
Abstract
Background:
Despite the posterior cruciate ligament (PCL) being an essential stabilizer of the knee, there is a paucity of data regarding injury management in pediatric patients.
Purpose/Hypothesis:
The purpose of this study was to evaluate differences in outcomes after operative (OP) versus nonoperative (NOP) management of pediatric isolated (single-ligament) PCL tears. It was hypothesized that managing PCL tears operatively would lead to improved functional outcomes compared with NOP management, especially in the setting of an associated meniscal tear.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Pediatric patients with an isolated PCL injury between 2006 and 2020 were identified and grouped according to whether they had a concomitant meniscal tear (PCL+M) or no meniscal tear (PCL-M). These cohorts were further sorted into OP, NOP, and nonoperative converted to operative (NOP2OP) treatment cohorts. Outcome data collected included Lysholm score, current activity level, and whether the patient returned to sports after treatment.
Results:
A total of 48 patients (49 knees) met study inclusion criteria (31 male, 18 female; mean age at injury, 15.6 years; age range, 8.3-18.9 years). There were 37 knees in the PCL-M cohort (30 NOP, 2 NOP2OP, and 5 OP) and 12 knees in the PCL+M cohort (4 NOP, 4 NOP2OP, and 4 OP). The mean duration of follow-up was 6.2 years (range, 2.4-15.7 years). The mean Lysholm scores were not significantly different between the OP and NOP knees in either the PCL-M cohort (P = .582) or the PCL+M cohort (P = .570); however, the PCL-M cohort overall had significantly higher scores compared with the PCL+M cohort (92.7 ± 13.0 vs 82.8 ± 18.8, respectively; P = .019).
Conclusion:
The pediatric patients in this series had similar functional outcomes when managed operatively or nonoperatively for their single-ligament PCL tear. When considering concomitant meniscal injury, the results indicated that children with meniscal injury had a worse outcome than those without a meniscal injury. Shared decision-making with patients and their family should take these results into consideration.
Isolated (single-ligament) posterior cruciate ligament (PCL) injuries in the pediatric population have not been fully studied to evaluate appropriate management. Current management of isolated PCL injuries is based predominantly on literature pertaining to adult-aged patients or is otherwise complicated by findings related to the injury not being single ligament.6-8 In adults, the long-term degeneration and outcomes of a PCL-deficient knee are related to the pattern of instability (unilateral vs multidirectional). 12 PCL-deficient knees with unilateral instability are known to do well clinically, while PCL-deficient knees with multidirectional instability have poorer functional outcomes. The early studies on isolated PCL injuries suggest that nonoperative (NOP) management may have good outcomes.5,7 However, some authors have suggested that young athletic patients need to have this injury reconstructed every time. 9 None of these previous studies have elucidated risk factors for poor outcomes with isolated PCL injury; they have only highlighted the need for reconstruction when multiple ligaments are involved or repair when a bony avulsion is present.7,12
The most comprehensive study regarding the treatment of PCL injuries in a pediatric population was conducted by Kocher et al 8 and was aimed at determining if surgical management was safe and effective in children. It was not designed to help guide whether or not surgery was superior to NOP management. Those authors identified their cohort based on the presence of other concomitant injuries that would influence the decision for surgery and against NOP management. Consequently, the question of whether surgery can be safely performed in the pediatric population was answered, but not the question regarding when a child/teenager should be managed with PCL reconstruction. With evidence in the adult population that NOP management can be appropriate in the right patient, there is a need to identify which factors may indicate improved outcomes with surgery in the pediatric population.
In the current study, we evaluated patients who underwent operative (OP) and NOP management of pediatric isolated (single-ligament) PCL tears. The primary aim of the study was to compare the patient-reported outcome scores and success in return to full activity between the 2 management cohorts. The secondary aim was to determine if the presence of a meniscal tear affects functional outcomes after either type of management, thereby starting the process of identifying indications for surgical intervention. Our hypothesis was that patients with PCL tears managed surgically would have improved functional outcomes compared with those who underwent NOP management.
Methods
The institutional review board (IRB) reviewed and approved this study and determined that written consent was not required. After receiving IRB approval for the study protocol, we retrospectively generated a list of potential patients seen in the orthopaedic clinic between 2006 and 2020 using the following International Classification of Diseases, 9th and 10th Revision codes: 844.2 (sprain of cruciate ligament–knee), 905.7 (late effect of sprain/strain without mention of tendon injury), and S83.521A (sprain of PCL). We also used the following Current Procedural Terminology code: 29889 (to cross-reference the lists). Included were patients aged <20 years with a PCL tear. Exclusion criteria were then applied as indicated in Figure 1. We defined an isolated PCL tear as a discrete injury to that ligament (complete tear [or high-grade injury] or avulsion injury verified on magnetic resonance imaging [MRI]), with only low-grade tears to other ligamentous structures in the knee, if present (Figures 2 and 3). Low-grade concomitant ligamentous injuries in this study were defined by a noncomplete rupture on MRI and not requiring surgical reconstruction. In total, 6 orthopaedic providers managed patients with PCL injuries during this period, with 3 surgeons completing operations.

Flowchart showing patient exclusion process.

Magnetic resonance imaging scans from a 14.3-year-old male patient who injured his knee playing basketball: (A) intact anterior cruciate ligament and (B) injured posterior cruciate ligament (PCL). This patient was treated with arthroscopic PCL reconstruction with anterior tibialis allograft and had a Lysholm score of 100 at the 24.7-month follow-up.

Magnetic resonance imaging scans from a 13.8-year-old female patient who injured her knee playing soccer: (A) intact anterior cruciate ligament and (B) injured posterior cruciate ligament. This patient was treated nonoperatively and had a Lysholm score of 95 at the 46.5-month follow-up.
A retrospective review was performed, and basic patient information was collected for this study: age, duration from injury to first visit and surgery, mechanism of injury, physeal status (open/closed), preferred sport, ethnicity, and sex. Complications, revisions, and Lysholm score (a 100-point scale consisting of 8 domains: limp, support, locking, instability, pain, swelling, stair-climbing, and squatting 11 ) were also obtained from chart review. Standard of practice for our group is to maintain contact with patients having cruciate ligament injuries for a minimum of 2 years, with the timeline distant visits often being a telephone encounter rather than an in-person visit. Physeal status was evaluated on plain radiograph and/or MRI scan. One patient had the radiographic evaluation performed at an outside institution, and the examinations were not uploaded into our medical record system; this patient was excluded from reports on physeal status. At the final encounter, patients were asked to report whether they returned to sport after treatment, and this was recorded categorically as yes or no. The presence or absence of a concomitant meniscal tear was also recorded.
Management Choice and Protocol
Patients were indicated for an OP or NOP treatment course based on the outcome of shared decision-making between the patient's family, the patient, and the surgeon. Nonsurgical patients were treated with a course of physical therapy and were offered a dynamic functional knee brace. The goal of physical therapy was to reduce postinjury swelling; increase quadriceps, hip, and core strength; and improve proprioception. They were allowed to progress back to activity as tolerated with no activity restrictions, often at 6 to 12 weeks postinjury. The recommendation for PCL functional bracing during activity was without an endpoint, and a single time point recording of bracing use (yes/no) was recorded; however, the true duration of use for each patient was not recorded. Failure of NOP management was recorded if a patient continued to complain of pain or instability. At that time, surgical intervention was offered.
The management protocol for surgical patients varied slightly based on the pathology present. If the PCL injury was an avulsion fracture, then it was managed via open reduction and internal fixation of the fragment or arthroscopy-assisted reduction and internal fixation. These injuries were immobilized for 4 weeks in extension to allow early callus formation before physical therapy was initiated. If the PCL injury was a ruptured midsubstance ligament, then it was managed via reconstruction using an allograft of appropriate size for the patient and early initiation of physical therapy (starting with postoperative week 1 or 2). A range of motion brace was used until the effusion resolved and the patient could successfully complete a straight-leg raise. The patient was then transitioned into either a knee sleeve or a PCL dynamic functional brace for at least a year after surgery but without a defined endpoint and without documented compliance for each patient. In both surgical groups, once physical therapy began, patients followed a range of motion, knee stabilization, and muscle strengthening protocol with similar stages to those after anterior cruciate ligament reconstruction, including seeking clearance for sport after 6 months.
Study Cohorts and Statistical Analysis
Each of the patients who met criteria were then placed in 2 cohorts: those with a concomitant meniscal tear (PCL+M) and those with no concomitant meniscal tear (PCL-M). These 2 cohorts were then further sorted into OP, NOP, and nonoperative converted to operative (NOP2OP) treatment cohorts. NOP2OP included patients undergoing surgery after persistent instability or pain after NOP management.
Basic descriptive statistics are reported. Continuous data were analyzed for normality using the Shapiro-Wilk test of normality. All continuous data reported in this study were found to be nonnormally distributed and were evaluated with the Mann-Whitney U test. Categorical data were evaluated with the Fisher exact test, and odds ratios were calculated manually if a significant relationship was found with the Fisher exact test. The knee was used as the unit of analysis. All analysis was performed using SPSS (Version 26; IBM Corp). Statistical significance was defined as P < .05. No a priori power analysis was performed.
Results
A total of 49 knees in 48 patients met criteria for this study, accounting for 89% with 2-year follow-up. Cohort characteristics are presented in Table 1. A total of 35 knees (71.4%) had sports-related injuries, with the most common sports being football (n = 8, 16.3%), baseball (n = 7, 14.3%), and soccer (n = 5, 10.2%). Non–sports-related injuries included falls from height (n = 3), rollerblade/skateboard (n = 4), all-terrain vehicle/motorcycle crashes (n = 1), motor vehicle accident (n = 2), horseplay (n = 2), and pedestrian hit by automobile (n = 2). The mean follow-up duration was 6.2 years (range, 2.4-15.7 years). Of 34 patients treated entirely nonoperatively, 15 (44.1%) reported using the functional knee brace during activity as prescribed. The patients with open physes (n = 19) had a Lysholm score of 96.7 ± 5.6 as compared with 85.8 ± 17.9 for patients with closed physes (n = 29) (P = .013).
Characteristics of the Study Cohort (N = 49 Knees, 48 Patients) a

Data are reported as mean ± SD (range) or No. of knees (%) unless otherwise indicated. PCL, posterior cruciate ligament.
1 patient did not have available images, only a report without mention of physeal status.
There were 37 PCL-M knees with intent to treat as follows: 32 NOP and 5 OP. Two of the NOP knees failed NOP management and were converted to PCL reconstruction (2/32, 6.3%). Details regarding conversion can be found in Table 2. There were 12 PCL+M knees with intent to treat as follows: 8 NOP and 4 OP. Of the 12 PCL+M knees, 3 had medial meniscal repairs while the PCL was managed nonoperatively, 3 had meniscal repairs simultaneous with PCL reconstruction, 2 had a meniscectomy simultaneous with PCL reconstruction, and 1 knee had a meniscectomy simultaneous with PCL reconstruction. One knee had PCL reconstruction while the meniscus was treated nonoperatively, 1 knee had both the meniscus and PCL treated nonoperatively, and 1 knee had meniscal repair initially and then underwent PCL reconstruction 1 year later.
Nonoperative to Operative Conversion a

F, female; M, male; PCL, posterior cruciate ligament; PCL+M, posterior cruciate ligament with concomitant meniscal tear; PCL-M, posterior cruciate ligament without concomitant meniscal tear; PCLR, posterior cruciate ligament reconstruction; PT, physical therapy.
Patient was noncompliant with PT by not attending PT and continuing to play volleyball.
One 16.8-year-old male patient injured his knee while wrestling. He was treated with PCL reconstruction including femoral Endobutton (Smith & Nephew) graft fixation and a suspensory interference screw for tibial fixation. The patient required a revision procedure 7 weeks later because of failed tibial fixation after noncompliance with standard activity modifications after his procedure. No other complications were reported for either the OP or NOP cohort.
Seven of the 37 knees (18.9%) in the PCL-M cohort were managed surgically compared with 8 of the 12 knees (66.7%) in the PCL+M cohort (P = .004). Lysholm scores were not significantly different between the OP and NOP knees in either the PCL-M cohort (P = .582) or the PCL+M cohort (P = .570); however, the PCL-M cohort overall had significantly higher scores than the PCL+M cohort (92.7 ± 13.0 vs 82.8 ± 18.8, respectively; P = .019). Further details are highlighted in Table 3. Combining the 2 treatment cohorts, we found that knees initially treated nonoperatively (n = 40) with a meniscal injury (n = 8) were 15 times more likely (95% CI, 2.1-110.0) to fail NOP treatment and convert to OP management than knees without an associated meniscal tear (P = .01).
Outcomes of Interest According to Study Groupings a

Data are reported as mean ± SD (range). PCL+M, posterior cruciate ligament with concomitant meniscal tear; PCL-M, posterior cruciate ligament without concomitant meniscal tear. Boldface values indicate significant differences.
Of the 35 knees with sports-related injuries, 29 (82.9%) reported returning to their sport. Of 26 such knees in the PCL-M cohort, 24 returned to sport, and 5 of 9 knees in the PCL+M cohort returned to sport (P = .027). Within the PCL+M cohort, 2 of 3 knees (66.7%) with sports-related injuries returned to sport when managed nonoperatively, while 3 of 6 (50.0%) managed operatively returned to sport (P > .99). In the PCL-M cohort, 21 of 22 knees (95.5%) with sports-related injuries returned to sport when managed nonoperatively and 3 of 4 (75.0%) when managed operatively (P = .289).
The Lysholm scores in Table 4 demonstrate that there were varied outcomes for these crossover patients depending on injury status of the meniscus. Patients with isolated PCL injury (PCL-M) had similar results between all 3 management cohorts (OP, NOP, NOP2OP), indicating there is no long-term detriment to opting for initial NOP management, as conversion to surgery resulted in similarly positive outcomes. However, in the PCL+M group, the 4 NOP2OP crossover patients had significantly lower scores than the OP patients (P = .029) and similar scores to the NOP patients (P = .2).
Lysholm Scores of Patients Who Converted From Nonoperative to Operative Management a
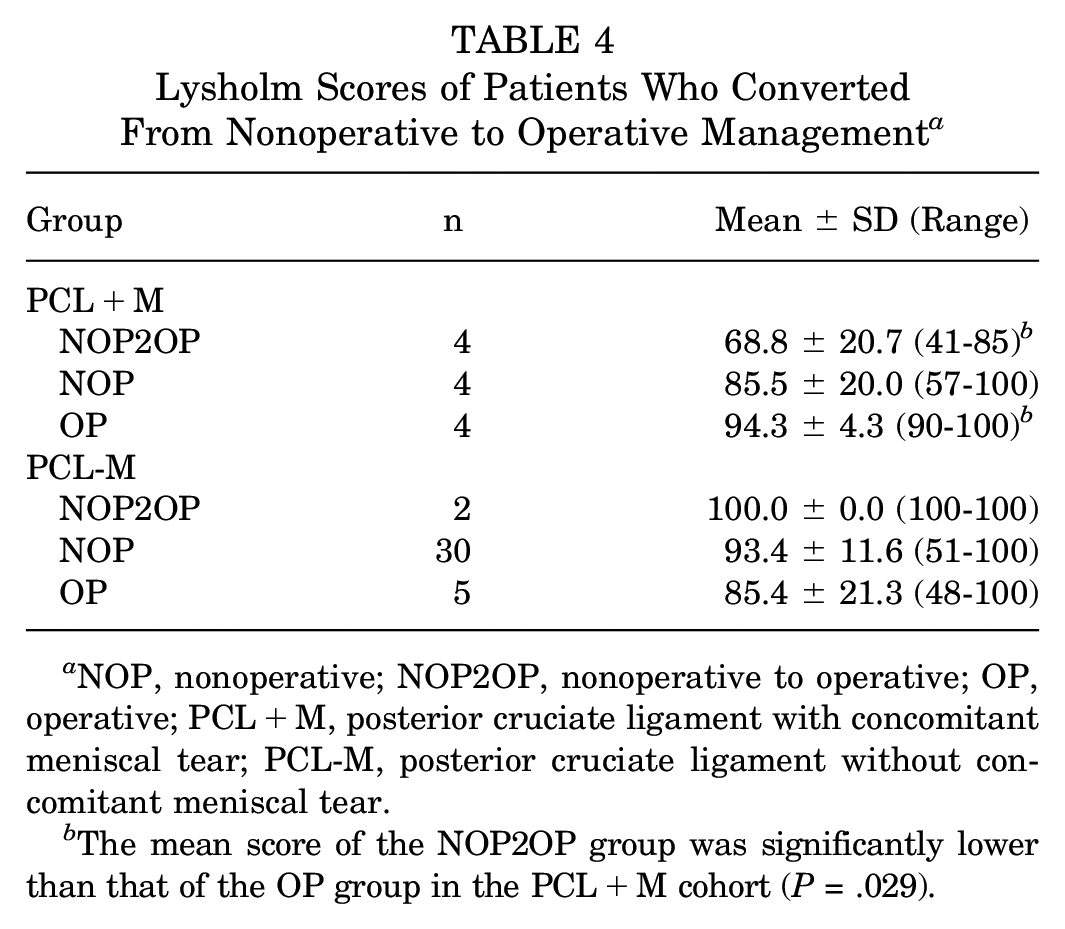
NOP, nonoperative; NOP2OP, nonoperative to operative; OP, operative; PCL+M, posterior cruciate ligament with concomitant meniscal tear; PCL-M, posterior cruciate ligament without concomitant meniscal tear.
The mean score of the NOP2OP group was significantly lower than that of the OP group in the PCL+M cohort (P = .029).
Discussion
The results of the current study suggest that NOP and OP management of PCL injuries in the pediatric and adolescent population are both safe and effective with reproducible functional results. Specifically, patients had positive Lysholm scores when managed both nonoperatively (92.5 ± 12.7) and operatively (85.3 ± 18.9). Additionally, 29 of 35 knees (82.9%) were able to return to sport, with 24 of 26 (92.3%) in the PCL-M cohort and 5 of 9 (56%) in the PCL+M cohort. The patients in the PCL-M group had better functional outcomes, with a Lysholm score of 92.7 ± 13.0 compared with 82.8 ± 18.8 in the PCL+M group (P = .019). Lastly, patients initially treated nonoperatively with a meniscal injury were 15 times more likely to fail NOP treatment and be converted to OP management than patients without an associated meniscal tear (P = .01).
Given the above findings, both OP and NOP treatment options can be presented to the patient and their families for consideration. With low complication rates in either management cohort, it appears that our hypothesis is refuted with evidence that single-ligament, or isolated, PCL injury in pediatric athletes can be successfully managed with either surgery or NOP treatment. The presence of a concomitant meniscal injury did not shift the outcome between OP and NOP management of PCL injury in this youthful population.
There are limited historical findings regarding the management of children and adolescents with PCL tears, with the vast majority of evidence in this population only being included as part of a larger sampling of an older, adult population, as the mean ages for these previous studies are all over the age of 21 years.3-5,10,12 There are 2 case reports involving a pediatric patient with a PCL injury; however, because of the nature of the study type, the results cannot be extrapolated to a larger series of patients.1,2 The only publication addressing this young cohort in isolation was performed to determine the safety of doing surgery in adolescents with a PCL injury. 8 In contrast to that study, our patient population included only patients who would not automatically be indicated for surgery because of their other concomitant injuries. Therefore, our study represents injury patterns in which the PCL injury itself (rather than other associated ligamentous insufficiency) would be the main indication for surgery. Although only 39.6% of the patients in our study had open physes at the time of injury, this is the best representation of the skeletally immature population in the literature on PCL management to date. The patients with open physes had better Lysholm scores than those with closed physes, suggesting that skeletally immature patients tend to have better outcomes across all treatment groups. There was insufficient power to subanalyze the patients based on physeal status within each treatment cohort.
In comparison with the previous literature, we also found that surgical management of PCL injuries in this youthful population is relatively safe, with only 1 complication in the OP cohort and no complications in the NOP cohort. It is important to note that 4 of 8 patients in the PCL+M group failed NOP management and required surgery, while 2 of 32 were converted in the PCL-M group.
A study conducted on the long-term effects in adult patients with PCL-deficient knees found that degeneration of the articular surfaces varied at all time points, with some patients reporting fairly normal function and others reporting significant deterioration. 3 No factors in that study were found to be the definitive cause of the differences in outcomes of PCL-deficient knees, although all their patients were male, and our study included a mix of sexes. The current study also contradicts the previous claims that PCL injuries should be immediately reconstructed in young athletic individuals, 9 as the outcomes for the NOP cohort appear to be no different from those seen in the surgical cohort, with similar return-to-sport rates.
Limitations
This study was limited by its small sample size and retrospective nature. A larger sample size may have captured additional failures in both the NOP and the surgical cohorts. Because of the small sample size of this crossover cohort, the power of this crossover subanalysis is not high enough to make strong claims about conversion to surgery, but it is worth noting this comparison. Additionally, our study focused on outcome questionnaires rather than any clinical or radiographic examination findings. However, we did achieve an 89% follow-up rate at our requisite duration of follow-up, which included the outcome questionnaire. The study also was limited by the patients having a heterogeneous mix of skeletal maturity and grade of PCL injury. A final limitation that could not be rectified owing to the retrospective nature of the study was the inability to evaluate the duration or time in the braces or sleeves that was prescribed for the patients, only that they were prescribed or recommended. Therefore, the outcomes related to physical therapy or brace use cannot be extrapolated fully.
Conclusion
The study outcomes demonstrated no significant differences (statistically or clinically) in Lysholm scores when comparing surgical and NOP management of isolated PCL tears. Moreover, even though a concomitant meniscal injury tended to predict a lower outcome score overall, our secondary aim failed to identify the presence of concomitant meniscal tear as a factor that could shift the risk-benefit ratio for performing surgery over NOP management of PCL tears. However, there did appear to be a higher risk for converting from NOP to OP management when a meniscal tear is present. Shared decision-making with patients and their family should take these results into consideration, and until longer-term outcome studies can demonstrate a difference between management choice, we will continue to emphasize the success of NOP management for our pediatric patients with single-ligament (isolated) PCL tears.
Footnotes
Final revision submitted August 1, 2023; accepted August 10, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.T.P. has received education payments from ImpactOrtho and SportsTek Medical and consulting fees from OrthoPediatrics. E.W.E. has received nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of California, San Diego (reference No. 192008).