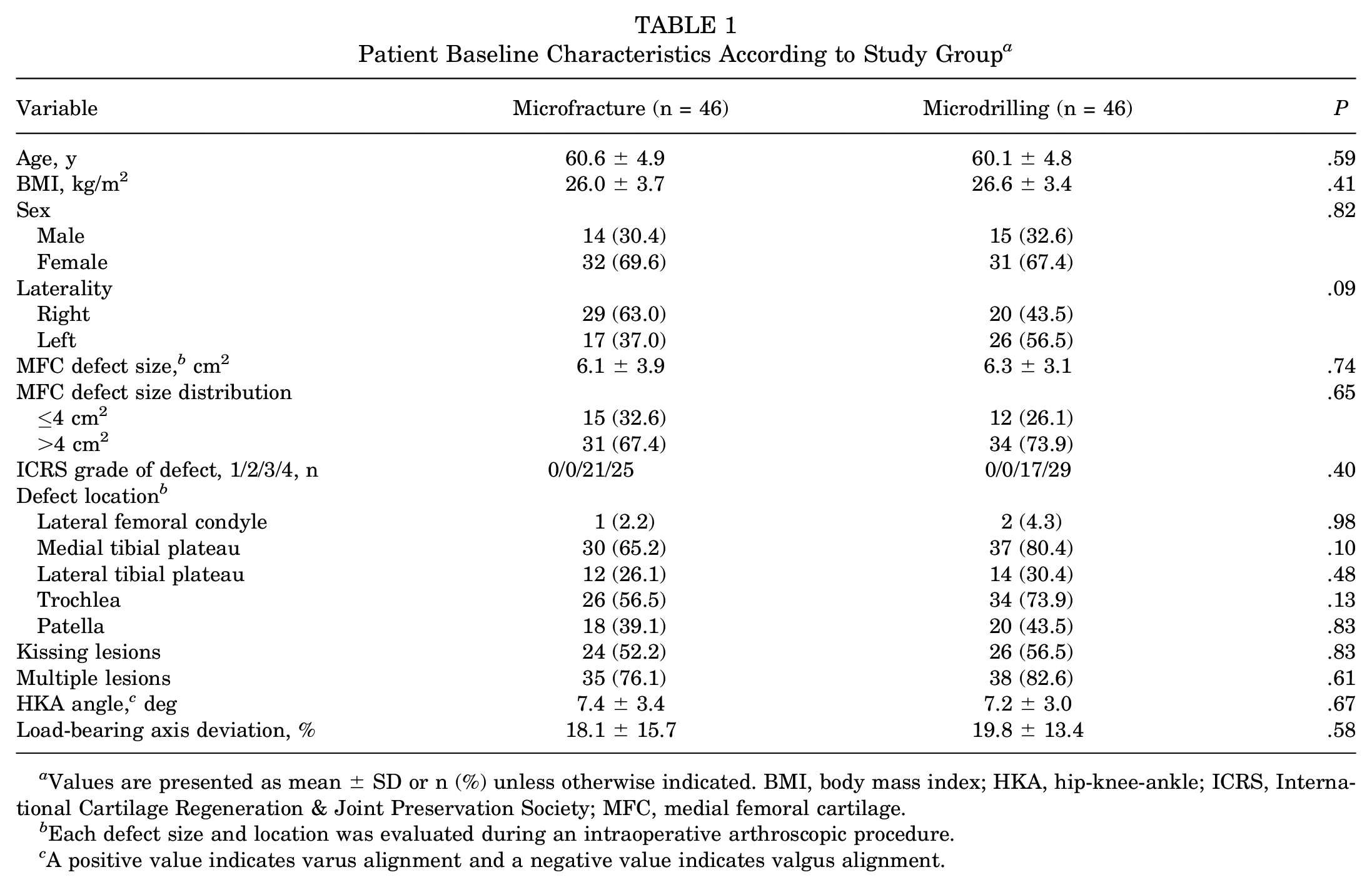
Values are presented as mean ± SD or n (%) unless otherwise indicated. BMI, body mass index; HKA, hip-knee-ankle; ICRS, International Cartilage Regeneration & Joint Preservation Society; MFC, medial femoral cartilage.
Each defect size and location was evaluated during an intraoperative arthroscopic procedure.
A positive value indicates varus alignment and a negative value indicates valgus alignment.
Clinical Outcomes
Preoperative VAS pain, Lysholm, and IKDC subjective scores were similar between the 2 groups (P = .79-.99) and all scores improved significantly from preoperatively to 6, 12, and 24 months postoperatively in both groups (P < .001). At the 12-month follow-up, the microdrilling group showed superior VAS pain, Lysholm, and IKDC subjective scores (P = .03, .007, and .001, respectively). However, no significant differences were observed at 24 months. WOMAC total scores were significantly superior in the microdrilling group at all time points (P = .004-.03) (Table 2).
Comparison of Patient-Reported Outcomes Between the Study Groups a

Values are presented as mean ± SD. Bolded P values indicate a statistically significant difference between the groups (P < .05). IKDC, International Knee Documentation Committee; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities index.
MCID Achievement Rate
At the 6-month postoperative follow-up, the microdrilling group had a significantly higher proportion of patients achieving the MCID on VAS (63.1% vs 41.3%; P = .04), Lysholm score (65.2% vs 41.3%; P = .02), and IKDC subjective score (78.3% vs 45.7%; P = .001). The MCID achievement rate for the Lysholm score remained higher in the microdrilling group at 12 months postoperatively (P = .03). No significant differences were observed between the 2 groups at 24 months postoperatively for VAS, Lysholm score, and IKDC subjective score (P = .21-.82) (Figure 2).

MCID achievement rates for the VAS pain, Lysholm, and IKDC subjective scores between the microfracture and microdrilling groups according to postoperative period. Statistically significant differences between the groups were observed at *postoperative 6 months for the VAS pain, Lysholm, and IKDC subjective scores and ***postoperative 12 months for the Lysholm score (P < .05). IKDC, International Knee Documentation Committee; MCID, minimal clinically important difference; MOWHTO, medial opening-wedge high tibial osteotomy; postop, postoperative; VAS, visual analog scale.
Objective Outcomes
Preoperative objective IKDC grade C or D rates did not significantly differ between the microdrilling (58.7%) and the microfracture (54.3%) groups. However, the microdrilling group exhibited a higher percentage of patients who achieved objective IKDC grade A or B at 12 months postoperatively (76.1% vs 52.2%; P = .03) and 24 months postoperatively (84.8% vs 50.0%; P = .001) (Table 3). In the arthroscopic assessment, the microdrilling group displayed significantly higher ICRS CRA scores than the microfracture group at 12 months postoperatively (8.1 ± 2.2 vs 6.9 ± 2.1; P = .01) (Figure 3). At 12 months postoperatively, there were no significant differences in postoperative radiographic alignment parameters and MOCART 2.0 scores between the 2 groups (P = .12-.59). However, in the subgroup analysis based on MFC defect size, the microdrilling group exhibited superior objective outcomes for large MFC defects (>4 cm2), with no differences in the alignment parameters due to MOWHTO between the 2 groups (Table 4).
Comparison of Objective IKDC Grade at Preoperative to Postoperative Follow-up a
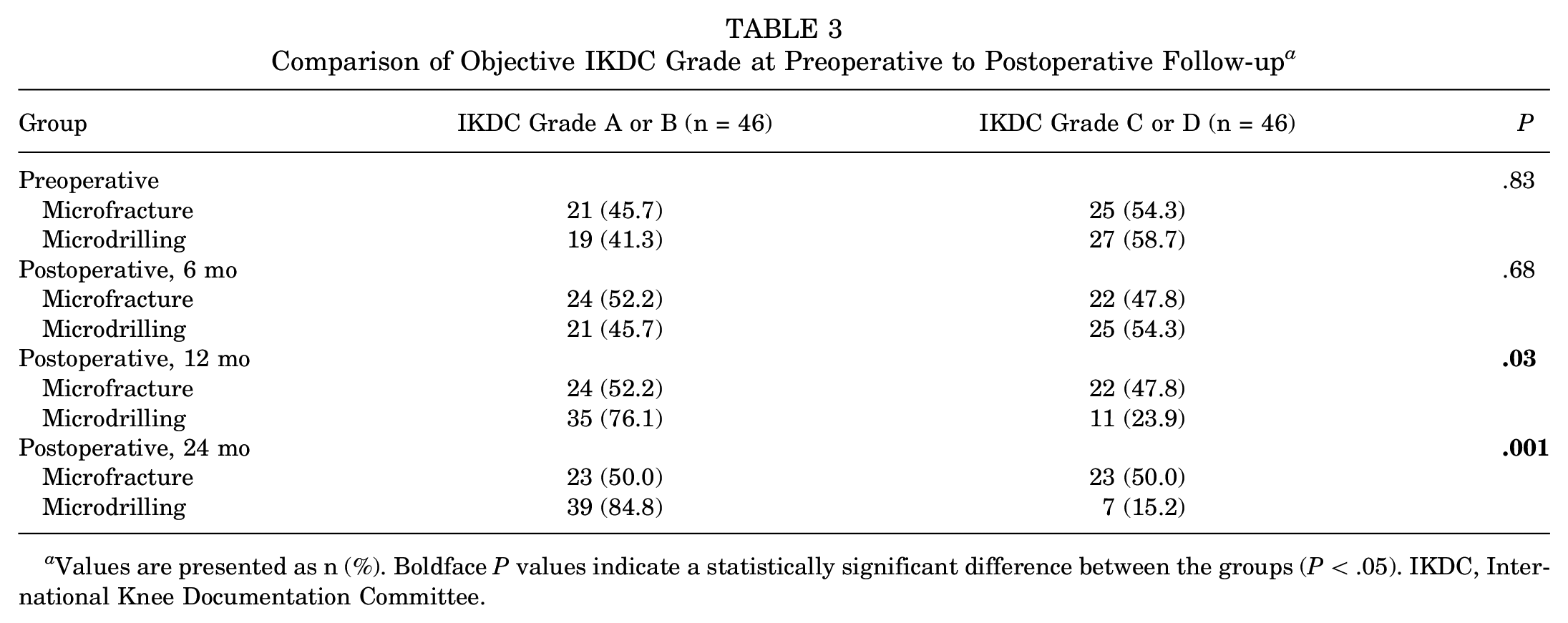
Values are presented as n (%). Boldface P values indicate a statistically significant difference between the groups (P < .05). IKDC, International Knee Documentation Committee.

ICRS CRA grade on arthroscopic assessment at 12 months postoperatively between the microfracture and microdrilling groups. *Statistically significant difference between groups (P < .05). CRA, Cartilage Repair Assessment; ICRS, International Cartilage Regeneration & Joint Preservation Society; MOWHTO, medial opening-wedge high tibial osteotomy.
Radiologic Assessment at Postoperative 12-Month Follow-up and Subgroup Analysis by MFC Defect Size at Last Follow-up a

Values are presented as mean ± SD or n (%) unless otherwise indicated. Last follow-up means that the IKDC objective grade is from postoperative 24-month follow-up and other variables are from postoperative 12-month follow-up. Boldface P values indicate a statistically significant difference between the groups (P < .05). CRA, Cartilage Repair Assessment; HKA, hip-knee-ankle; ICRS, International Cartilage Regeneration & Joint Preservation Society; IKDC, International Knee Documentation Committee; MFC, medial femoral cartilage; MOCART, magnetic resonance imaging of cartilage repair tissue.
Varus alignment is indicated by a positive value and valgus alignment by a negative value.
Depending on the load-bearing axis deviation, undercorrected means <56.25%, acceptable means 56.25% to 66.30%, and overcorrected means >66.30%.
No major complications associated with either MOWHTO or the combined cartilage procedure were observed. Subchondral edema was observed in the majority of the patients at the 1-year follow-up MRI (91.3% for both groups). Subchondral cyst formation and intralesional osteophytes were noted in a small number of cases in each group, with no significant differences observed between groups (subchondral cyst: microfracture, 8.7%; microdrilling, 6.5% [P = .69]; intralesional osteophyte: microfracture, 4.3%; microdrilling, 2.2% [P = .56]). No osteonecrosis was observed in either group. MOCART 2.0 subscales evaluating subchondral bone defects or bony overgrowth and subchondral changes showed no differences between the groups (bony defect or overgrowth: microfracture, 7.7 ± 2.5; microdrilling, 7.9 ± 2.7 [P = .73]; subchondral change: microfracture, 11.4 ± 4.2; microdrilling, 12.9 ± 3.2 [P = .07]).
Discussion
The primary finding of this study was the superiority of microdrilling over microfracture for treating MFC defects during MOWHTO according to several clinical outcomes from 6 to 24 months after surgery, including cartilage repair assessed through MRI and arthroscopic evaluation. The excellent objective outcomes of microdrilling in large MFC defects (>4 cm2) were particularly encouraging. This suggests that microdrilling may effectively address the limited indications for microfracture in large cartilage defects commonly encountered during MOWHTO procedures.
Clinically, the MCID scores play a vital role in establishing treatment thresholds via outcome measures. MCID represents the change in outcome scores that result in the smallest clinically noticeable improvement after surgery. 33 We were unable to calculate the MCID using the anchor method; therefore, we relied on previously established values from other studies.1,12,19,51 Comparison of the microfracture and microdrilling groups in terms of MCID achievement rates for the VAS pain, Lysholm, and IKDC subjective scores revealed a higher MCID achievement rate in the microdrilling group at the 6-month postoperative mark. This finding indicates that microdrilling has a more substantial impact on early postoperative satisfaction and symptom improvement. These results are consistent with the findings reported by Beletsky et al, 1 who conducted a retrospective comparison between microfracture and microdrilling in 34 patients and found a statistically significantly favorable MCID achievement rate in the IKDC subjective score, Knee injury and Osteoarthritis Outcome Score (KOOS) Pain subscale, and KOOS Sport and Recreation subscale in the microdrilling group compared with the microfracture group at 6 months postoperatively. They attributed these results to differences in bone channels reaching the medullary stroma, reduced bone compression, and the absence of osteonecrosis in the microdrilling group. 1
Microfracture is a widely utilized technique for cartilage repair due to its ease of execution and cost-effectiveness.28,39,47 To date, few studies have retrospectively evaluated the effectiveness of microdrilling or microfracture as distinct modalities for managing MFC defects in patients undergoing MOWHTO. 10 Several studies have noted the challenges associated with achieving adequate microfracture in degenerative chondral lesions, primarily due to the presence of osteosclerosis and the thin nature of the tissue around the defect perimeter, rendering it challenging to achieve an adequate effect.21,32,48 Moreover, several studies reporting on postoperative outcomes at 1 to 5 years after MOWHTO with microfracture have failed to demonstrate statistically significant clinical superiority compared with high tibial osteotomy alone.25,27,37
Several studies have explored microdrilling as a technique for managing cartilage defects, with the fundamental premise being that certain factors can enhance its efficacy. These factors include creating a vertical wall during defect preparation, increasing the depth of subchondral penetration, reducing the awl diameter, and augmenting the number of subchondral perforations. Such adjustments are believed to elevate the concentration of mesenchymal stem cells and promote the release of growth factors and chemotactic cytokines, thereby facilitating cartilage healing. 43 In recent publications, Chen et al6,7 proposed an alternative approach to prevent thermal osteonecrosis, a potential complication associated with traditional microdrilling. Their studies,6,7 conducted in rabbits, combined microdrilling with cooled irrigation and compared cartilage filling based on different drilling depths. Remarkably, they found that a 6-mm drilling depth resulted in significantly better cartilage filling when compared with a 2-mm drilling depth. Moreover, Min et al 29 conducted a study in rabbits to measure the number of mesenchymal stem cells and compare it with the total exposed area, which varied based on drill size and the number of holes. Their findings revealed that the number of mesenchymal stem cells increased as the total exposed area expanded. The microdrilling technique employed in our study, characterized by 1- to 2-mm spacing and a 13- to 15-mm depth using a 1.5-mm drill, aligns with these effective principles. By allowing deeper penetration compared with microfracture and increasing the exposed area, microdrilling likely enhances the concentration of mesenchymal stem cells. Yang et al 53 reported that at a mean follow-up of 5.3 years after MOWHTO, the final IKDC subjective score and WOMAC score of the “good status” group, assessed as ICRS CRA grade 1 or 2 at 1-year second-look arthroscopy, were significantly improved compared with the “bad status” group, assessed as ICRS CRA grade 3 or 4. These results support the superiority of microdrilling for cartilage repair of MFC at 12 months postoperatively on MRI and arthroscopy in our study, which may have important clinical and cost-effective significance in combination with MOWHTO.
A study by de Windt et al 9 demonstrated that patients with femoral condylar defects experienced significantly greater improvement with microfracture than those with defects in the tibia or patella after 36 months of observation. However, Kreuz et al 23 reported favorable results for tibiofemoral cartilage defects (<4 cm2) in patients <40 years of age from 18 to 36 months after surgery. In patients >40 years of age, the ICRS grade worsened between 18 and 36 months, regardless of the lesion site. Additionally, Weber et al 52 reported that in a midterm follow-up of microfracture over 5 years, 42.1% of patients underwent reoperation at a mean of 2.63 years, despite having a mean age of 35.87 years. Multivariate analysis identified a large defect size exceeding 3.6 cm2 as an independent risk factor for this reoperation rate. These findings highlight the limitations of microfracture as a cost-effective cartilage procedure for MOWHTO patients, who tend to be older and have larger cartilage defects on average. Recently developed microdrilling techniques have shown promise owing to their cost-effectiveness and their compatibility with single-stage MOWHTO procedures. However, literature directly comparing microdrilling with other cartilage procedures is limited. Our study is valuable in this context, as it demonstrates favorable clinical results for microdrilling in combination with MOWHTO through a comparative analysis with microfracture. It further underscores the efficacy of microdrilling, particularly in addressing large MFC defects (>4 cm2) found in most MOWHTO groups.
Limitations
This study has a few limitations that should be considered. First, its retrospective design introduced the possibility of measurement bias. Second, combined MOWHTO presents a significant limitation in directly comparing microfracture and microdrilling. Although there was no significant difference in postoperative alignment between the 2 groups, MOWHTO may affect clinical outcomes and cartilage repair, introducing the potential for unknown confounding factors that could influence outcomes. Third, we employed preestablished MCID values derived from microfracture-specific cohorts, including IKDC (6.3 points),1,12 VAS pain (27 points),19,51 and Lysholm (10.2 points),19,51 for the MCID threshold calculation of PROMs in the analysis of clinical outcomes and systematic reviews of cartilage repair surgery. Fourth, the patient assessments covered a 24-month clinical follow-up and a 12-month MRI and arthroscopic evaluation, limiting the generalization of short-term results and necessitating further research to investigate long-term effects. Finally, potential inaccuracies in measuring the MOCART 2.0 score via MRI and ICRS CRA grades during arthroscopy may arise owing to variations in MRI image quality and challenges associated with irregularities in the articular surface and unclear lesion margins. Additionally, we did not perform histological assessments, which are important for evaluating the durability and quality of the repaired tissue. 26 These limitations emphasize the importance of conducting more comprehensive prospective studies with extended follow-up periods and refined scoring methodologies to enhance our understanding of the effectiveness of the microdrilling technique.
Conclusion
Combining MOWHTO with microdrilling for MFC defects demonstrated superior clinical recovery and enhanced functional outcomes for up to 24 months postoperatively, surpassing the results achieved with microfracture procedures. Furthermore, the combined microdrilling approach exhibited improved cartilage repair outcomes on postoperative MRI and arthroscopic evaluations, even in cases involving large MFC defects.
Footnotes
Final revision submitted July 9, 2024; accepted July 25, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Gangnam Severance Hospital (ref No. 3-2023-0268).