
Abstract
Background:
The correlation between the Miniaci angle and presurgical hip-knee-ankle (HKA) angle, weightbearing line (WBL) percentage, and changes in the HKA angle (ΔHKA angle) and WBL percentage (ΔWBL percentage) is significant in opening-wedge high tibial osteotomy (OWHTO). The conversion formulas that interrelate the Miniaci angle with pre-HKA angle (formula 1), pre-WBL percentage (formula 2), ΔHKA angle (formula 3), and ΔWBL percentage (formula 4) have been derived through the linear regression analysis. However, the accuracy of conversion formulas has not been validated.
Purpose:
To validate the precision of conversion formulas targeting various surgical objectives for OWHTO planning in the varus knee patient population.
Study design:
Cross-sectional study; Level of evidence, 3.
Methods:
A retrospective study of 155 lower limbs of 112 patients with medial unicompartmental knee osteoarthritis was conducted. A computer simulation of OWHTO was performed to calculate the Miniaci angle by delivering the WBL to the Fujisawa point (group 1), at 65% WBL percentage (group 2), and 4.5° of valgus (group 3). Spearman correlation and Bland-Altman analyses were conducted between the computer simulation and formula calculation.
Results:
Upon evaluating the widely accepted Fujisawa point as a postoperative target, all formula results demonstrated a strong correlation with computer simulation outcomes (r = 0.962-0.999). Compared with the simulated Miniaci angle, the mean bias of the calculated angles derived from formulas 1 to 4 was 0.098° (formula 1), –0.268° (formula 2), 0.065° (formula 3), and −0.246° (formula 4). Notably, the formula based on the ΔHKA angle exhibited an ideal correlation with the simulated Miniaci angle (r = 0.998-0.999). In the 3 groups with varying postoperative targets, the mean bias of this formula in predicting the Miniaci angle was 0.065° (group 1), 0.070° (group 2), and 0.080° (group 3).
Conclusion:
Formulas based on the presurgical HKA angle and WBL percentage showed perfect accuracy for measuring the Miniaci angle targeting the Fujisawa point. The formula based on ΔHKA angle achieved the best accuracy and may be a valuable tool for measuring the Miniaci angle in broader surgical targets.
Keywords
The management of knee osteoarthritis (OA) is individualized based on patient factors, including age, body mass index, OA severity, ligament status, and lower limb alignment. Young individuals afflicted with knee OA maintain high functional aspirations and are invariably keen on regaining their vitality after surgery. 17 Opening-wedge high tibial osteotomy (OWHTO) is a classic surgical procedure for the treatment of early and midterm OA symptoms4,13 that aims to readjust normal force distribution by reducing the load on the cartilage and subchondral bone of the affected side. OWHTO has been shown to alleviate pain, improve knee joint function, slow the progression of knee joint degeneration, and potentially reduce the need for total knee arthroplasty.15,22 Achievement of the appropriate degree of correction of lower limb alignment determines the effect of OWHTO. This correction degree is commonly achieved through adjustment of parameters, including the hip-knee-ankle (HKA) angle and weightbearing line (WBL) percentage. 12
Successful OWHTO relies on accurate presurgical planning based on standing whole-leg radiography (WLR).8,19,20 A picture archiving and communication system is commonly used to measure presurgical parameters but cannot virtually perform computer simulations. Numerous surgeons now leverage commercial software to facilitate the surgical planning process. While the software enhances planning efficiency, it also incurs additional expenses. A previous study 12 found that the presurgical HKA angle, presurgical WBL percentage, and changes in the HKA angle (ΔHKA angle) and WBL percentage (ΔWBL percentage) were strongly correlated with the Miniaci angle in presurgical planning. They further found that conversion formulas based on presurgical parameters could accurately calculate the required correction angle. However, they only analyzed the data in which the planning target was the Fujisawa point, while others suggested targets within a valgus of 3° to 6° or a WBL percentage of 60% to 70%.7,19 Additionally, the conversion formulas were not externally validated, as the use of data obtained from different radiographic machines may cause unknown bias.
To address this knowledge gap, the present study further validated the capability and usable range of the conversion formulas through external validation. We collected a large number of patient WLRs using different radiographic machines. Computer simulations and conversion formula calculations were performed for comparison and analysis. We hypothesized that the conversion formulas would achieve perfect accuracy for radiographs from other devices.
Methods
This retrospective study was approved by our institutional review board. We retrospectively evaluated 112 patients who consented to participate. A total of 155 standing WLRs (Multitom Rax, Version VF10; Siemens Healthineers) were collected and analyzed between January and September 2022. The inclusion criteria were as follows: (1) adults, (2) isolated medial compartment osteoarthritis, Kellgren–Lawrence classification grade ≤3, (3) mechanical varus malalignment with an angle of correction of >5°, and (4) patella facing anteriorly in the bipedal standing position. The exclusion criteria were as follows: (1) history of fracture or orthopaedic surgery, (2) apparent deformities of the femur and tibia, (3) leg-length discrepancy, and (4) developmental dysplasia of the hip or femoral head necrosis. 21 The details of enrollment are shown in Figure 1.
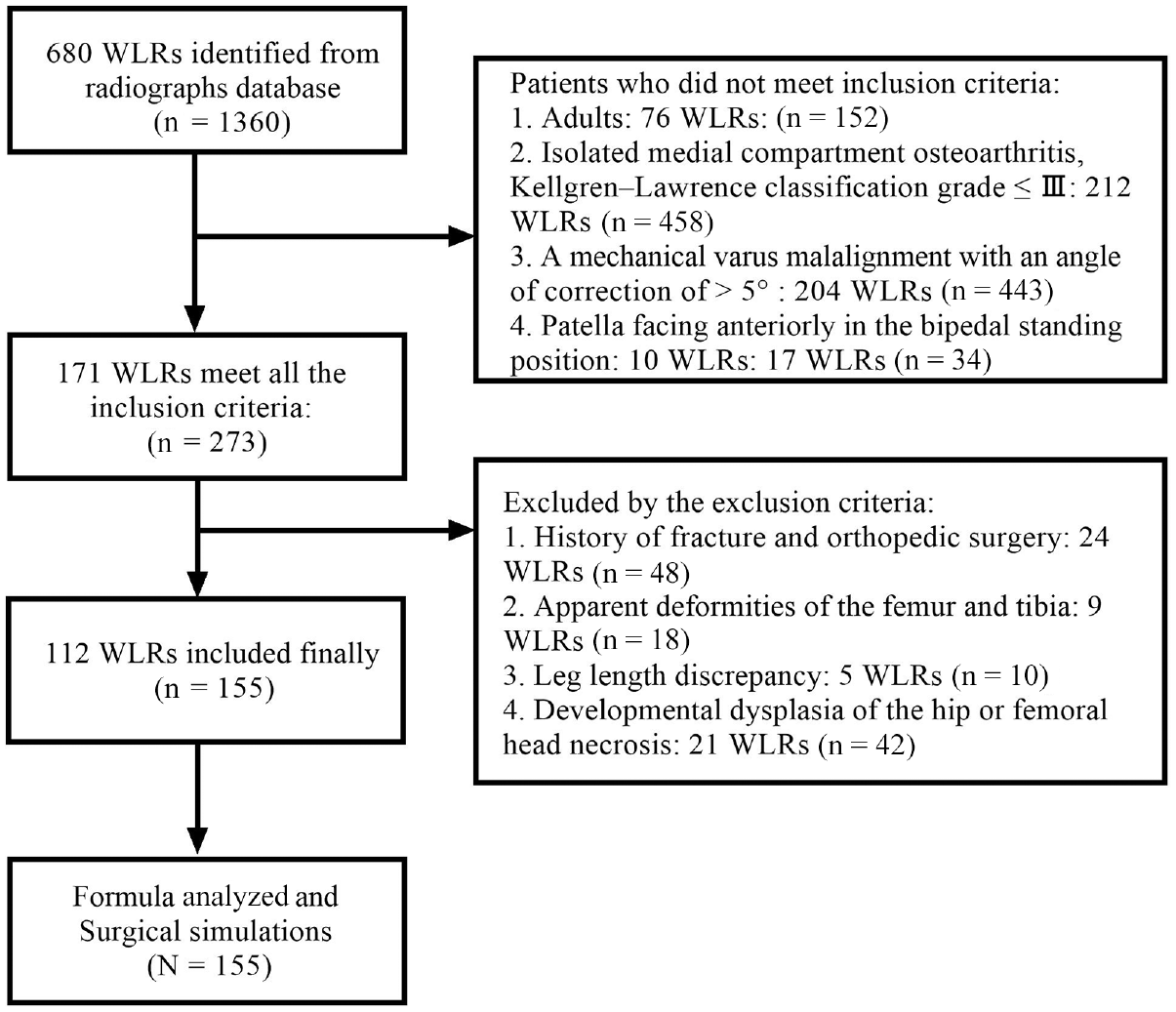
Flow diagram of patients’ whole-leg radiography (WLR) enrollment.
Presurgical Planning
Personalized surgical planning was performed using commercial software based on standing WLRs (Medraw V1; Image Medraw Technology). Surgical planning was simulated according to the Miniaci approach. The Miniaci method began by establishing a reference line from the hip joint center to the correction point at the knee joint line, extending it to the ankle level. From the hinge point, located approximately 1.5 cm from the articular surface, one line was drawn to the terminal point of reference line and another line to the center of the ankle joint. The angle formed by these 2 lines was the Miniaci angle, which was the degree of adjustment required for the surgical procedure.19,23 The measurement of parameters and selection strategy for landmarks have been reported in a previous study. 12 The related anatomical landmarks were selected by 2 experienced orthopaedic surgeons (H.C., L.C.). Three goals, including the Fujisawa point, 65% WBL percentage, and postsurgical HKA angle of 4.5° valgus, were set and analyzed by adjusting the postoperative targets. The main parameters included in the study were Miniaci angle, HKA angle, and WBL percentage. The Miniaci angle was defined as the correction angle between the upper and lower osteotomy lines in computer simulations. The HKA angle was defined as the angle between the mechanical axis of the tibia and femur, and the WBL percentage was calculated as the percentage of the tibial plateau width (medial to lateral) where the mechanical axis of the lower limbs crossed.
Formula Calculation
In our previous research, we derived these formulas by analyzing the linear relationships between the preoperative parameters and the Miniaci angle, noting that their determination coefficients closely approximated a value of 1. 12 The robust linear relationships indicated that these conversion formulas could have broad application potentials. This study incorporates these formulas for rigorous external validation to test their applicability. The 4 formulas are listed in Table 1. The related independent variables were integrated into formulas, and the results of the dependent variables were recorded.
Conversion Formulas Between the Miniaci Angle and Overall Lower Limb Alignment Parameters a

Δ, change in presurgical parameters; HKA, hip-knee-ankle; Pre-, presurgery; WBL %, weightbearing line percentage.
Statistical Analysis
The primary outcome measured in our study was the difference between the formulas and computer simulations in terms of the Miniaci angle. Descriptive statistics for quantitative variables are presented as the mean ± SD (95% CI) or median (lower quartile–upper quartile). The Bland-Altman method was used to plot the difference between the formula results and the simulated correction angles determined by the Miniaci method. Spearman correlation analysis was used to analyze the relationship between the Miniaci angle and the formula results. Correlation values were classified as follows: perfect association (0.91–1.00), strong association (0.50–0.90), moderate association (0.30–0.49), weak association (0.01–0.29), and no association (0.00). To assess the intraclass correlation coefficients, we randomly selected 30 additional lower limbs for measurement, on which 2 independent orthopaedic surgeons (H.C., L.C.) conducted surgical simulations twice 2 weeks apart. The intra- and interrater reliabilities were 0.849-0.995 and 0.800-0.989, respectively (see Appendix Table A1). All statistical analyses were performed using SPSS (Version 26; IBM). Statistical significance was defined as P < .05.
Results
A total of 155 lower limbs from 112 patients (91 female and 21 male) were included in this study. Two orthopaedic surgeons (H.C., L.C.) used all eligible lower limbs to perform formula calculations and computer simulations. The baseline results of the 3 surgical target groups, including patient demographics and surgery-related radiographic parameters, are shown in Table 2.
Demographic and Radiographic Parameters for Patients a

Δ, change in presurgical parameters; HKA, hip-knee-ankle; mMPTA, mechanical medial proximal tibial angle; Post-, postsurgery; Pre-, presurgery; WBL %, weightbearing line percentage.
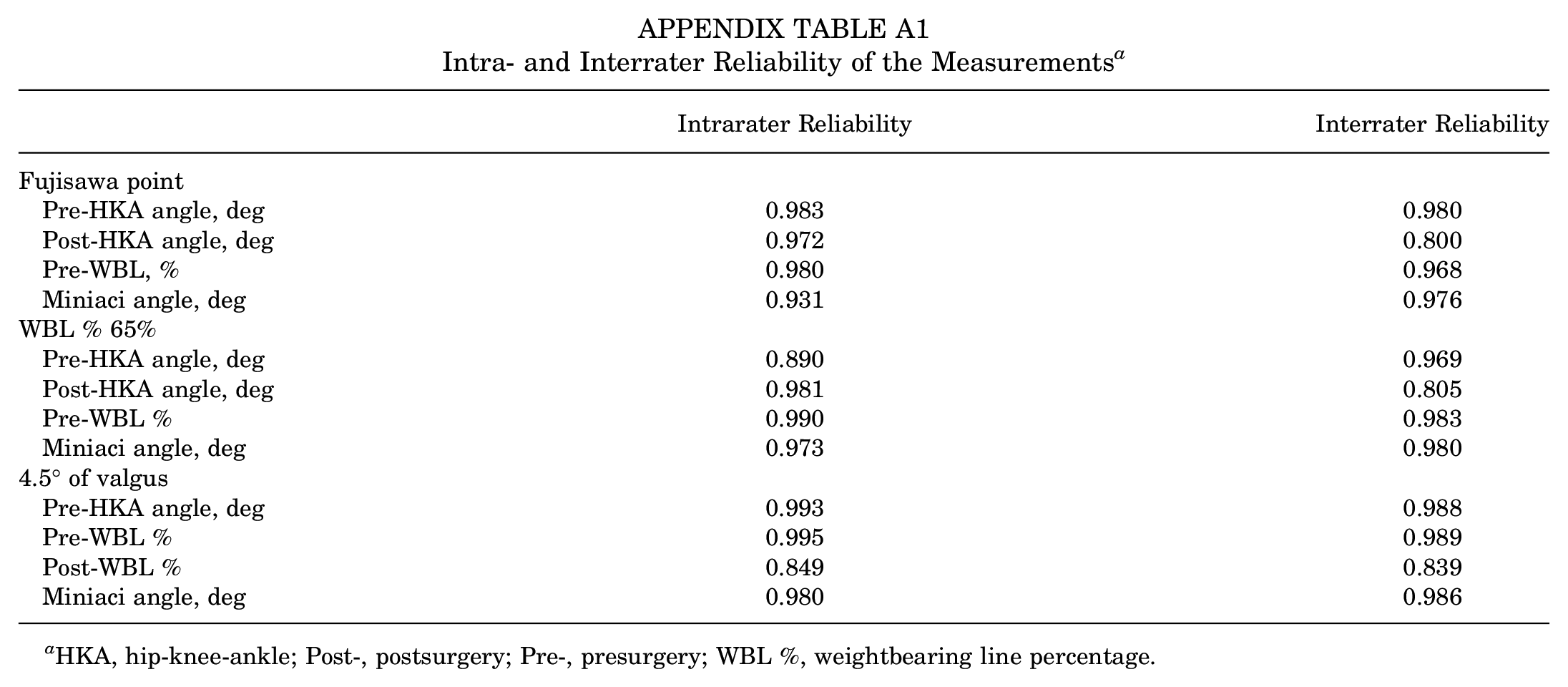
The intra- and interrater reliabilities of the parameters are shown in Appendix Table A1. For the Fujisawa point (62.5%), the reliabilities of presurgical HKA angle, postsurgical HKA angle, presurgical WBL percentage, and Miniaci angle were 0.931-0.983 and 0.800-0.980, respectively. For a WBL percentage of 65%, the reliabilities of the presurgical HKA angle, postsurgical HKA angle, presurgical WBL percentage, and Miniaci angle were 0.890-0.990 and 0.805-0.983, respectively. For a postsurgical HKA angle of 4.5° valgus, the reliabilities of the presurgical HKA angle, presurgical WBL percentage, postsurgical WBL percentage, and Miniaci angle were 0.849-0.995 and 0.839-0.989, respectively (see Appendix Table A1).
Table 3 shows the analysis results of Spearman correlation between the parameters. Regarding the Fujisawa point as the postsurgery target, the calculation outcome of formulas 1 to 4 showed a perfect association with the computer simulation results (r = 0.962-0.999). When WBL percentages of 65% and an HKA angle of 4.5° valgus were set as postsurgical targets, all formulas showed similar performance to the Fujisawa point group, showing a perfect correlation with the simulated results (r = 0.961-0.999 and r = 0.951-0.998).
Spearman Correlation Analysis Between Formula Calculation Outcome and Simulated Parameters a
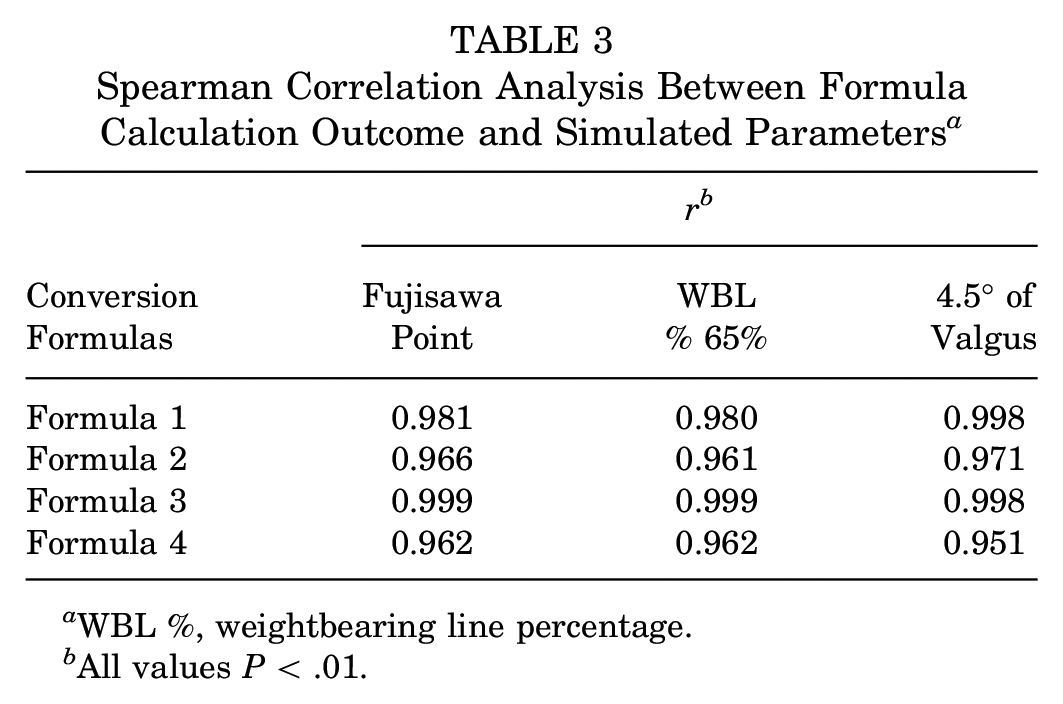
WBL %, weightbearing line percentage.
All values P < .01.
A Bland-Altman analysis was performed to confirm the accuracy of the above formulas, shown in Figures 2 to 4. For the Fujisawa point group, the mean bias value (95% CI) of formulas 1 to 4 in predicting the Miniaci angle was 0.098° (−0.606° to 0.801°), –0.268° (−1.335° to 0.799°), 0.065° (−0.116° to 0.245°), –0.246° (−1.349° to 0.857°), respectively (Figure 2). The currently accepted error range of the Miniaci angle in clinical practice is less than 1.63° and 1.18° for HKA- and WBL-based planning, respectively. 11 The success rates of formulas 1 to 4 are listed in Table 4. All formula rates were >92%, indicating that the results had an excellent level of agreement with the computer-simulated Miniaci angle. Notably, formula 1 and formula 3 achieved a 100% success rate (Table 4).

The Bland-Altman analysis of the bias between the formula calculation and the computer-simulated Miniaci angle in the Fujisawa point group. The computer-simulated Miniaci angle is compared with the calculation results from formula 1 (A), formula 2 (B), formula 3 (C), and formula 4 (D).s; HKA, hip-knee-ankle; Pre-, presurgery; WBL %, weightbearing line percentage.

The Bland-Altman analysis of the bias between the formula calculation and the computer-simulated Miniaci angle in the WBL % 65% group. The computer-simulated Miniaci angle is compared with the calculation results from formula 1 (A), formula 2 (B), formula 3 (C), and formula 4 (D). Δ, change in presurgical parameters; HKA, hip-knee-ankle; Pre-, presurgery; WBL %, weightbearing line percentage.

The Bland-Altman analysis of the bias between the formula calculation and the computer-simulated Miniaci angle in the 4.5° of valgus group. The computer-simulated Miniaci angle is compared with the calculation results from formula 1 (A), formula 2 (B), formula 3 (C), and formula 4 (D). Δ, change in presurgical parameters; HKA, hip-knee-ankle; Pre-, presurgery; WBL %, weightbearing line percentage.
Successful Rate of Formula Calculation Results a

Data are presented as percentages. WBL %, weightbearing line percentage.
The Bland-Altman results with a WBL percentage of 65% are shown in Figure 3. For formulas 1 to 4, the mean bias values (95% CI) in predicting the Miniaci angle were 0.677° (−0.068° to 1.422°), 0.311° (−0.819° to 1.441°), 0.070° (−0.121° to 0.261°), and −0.282° (−1.407° to 0.843°), respectively. The success rate of all formulas was >80%, indicating that the results maintained a good level of agreement with the simulated Miniaci angle in 65% of the WBL situations (Table 4). The mean bias of formula 1 reached approximately 0.5°, whereas the others remained similar.
The Bland-Altman results with a postsurgical HKA angle of 4.5° are shown in Figure 4. For formulas 1 to 4, the mean bias values (95% CI) in predicting the Miniaci angle were 1.571° (1.367° to 1.776°), 1.209° (0.183° to 2.235°), 0.080° (−0.127° to 0.287°), and −0.371° (−1.660° to −0.918°), respectively. The success rate of formula 3 was 100%, and that of formula 4 added up to 95%; however, the others dropped to unsatisfactory levels (Table 4).
Discussion
The primary finding of this study was that formulas 1 to 4, based on preoperative parameters, exhibited commendable accuracy in targeting the Fujisawa point during external validation. Furthermore, the HKA-based conversion formulas showed superior performance to that of the WBL-based formulas when applied to broader planning targets, especially formula 3. In the Fujisawa point group, we found that formulas based on the presurgical HKA angle and WBL percentage showed perfect accuracy and consistency on another radiographic machine. The correlation value (r = 0.962-0.999) of the formulas and computer simulations indicates that the conversion formulas resemble the digital planning results. The Bland-Altman analysis of the Miniaci angle calculated using formulas showed that the exact bias was mostly < ±1.63° and ±1.18° for HKA- and WBL-based planning, which is acceptable in clinical practice. 11 This result strongly validates the finding of Jiang et al 12 that the Miniaci angle is perfectly correlated with the presurgical HKA angle and presurgical WBL percentage and that conversion formulas have reliable and practical applications. The formulas based on the presurgical HKA angle and presurgical WBL percentage simplify the complex surgical planning of OWHTO, while achieving a nearly 100% success rate in gaining the Miniaci angle. However, for broader surgical targets, such as an HKA angle of 4.5°, formulas based on ΔHKA showed the best accuracy and reliability while achieving the least bias with the simulated Miniaci angle. Depending on these conversion formulas, orthopaedic surgeons can easily calculate the Miniaci angle using the presurgical parameters on the WLR without any other digital software. The Miniaci angle can help ascertain the angular correction with high reliability and efficiency. 2 Surgeons can then directly measure the exact gap with the Miniaci angle and the depth of osteotomy.19,24
In this study, we evaluated the power of formulas based on the presurgical HKA angle and presurgical WBL percentage in the WLRs of different radiographic machines. In the study of Jiang et al, 12 HTO formulas were invented by combining computer surgical simulation and Miniaci methods. Despite various projection sources and the projection ratio from the radiographic machine, formula 1, based on the presurgical HKA angle, and formula 2, based on the presurgical WBL percentage, still maintained a perfect correlation with the computer-simulated Miniaci angle (Table 3). The formula results, which maintained a success rate of nearly 100%, were considered reliable for presurgical planning (Table 4). In our surgical simulations, these formulas have demonstrated exceptional reliability across different radiographic machines, proving themselves to be valuable tools for osteotomy procedures. By targeting the mechanical axis of the limb passing through the Fujisawa point, surgeons can easily calculate the Miniaci angle with satisfactory accuracy using these formulas.
Furthermore, formula 3, which utilized ΔHKA angle before and after surgery, showed the best applicability and stability when targeting a broader range of postoperative HKA angles or WBL percentages. As shown in Tables 3 and 4, the results of formulas between the Miniaci angle and ΔHKA angle have the strongest association with the simulated Miniaci angle (r > 0.99) and are 100% acceptable for clinical practice. The exact Miniaci angle could be considered while maintaining a bias of nearly 0 (Figures 2-4). Based on the presurgical HKA, the Miniaci angle can be directly estimated by selecting a postoperative HKA angle target between 3° and 6°. 7 The results of the formula between the Miniaci angle and ΔWBL percentage were perfectly associated with the simulated Miniaci angle and were 90% acceptable for the surgical plan in the 3 groups. However, it is worth noting that formula 3, based on the ΔHKA angle, always performed better than formula 4 based on the ΔWBL percentage. In the 4.5° of valgus group, the mean value of the post-WBL percentage was 69.0% (68.0%-70.0%), which is far from the Fujisawa point, and formula 2 based on the pre-WBL percentage only achieved a success rate of 78.39%, which is much lower than formulas based on ΔHKA angle. This indicates that the HKA angle is a more reliable parameter when using the Miniaci method. This was consistent with the findings of Jiang et al, 11 who found that the HKA angle has less error and slighter variability than the WBL percentage. Although Miniaci et al 19 claimed to achieve a WBL passing 60% to 70% of the width of the tibial plateau after surgery, the calculation of the formula based on WBL percentage appears less accurate than formulas based on HKA angle for a broader target range.
Although the Fujisawa point is the most recognized target for most surgeons, its validity has been challenged, particularly due to the lateral closed-wedge operative approach and the small sample size. Therefore, surgeons commonly choose different realignment targets in clinical practice. Martay et al 18 found that the postsurgical WBL percentage, which is between 50% and 60%, could be considered a safe zone for balancing the medial and lateral compartment stresses according to their finite element analysis. In addition, Lee et al 16 and Jiang et al 10 found that surgery aimed at the lateral tibial spine had clinical outcomes similar to those of the Fujisawa point. Therefore, the proper realignment target should be personalized by considering the balance of compartment stress, bias in correction, and the effects of soft tissue laxity. Our formulas based on ΔWBL percentage and ΔHKA angle maintain satisfactory success rates in 3 different target groups, especially those based on ΔHKA angle; hence, they could help surgeons assess the correction angle when aiming at personalized targets.
Potential discrepancies in presurgical planning have been analyzed previously. In a comparative clinical study, the prediction of the presurgical osteotomy angle of OWHTO using the Miniaci method was reliable. Compared with the Dugdale method, a minor error of correction angles was obtained using the Miniaci method. 23 Similarly, researchers compared 2 groups of cases using the cable and Miniaci methods, and the results showed that the Miniaci method acquired a superior ectropion angle and WBL percentage after the operation. 24 Although some studies have questioned the complexity of the Miniaci method,2,23 our formulas simplify the planning process and do not require specific digital planning software.
Although achieving an accurate osteotomy angle is critical for lower limb alignment correction, 2 this aim is difficult to target in presurgical planning. While advocates of patient-specific instrumentation (PSI) and computer navigation claim superior accuracy and clinical efficacy, others warn that these technologies require complex and expensive hardware and software products.3,5,6 In addition, PSI and computer navigation are considered more time-consuming.1,25 While the conversion formulas may not offer the same level of precision and intraoperative guidance as computer-assisted navigation or PSI, they serve as a beneficial tool for preoperative planning. These formulas enable surgeons to calculate the Miniaci angle using presurgical parameters efficiently. By integrating the Miniaci angle and the depth of the osteotomy, the gap of the medial opening wedge is calculated using trigonometric functions.12,14 Although the gap can be influenced by factors such as the thickness of the bone saw and the imperfect osteotomy process, these deviations can be effectively corrected during surgery. This is achieved through extraosseous verification techniques, specifically by monitoring the changes in the distance between markers strategically positioned near the osteotomy line. 9
Limitations
This study has several limitations that should be acknowledged. First, the calculation of the conversion formula and computer simulations is theoretical. A prospective study that includes actual surgical results may be more feasible in this context. However, our study included a large cohort without selection bias and achieved excellent intra- and interrater reliability. Second, as a computer simulation–based study, we did not consider the soft tissue and laxity of the knee, which can alter the joint space, and the change in the joint line convergence angle in OWHTO. In the near future, we will further evaluate the impact of soft tissue and knee joint laxity on the osteotomy in a prospective randomized controlled trial study. Third, the formula results did not perfectly reflect accurate postoperative parameters owing to individual differences. Fourth, our formula calculation and computer simulation were limited to postsurgical targets within a valgus of 3° to 6° or a WBL percentage of 60% to 70%. However, the accuracy of these formulas can be guaranteed within this range, and the aforementioned targeting range is widely accepted.
Conclusion
The formulas based on the presurgical HKA angle and WBL percentage accurately predicted the Miniaci angle targeting the Fujisawa point. The formula based on ΔHKA angle achieved the best accuracy and represented a potentially valuable tool for predicting the Miniaci angle in broader surgical targets. These formulas related to the Miniaci method could be applied to simplify OWHTO planning by calculating the gap for the medial opening wedge without complex surgical simulation.
Footnotes
Appendix
Intra- and Interrater Reliability of the Measurements a
| Intrarater Reliability | Interrater Reliability | |
|---|---|---|
| Fujisawa point | ||
| Pre-HKA angle, deg | 0.983 | 0.980 |
| Post-HKA angle, deg | 0.972 | 0.800 |
| Pre-WBL, % | 0.980 | 0.968 |
| Miniaci angle, deg | 0.931 | 0.976 |
| WBL % 65% | ||
| Pre-HKA angle, deg | 0.890 | 0.969 |
| Post-HKA angle, deg | 0.981 | 0.805 |
| Pre-WBL % | 0.990 | 0.983 |
| Miniaci angle, deg | 0.973 | 0.980 |
| 4.5° of valgus | ||
| Pre-HKA angle, deg | 0.993 | 0.988 |
| Pre-WBL % | 0.995 | 0.989 |
| Post-WBL % | 0.849 | 0.839 |
| Miniaci angle, deg | 0.980 | 0.986 |
HKA, hip-knee-ankle; Post-, postsurgery; Pre-, presurgery; WBL %, weightbearing line percentage.
Final revision submitted July 20, 2024; accepted July 29, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the National Natural Science Foundation of China (12272232); Science and Technology Commission of Shanghai Municipality (23S31905900, 20ZR1432000, 21S31905500); Project of Biobank (YBKB202118) from Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine; and a grant from Shanghai Ninth People’s Hospital (2022yxyjxys-wl). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine (SH9H-2023-T97-1).