
Abstract
Background:
There is still controversy regarding the ideal management method for meniscal tears combined with anterior cruciate ligament (ACL) injury, especially for professional athletes.
Purposes:
To (1) describe the incidence of secondary meniscectomy in professional athletes after undergoing meniscal repair concomitant to primary ACL reconstruction (ACLR) and (2) identify the associated risk factors for repair failure of the medial meniscus (MM) and/or lateral meniscus (LM) in this population at long-term follow-up.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This was a retrospective comparative study. Included were professional athletes who underwent arthroscopic primary ACLR and repair of MM and/or LM tears between January 2013 and December 2022and who had ≥2 years of follow-up. Risk factors associated with secondary meniscectomy were analyzed using a Cox proportional hazards model.
Results:
Out of 230 professional athletes (mean ± SD age, 23.3 ± 5.0 years; mean Tegner score, 9.3 ± 1.0) who underwent primary ACLR, 196 patients (85.2%) also had meniscal repair. The most common type of graft used was hamstring tendon (74%), and 74% of patients underwent a concomitant lateral extra-articular procedure. Among the 196 patients with meniscal lesions, 37% had LM lesions, 29% had MM lesions, and 34% had both LM and MM lesions. LM tears were repaired in 92.8% of cases, while 7.2% were left in situ. The most common type of repair for LM tears was the all-inside technique. MM tears were repaired in 97.6% of cases, with 2.4% left alone. The most common type of repair for MM tears was the suture hook technique, and no meniscectomies were performed. At a mean follow-up of 95.8 ± 45.1 months, 26 patients (13.3%) underwent a secondary meniscectomy: 7 (5.0%) for LM and 19 (15.4%) for MM. A Cox model revealed no significant risk factors associated with secondary lateral or medial meniscectomy.
Conclusion:
At long-term follow-up, the meniscal repair failure rate in this population of patients who underwent primary ACLR was 13.2% overall, 5% for LM tears and 15.4% for MM tears. No risk factors for secondary meniscectomy were found.
Keywords
Meniscal tears combined with anterior cruciate ligament (ACL) injuries are common in professional athletes facing the high demand for their participation in sporting activities.6,13 Meniscal injuries have been reported to occur in 41% to 82% of individuals with ACL injuries, and an increased incidence of meniscal injuries is noted with participation in contact sports.5,25,37 Meniscal tears and ACL injuries, as well as surgical treatment for these injuries, have been shown to be associated with decreased durability while playing sports.8,30,32 Historically, meniscectomy has been preferred over meniscal repair in professional athletes because it allows quicker return to play and avoids meniscal repair failure. 24 However, the meniscus plays an important role in protecting the knee joint through means such as shock absorption, load bearing, knee stability, lubrication, and articular cartilage nutrition.1,19,27,54,55 Long-term studies of patients after ACL reconstruction (ACLR) have demonstrated that meniscectomy is associated with increased rates of osteoarthritis.10,23,34 It is now accepted that meniscal repair reduces the risk of radiographic degenerative changes.51,54 Treatment options for meniscal tears have shifted from meniscectomy to meniscal repair over the past 2 decades.4,30,51 Various arthroscopic techniques and devices for meniscal repair have evolved to improve the outcomes of meniscal repair. 33 However, previous reports have indicated that the success rate of meniscal repair is not high in professional athletes.22,28
Due to the lack of sufficient evidence, there is still controversy regarding the ideal management of meniscal tears combined with ACL injuries, especially for professional athletes. An analysis of possible predictors of meniscal repair outcomes is highly desirable. A better understanding of the expected outcome will facilitate a more differentiated approach to optimal surgical treatment.
The primary objective of this study was to describe the incidence of secondary meniscectomy in professional athletes who underwent meniscal repair concomitant to primary ACLR. The second objective was to identify the associated risk factors for repair failure of the medial meniscus (MM) and/or lateral meniscus (LM) in this specific population at long-term follow-up. Our hypothesis was that the incidence of secondary meniscectomy would be significant and that MM repair would demonstrate a higher long-term failure rate compared with LM repair.
Methods
Patient Enrollment
Institutional review board approval was granted for this study, and all patients provided informed consent to participate. We performed a retrospective analysis of prospectively collected data from the Scientific Anterior Cruciate Ligament Network International (SANTI) Study Group. All patients who underwent arthroscopic primary ACLR performed by a single surgeon (B.S.-C.)between January 2013 and December 2022 were considered eligible for the study. All of these patients had sustained ACL tears and were diagnosed on the basis of clinical examination and magnetic resonance imaging. The patients were unable to resume their previous levels of activity because of instability symptoms and therefore underwent ACLR.
From this group, all individuals who were professional athletes and who underwent MM and/or LM repair were identified. Patients were defined as professional athletes via participation in competition at national and/or international levels at the time of injury and whose primary source of income stemmed from performing their sport. Athletes who had <2 years of follow-up, who underwent major concomitant surgery (eg, multiligament reconstructions), or who refused to provide consent were excluded.
Surgical Techniques for Meniscal Repair and ACLR
Patients were positioned in the standard arthroscopy position, with lateral support at the level of a padded tourniquet and a foot post to allow the knee to be maintained at 90° of flexion when needed. All patients underwent systematic standard arthroscopic exploration of the knee and scoping of the posteromedial compartment with a transnotch view from the anterolateral portal to visualize meniscocapsular attachment in the posterior horn.44,53 The meniscocapsular attachments and meniscus were evaluated by probing with either a needle or an arthroscopy hook inserted through a posteromedial portal.50,53
ACLR was performed either as an isolated procedure or in conjunction with a lateral extra-articular procedure (LEAP). ACL grafts included quadrupled semitendinosus tendons, 46 bone–patellar tendon–bone, 21 or, in the case of combined ACL–anterolateral ligament grafts, a tripled semitendinosus with a single strand of gracilis (Figure 1).40,45 The decision to use a particular graft type was based on patient factors/choices. The combined LEAP increased over the study period. LEAP was performed with double-strand gracilis autograft 40 or with an iliotibial band strip. 9 The decision to perform a LEAP was based on patient preference and the surgeons’ evolving criteria for LEAPs during the study period. Over time, the indications for combined procedures expanded to include grade 3 pivot shift, chronic injuries, hyperlaxity, and young patients who participated in pivoting sports, as these factors indicate a high-risk population. This expansion was further supported by our positive clinical outcomes.

Surgical techniques for anterior cruciate ligament reconstruction (ACLR): isolated ACLR with (A) bone–patellar tendon–bone or (B) quadrupled semitendinosus/gracilis tendons versus combined ACLR with a lateral extra-articular procedure using (C) a double strand of gracilis or (D) an iliotibial band strip.
Postoperative Rehabilitation Protocol
Two different protocols were adopted depending on the affected meniscus. For the MM, this consisted of brace-free, immediate full weightbearing and progressive range of motion exercises, with restricted range of motion from 0° to 90°, regardless of the surgical repair technique. For the LM, rehabilitation consisted of partial weightbearing and a brace locked in extension, except during prescribed exercises. In both cases, the main objectives were to activate the vastus medialis obliquus through biofeedback, allow knee flexion without forcing it, and protect the meniscal repair and ACLR. When the range of motion was restored, the knee showed no signs of intra-articular effusion, and ligament testing was normal, the protocol allowed a gradual return to running, never before 4 months, to protect the meniscal repairs. Return to sports was allowed at 4 months for nonpivoting sports, 6 months for pivoting noncontact sports, and 8 to 9 months for pivoting contact sports.
Epidemiological and Risk Factor Analysis of Meniscal Repair Failure
The data collected included sex, body mass index, age, year at which the ACL injury was sustained while the patient was participating in a contact or noncontact sport (although data on the specific mechanism of injury were not available), preoperative Tegner activity score, preoperative side-to-side laxity difference, and primary or revision ACLR. Treatment delay was also examined as a continuous variable. For patients who underwent concomitant meniscal repair, the MM and LM tears were categorized based on tear pattern: longitudinal, radial, horizontal, root, and complex. Longitudinal tears of the posterior horn of the MM included ramp lesions. Meniscal repairs were categorized based on technical patterns, including no repair, all-inside, mixed, outside-in, hook, and pullout patterns. For the MM, each case was evaluated separately, promoting repair in red or white-red zones. For the LM, repair was mandatory due to the biomechanical consequences and complication known of a lateral meniscectomy. 11
For failure, the results of both MM and LM repair during the same surgical procedure were analyzed separately. Treatment failure was defined as the need to undergo subsequent surgery to address persistent meniscal symptoms after repair and after being confirmed by radiological images. The time to meniscal repair failure was recorded for analysis.
Follow-up Schedule and Data Collection
Follow-up was scheduled at 3 and 6 weeks and at 3, 6, and 12 months postoperatively. Physical examination with side-to-side laxity difference and meniscal test was performed at each control. In the face of a new onset of meniscal symptoms, a computed tomography scan with intravenous contrast injection was performed to confirm the diagnosis of a new meniscal lesion or failure of repair.
After the first year, follow-up was conducted annually when possible. The end of the study was defined as November 2020. For each participant, the final follow-up was defined as the most recent examination before this date according to the data collected prospectively in the Santy database. Public media were also followed to determine whether any of the players had undergone additional surgery at another center.
Data Analysis
All statistical calculations were performed with SAS for Windows (Version 9.4; SAS Institute Inc), with the level of statistical significance set at P < .05. Descriptive data analysis was conducted depending on the nature of the considered criteria. The quantitative data are reported as the number of observed (and missing, if any) values, means with standard deviations, and ranges. The qualitative data are reported as the number of observed (and missing, if any) values and the number and percentage of patients per class. Patient characteristics were further evaluated according to the meniscal repair location (medial or lateral) and repair technique. The Fisher exact test and the chi-square test were used to analyze categorical data, and continuous variables were evaluated using analysis of variance with the Bonferroni adjustment for multiple comparisons. Survival analysis, or specifically, Cox proportional hazards modeling, was used to determine whether meniscal repair failure rates differed according to the location and technique of meniscal repair. The time of study entry was defined as the date of meniscal repair for all patients. The time to event for patients who experienced failure of meniscal repair was the date of subsequent surgery. Risk factors, such as age, sex and sports type, were included in the Cox proportional hazards models.
Results
Patient Characteristics
A total of 196 professional athletes from 230 ACLRs were included in the present study (Figure 2), with an incidence of meniscal tears of 85.2%. Among the 196 patients with meniscal lesions, 73 (37.2%) had LM lesions, 57 (29.1%) had MM lesions, and 66 (33.7%) had lesions in both the LM and the MM. The LM tears were repaired in 92.8% of cases, while 7.2% were left in situ. The MM tears were repaired in 97.6% of cases, with 2.4% left alone, and no meniscectomies were performed. The overall mean age, Tegner activity score, and follow-up time were 23.3 ± 5.0 years, 9.3 ± 1.0, and 95.8 ± 45.1 months, respectively (Table 1).

Flowchart of patient inclusion and exclusion. ACL, anterior cruciate ligament.
Patient Characteristics (N = 196 Patients) a

Data are presented as mean ± SD or n (%).
Range, 25.2-214.7 months.
Meniscal Tears by Sport and Type of Sport
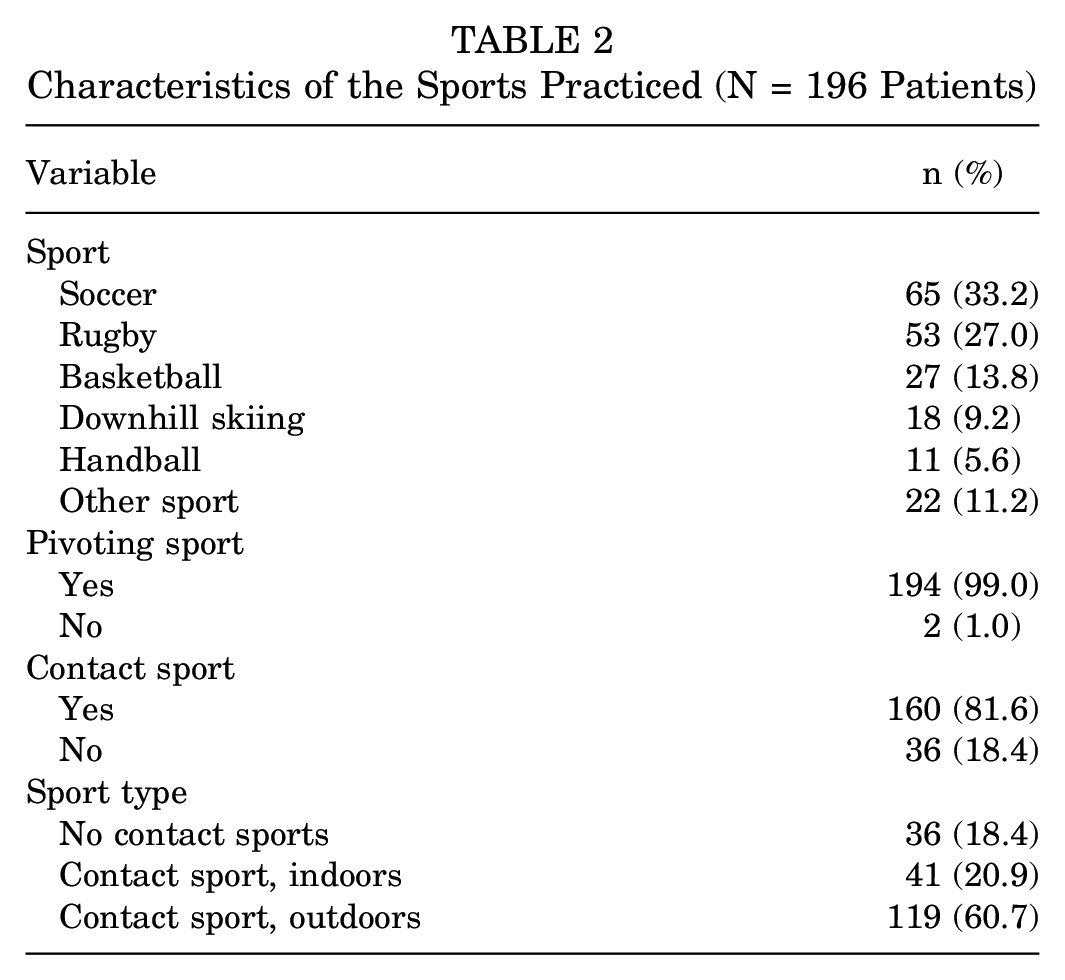
Soccer and rugby were the most common sports practiced, with 65 (33.2%) and 53 (27.0%) athletes participating, respectively (Table 2). A total of 194 (99.0%) patients practiced pivoting sports, and 2 patients practiced horse riding. Overall, 160 (81.6%) patients practiced contact sports (Table 2).
Characteristics of the Sports Practiced (N = 196 Patients)
Intraoperative Procedures and Findings
The most common graft type used was hamstring tendon (145 patients; 74.0%). A total of 145 (74%) patients underwent LEAP (Table 3). For LM lesions, the most common tear type and repair technique were longitudinal tears of the posterior horn (68 patients; 48.9%) and the all-inside suture technique (111 patients; 79.9%) (Table 4). For MM lesions, the most common tear type and repair were ramp lesions (104 patients; 84.6%) and the suture hook technique (69 patients; 56.1%) (Table 4).
Intraoperative Procedures and Findings (N = 196 Patients) a

BPTB, bone–patellar tendon–bone; HT, hamstring tendon; LEAP, lateral extra-articular procedure; QT, quadriceps tendon.
Types of LM and MM Tears and Repairs a

There were 73 isolated LM repairs, 57 isolated MM repairs, and 66 LM or MM repairs combined with medial lesions. LM, lateral meniscus; MM, medial meniscus.
Incidence of Secondary Lateral and Medial Meniscectomy
Overall, 26 patients (13.3%) underwent a secondary meniscectomy. Of the 139 patients who had a LM previous lesion, 7 (5.0%) underwent a secondary lateral meniscectomy. The incidence rate of secondary lateral meniscectomy–free status at 60 months according to the Kaplan-Meier method was 95.5% (95% CI, 90.3-98.0) (Figure 3A). The Cox model showed no significant risk factors associated with secondary lateral meniscectomy (Table 5).

Time to (A) secondary lateral meniscectomy and (B) secondary medial meniscectomy according to meniscal tear. (A) The incidence rate of secondary lateral meniscectomy–free status at 60 months according to the Kaplan-Meier method was 95.5 (95% CI, 90.3-98.0). (B) The incidence rate of secondary medial meniscectomy–free status at 60 months according to the Kaplan-Meier method was 85.6 (95% CI, 77.7-90.8).
Cox Proportional Hazards Model for Secondary Lateral or Medial Meniscectomy: Multivariate Analysis (n = 139 Observations) a

BPTB, bone–patellar tendon–bone; HR, hazard ratio; HT, hamstring tendon; LEAP, lateral extra-articular procedure; LM, lateral meniscus; MM, medial meniscus; QT, quadriceps tendon.
Overall, of 123 patients who had a previous MM lesion, 19 (15.4%) patients underwent a secondary medial meniscectomy. The incidence rate of secondary medial meniscectomy–free status at 60 months according to the Kaplan-Meier method was 85.6% (95% CI, 77.7-90.8) (Figure 3B). The Cox model showed no significant risk factors associated with a secondary medial meniscectomy (Table 5).
Complications
Ten (5.1%) patients had an ACL graft rupture. Eleven (5.6%) patients had cyclops lesions. Fifteen (7.7%) patients underwent arthrolysis surgery (Table 6).
Incidence of Complications (N = 196 Patients) a
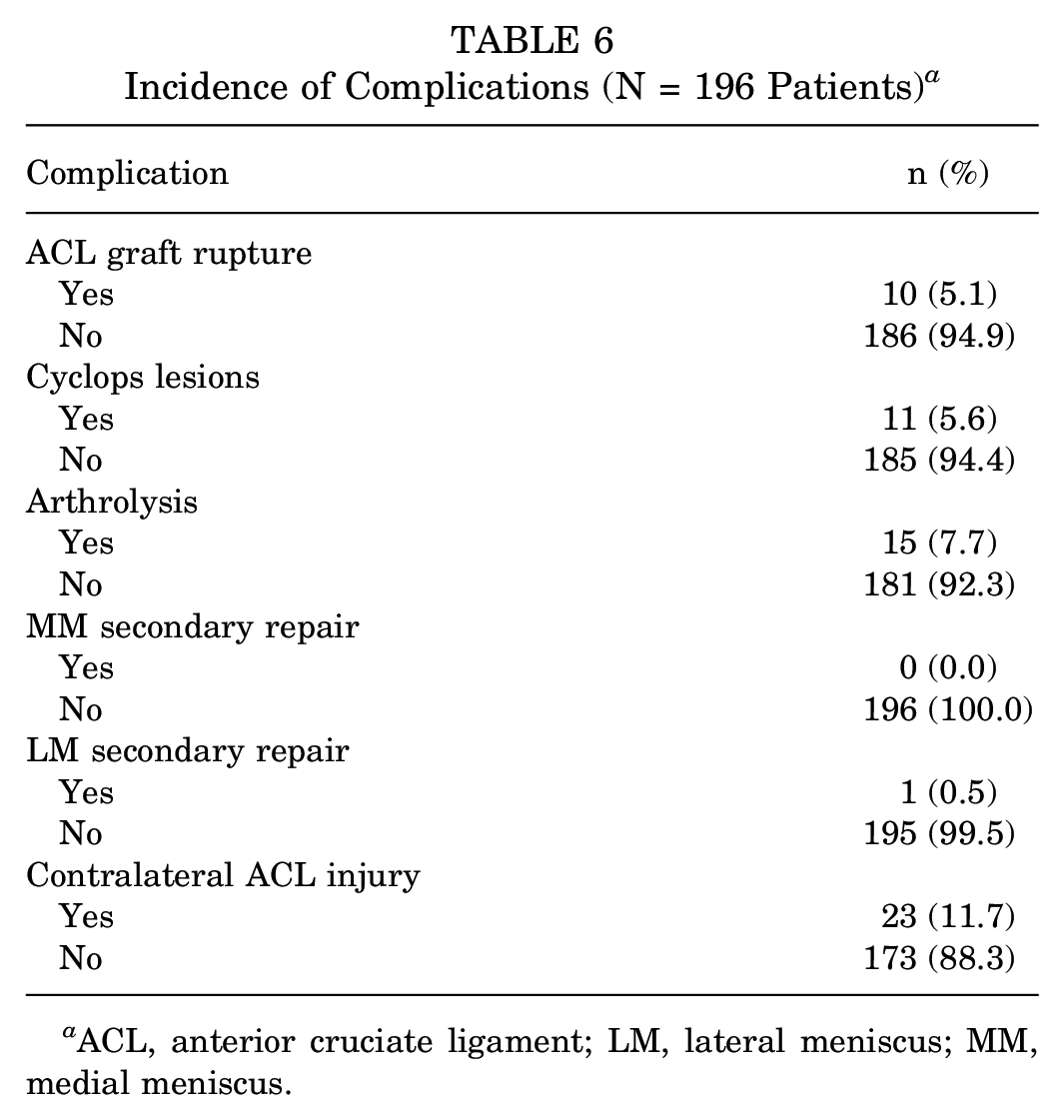
ACL, anterior cruciate ligament; LM, lateral meniscus; MM, medial meniscus.
Discussion
This study showed that among professional athletes with ACL ruptures, the incidence of meniscal tears reached 85.2% (196/230) of the cases. A total of 37% had LM lesions, 29% had MM lesions, and 34% had lesions in both menisci. Specifically, the most common LM lesions were longitudinal tears (51.1%), and the most common MM lesions involved longitudinal tears of the posterior horn, including ramp lesions (85.2%). During long-term follow-up, the rate of secondary meniscectomy was 15.4% for the MM tear group and 5.0% for the LM tear group. Cox proportional hazards model revealed no significant risk factors associated with secondary lateral or medial meniscectomy.
The current study comprises the largest long-term cohort of 196 professional athletes in which the incidence and failure rate of meniscal lesions combined with an ACL injury were analyzed. However, studies analyzing the incidence of meniscal lesions and the clinical outcomes of meniscal repair combined with ACLR in professional athletes are rare. Farinelli et al 14 reported concomitant injuries associated with ACL rupture in elite professional alpine ski racers (n = 44) and soccer players (n = 37). Ramp lesions and longitudinal tears represented 14% and 19% of soccer players, respectively. On the lateral side, longitudinal tears, posterior root tears, and radial tears represented 24%, 16%, and 16% of professional athletes, respectively. In alpine skiers, the most common types of MM tears were bucket-handle (16%) and longitudinal tears (14%). On the lateral side, longitudinal and complex tears represented 27% and 16% of professional athletes, respectively.
According to a systematic review by Nepple et al, 31 MM repairs are significantly more likely to fail compared with LM repairs (23.9% vs 12.6%; P = .04). Logan et al 22 reported the incidence of meniscal lesions and clinical outcomes of meniscal repair in 45 elite athletes (mean follow-up, 8.5 years): MM repair, 67%; LM repair, 33%; ACLR, 83.3%. In their series, the failure rates of MM and LM repair were 36.4% and 5.6%, respectively. In the present study, the rate of secondary medial meniscectomy (15.4%) was greater than that of secondary lateral meniscectomy (5.0%), in accordance with previous reports, and the success rates of MM and LM repair were greater than those in previous reports. We believe that the higher failure rate of medial meniscus (MM) repairs is due to biomechanical factors. The MM plays a crucial role in rotational stability and load sharing as the fixed meniscus, particularly in an athletic cohort where 194 (99.0%) patients engaged in pivoting sports.
Primary and revision ACLR combined with LEAP was recently shown to be associated with lower ACL graft failure rates than isolated ACLR29,35,39,49 in professional athletes.16,17 The decrease in failure rates is attributed to increased rotational stability and load sharing, which protect the ACL graft from excessive forces. 38 Furthermore, the increase in stability achieved by LEAP during ACLR is also associated with a significantly lower rate of failure after MM repair than that achieved via isolated ACLR. 48 Aligning with these previous findings, the percentage of patients who underwent LEAP in this series was high (74%); however, in this specific population, LEAP was not a protective factor for secondary meniscectomy.
Both the MM and the LM have their own specific functions, and repairing the meniscus is important for improving the clinical outcomes of ACLR. MM repair as a secondary stabilizer for anteroposterior translation has been demonstrated by several biomechanical cadaveric studies20,41,42 and leads to better integration of the ACL graft than meniscectomy.2,52 The importance of meniscal preservation also lies in avoiding the accelerated osteoarthritis seen in meniscectomy. Additionally, partial meniscectomy considerably increases the peak contact stress in the lateral compartment compared with the medial side. 43 Especially in athletes, rapid chondrolysis has been reported after partial lateral meniscectomy18,26,36,43 and refers to the rapid loss of articular cartilage in the lateral compartment, resulting in knee pain and persistent swelling. 36 In both menisci, a reoperation because of repair failure can lead to the above-mentioned consequences, as well as the delay in returning to play.
In recent years, there have been several reports regarding the prevalence of ramp lesions combined with ACL injury, which is as high as 42%.3,7,47 In the series by Magosch et al, 25 the percentage of ramp lesions among all MM tears combined with ACL injuries was 64.4% (67/104 patients). Farinelli et al 14 reported that the prevalence of ramp lesions combined with ACL injury in elite athletes was 14%. In the present study, the incidence of ramp lesions (84.6%) was much greater than that in previous reports. Ramp lesions are common but frequently underrecognized in ACL-injured knees, and the magnetic resonance imaging sensitivity for detecting ramp lesions is between 48% and 86%.12,44 As reported by Thaunat et al, 53 hidden lesions (type 3) can be found by dissecting the synovial tissue with a needle or shaver over the tear. To treat ACL injuries in professional athletes, probing with either a needle or an arthroscopy hook inserted through a posteromedial portal, as previously reported,50,53 is mandatory for recognizing ramp lesions. Furthermore, suture hook repair through a posteromedial portal is associated with a significantly lower secondary meniscectomy rate than is all-inside meniscal repair of ramp lesions performed at the time of ACLR, 15 and patients in the suture hook repair group who underwent an additional LEAP had significantly better meniscal repair survivorship than patients who did not undergo LEAP. 15 Our evaluation and treatment of ramp lesions could have contributed to the higher success rate of MM repair than that in previous reports.
Elite athletes face unique challenges due to the rigorous demands of their sports and the high expectations for returning to preinjury performance levels. We believe it is mandatory to advocate vigilance due to the high incidence of meniscal injury, especially ramp lesions, in this specific population and the clinical consequences of having underrecognized or undertreated lesions that can lead to delayed return to play or even worsening performance. Finally, future research should be focused on finding risk factors or repair technique improvements to decrease failure rates in meniscal repairs.
Limitations
This study has several limitations. First, it was a single-surgeon study, so the results may reflect the characteristics of the specific surgeon. However, the inherent consistency in technique that comes with a single-surgeon series helps decrease bias introduced by multiple techniques or multiple surgeons. Also, the study design was retrospective. Despite the inherent limitations of retrospective studies, this study benefits from a large sample size for this specific population; while large sample sizes cannot eliminate all biases inherent in retrospective studies, they significantly enhance the reliability and validity of the research findings. Furthermore, the possible etiology or size of the meniscal lesions was not reported, and only symptomatic meniscal repair failures were reported. Although it would have been interesting to study this, the relevant data were not recorded or available because of the retrospective study design. Third, this study did not include an assessment of functional outcomes or a comparison with a control group—for example, patients who underwent nonoperative treatment for meniscal lesions or tear debridement without repair. Fourth, the results of this study cannot be extrapolated to patients with ACL injuries who undergo nonoperative treatment, as they are not evaluated arthroscopically.
Conclusion
In this retrospective analysis of professional athletes with an ACL rupture, 85.2% (196/230) had meniscal lesions, with 37% having LM tears, 29% having MM tears, and 34% having lesions in both menisci. At long-term follow-up, the meniscal repair failure rate in this population of patients who underwent primary ACLR was 13.2% overall, 5% for LM tears and 15.4% for MM tears. No risk factors for secondary meniscectomy were found.
Footnotes
Final revision submitted July 3, 2024; accepted July 23, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Arthrex provided a research grant for the present study. GCS Ramsay Santé funds the scientific activity at the Centre Orthopédique Santy. B.S.-C. has received consulting fees and royalties from Arthrex and has stock in AREAS (cofounder). J.-S.A has received fellowship support from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from GCS Ramsay Santé (reference No. COS-RGDS-2024-01-002-SONNERY-COTTET-B).