
Abstract
Background:
The incidence of anterior cruciate ligament reconstruction (ACLR) graft failure is inversely related to the diameter of the ACLR graft. When the diameter of a 4-stranded hamstring tendon graft with a doubled semitendinosus and doubled gracilis tendon (ST×2 + G×2) configuration is <8 mm, the gracilis tendon is often thin.
Hypothesis:
(1) The diameter of the doubled semitendinosus tendon (ST×2) alone would be able to predict the probability of a 4-stranded ACLR graft having a diameter of ≥8 mm, and (2) there would be a specific cutoff value for the ST×2 diameter such that the addition of a doubled gracilis tendon (G×2) will not result in a 4-stranded graft with a ≥8-mm diameter.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Included were patients who had undergone 4-stranded hamstring ACLR between 2008 and 2018. Patients were excluded if the diameter measurements of the tendons or ACLR graft were missing. A receiver operating characteristic (ROC) analysis was performed to assess the predictability of ST×2 on an ACLR graft with a diameter of ≥8 mm. The effect of including G×2 on the final graft size was reported.
Results:
A total of 314 patients were included, and the mean diameters of ST×2 and G×2 were 6.5 ± 0.8 mm and 5.0 ± 0.7 mm, respectively. There was a moderate to strong correlation between the diameter of ST×2 and that of G×2 (men: r = 0.678; women: r = 0.654; P < .001 for both). An ST×2 with a diameter <6 mm predicted a 4-stranded ACLR graft of <8 mm (area under the ROC = 0.917; P < .001). When ST×2 was <6 mm, the addition of a G×2 did not result in the ACLR graft's having a diameter of ≥8 mm, regardless of patient sex or G×2 diameter.
Conclusion:
When the diameter of the doubled semitendinosus was <6 mm, the addition of the doubled gracilis was unlikely to produce a 4-stranded ACLR graft with a diameter of ≥8 mm. Surgeons should consider alternative methods such as tripling or quadrupling the semitendinosus tendon to increase the size of the ACLR graft, rather than routinely harvesting the gracilis tendon.
The medial hamstring tendon autograft is a commonly used graft in anterior cruciate ligament reconstruction (ACLR). 2 The majority of surgeons harvest both the semitendinous and the gracilis tendons simultaneously and prepare the ACLR graft as a 4-stranded graft with a doubled semitendinosus tendon and a doubled gracilis tendon (ie, the “ST×2 + G×2” configuration). 16 The advantage of preparing the graft this way is that the length of the resultant ACLR graft is always long enough to allow the use of all types of fixation methods available in the market, including both aperture fixation and suspensory fixation. The diameter of the resultant 4-stranded graft is influenced by several anthropometric factors of the patient, including body height, body weight, and sex. Short and thin patients are more likely to have a 4-stranded graft with a smaller diameter than taller and heavier individuals.9,11,18
The incidence of ACLR graft failure is inversely related to the diameter of the ACLR graft.3,7,17 A graft diameter of <8 mm has been reported to be associated with a higher incidence of ACLR graft failure 3 and revision ACLR. 17 The percentage of 4-stranded hamstring tendon grafts in the ST×2 + G×2 configuration with a diameter of <8 mm has ranged from 5.8% to 16.9% in White patients11,16 and 43% to 77% in Asian patients, respectively.8,15 During clinical practice, the diameter of the 4-stranded graft is often known only after both the semitendinosus and gracilis tendons are harvested and the 4-stranded graft is prepared. Additionally, if the configuration of the 4-stranded graft is not changed, there is little a surgeon can do to increase the size of the ACLR graft.
The diameter of the gracilis tendon is known to be smaller than that of the semitendinosus tendon. 20 It is not uncommon to observe that the gracilis tendon is very thin when the diameter of the entire 4-stranded ACLR graft is <8 mm. It has been reported that the inclusion of the thin gracilis tendons into the 4- or 5-stranded graft as additional tissue does not significantly change the final graft size. 16 However, despite knowing that the final graft size will not be significantly increased, a majority of surgeons include the gracilis tendon into the final construct of the ACLR graft, as it has already been harvested.
It would be helpful to have a method to predict the size of the 4-stranded hamstring ACLR graft and eliminate the need to harvest an exceptionally thin gracilis tendon. Attempts have been made to predict this diameter through regression analysis of anthropometric factors9,18 or preoperative imaging results. 13 However, these methods are not routinely employed in ACLR. Furthermore, these methods have been unable to predict whether the addition of the gracilis tendon into the final ACLR graft construct is helpful in increasing the diameter of the graft to ≥8 mm.9,13,18
The dimensions of the semitendinosus tendon and gracilis tendon are correlated with similar sets of anthropometric data, including body height, body weight, and sex.4,6,15,20 It is likely that the diameter of the semitendinosus tendon is correlated with that of the gracilis tendon, and the diameter of the harvested semitendinosus tendon alone can be used to predict the size of the final 4-stranded ACLR graft, even before the harvesting of the gracilis tendon.
Thus, the aim of this research was to minimize the need for unnecessary harvesting of a thin gracilis tendon. It was hypothesized that the diameter of the doubled semitendinosus tendon (ST×2) by itself would be able to predict the probability of a 4-stranded hamstring ACLR graft having a diameter of ≥8 mm. Furthermore, it was hypothesized that there would be a specific cutoff value for the ST×2 diameter such that the addition of a doubled gracilis tendon (G×2) will not result in a 4-stranded graft with a ≥8-mm diameter.
Methods
The local ethics committee of the author's institute approved the current study; the requirement for obtaining informed consent from the participants was waived by the ethics committee. A retrospective study was conducted using prospectively collected data on patients who underwent medial hamstring harvesting between January 2008 and December 2018. Patients were excluded if there were graft harvesting complications, including premature amputation of the harvested tendon. Graft harvesting complications can result from technical errors or situations where harvesting is difficult, such as the presence of a sizable exostosis in the medial proximal tibia. Patients were also excluded if data regarding the diameter of the harvested medial hamstring or the ACLR graft were not available due to data entry issues. The criteria for including and excluding participants are outlined in Table 1.
Study Inclusion and Exclusion Criteria a

ACLR, anterior cruciate ligament reconstruction.
Harvesting the Medial Hamstring Tendon Autograft
The harvesting of the medial hamstring tendon graft was performed using an anterior approach at the time of ACLR. The patient was placed in a supine position on the operating table and administered general anesthesia with muscle relaxants. A pneumatic tourniquet was applied to the proximal thigh. With the knee flexed at 90°, a longitudinal incision was made on the anteromedial aspect of the medial proximal tibia at the level of the tibial tuberosity. The subcutaneous tissue was dissected until the sartorial fascia was reached, and the semitendinosus and gracilis tendons were identified through palpation. An L-shaped incision was made in the sartorial fascia, and the combined insertion of the medial hamstring was sharply dissected from its attachment on the medial proximal tibia. The semitendinosus and the gracilis tendons were separated from the sartorial fascia, and the graft was harvested from the proximal end using a closed tendon stripper. The surgeon recorded in a prospective data collection form whether graft harvesting complications, such as premature amputation of the tendon, occurred or not. The surgical procedures were performed by 1 of the 2 fellowship-trained sports medicine surgeons, one of whom was the study author (W.P.Y.).
Measurement of Tendon Diameter
The harvested semitendinosus or gracilis tendon was prepared on a side table with the removal of all muscle. The tendon was first doubled by folding it directly in half, and the diameter of the doubled harvested tendon (ie, either ST×2 or G×2) was measured using a graft sizer with diameter sizes ranging from 4.5 to 12 mm in 0.5-mm increments (Smith & Nephew) (Figure 1). The size of the doubled tendon was determined as the smallest diameter on the graft sizer that allowed passage of the tendon under maximal manual tension. If the doubled tendon could easily pass through the smallest of the graft sizer holes (4.5 mm) without resistance, the diameter was recorded as <4.5 mm. The ACLR graft was then prepared, and the diameter of the entire graft (ST×2 + G×2) was measured using the graft sizer.

Graft sizer used to measure the diameter of the doubled harvested tendons and the 4-stranded anterior cruciate ligament reconstruction graft.
Statistical Analysis
The diameters of ST×2, G×2, and the 4-stranded ACLR graft were reported as means with standard deviations. A comparison of the ST×2 diameter versus G×2 diameter was performed using the paired t test, with mean difference, 95% CI, and Cohen d effect size calculated. The association between the diameters of ST×2 and G×2 was examined using Pearson correlation analysis. The strength of the association was classified as perfect if the correlation coefficient (r) was 1, strong if it ranged from 0.7 to 0.9, moderate if it ranged from 0.4 to 0.6, and weak if it ranged from 0.1 to 0.3. A P value of <.05 was considered statistically significant.
A receiver operating characteristic (ROC) analysis was performed to investigate the relationship between the diameter of ST×2 and the diameter of the 4-stranded ACLR graft. The area under the ROC curve (AUC) was interpreted as indicating excellent discrimination if >0.9 and acceptable discrimination if between 0.8 and 0.9. In addition, the cutoff value for an ST×2 diameter that predicts a 4-stranded ACLR graft with a diameter of ≥8 mm was calculated with odds ratio (OR) and 95% CI. Sensitivity, specificity, positive predictive value, and negative predictive value were also reported. Finally, the effect of including G×2 on the final graft size having a diameter of ≥8 mm was also calculated.
Power Analysis
The mean diameter of 4 strands of the semitendinosus and 4 strands of the gracilis tendon was reported as 7.4 ± 0.7 mm and 5.9 ± 0.6 mm, respectively, according to Xie et al. 20 A power analysis was conducted to test the null hypothesis that there was no correlation between the diameter of ST×2 and the diameter of G×2, with alpha set at .05 and power set at 0.8. The calculation was based on a 2-tailed test. In order to detect a correlation coefficient of ≥0.3, a minimum of 84 patients was required.
Results
Out of 325 eligible patients, 314 patients satisfied the inclusion and exclusion criteria (Figure 2). There were 237 men and 77 women, with a mean age of 27.3 ± 8.3 years.

Flowchart showing the enrollment of study patients. ACLR, anterior cruciate ligament reconstruction.
Correlation Between the Diameters of the Doubled Semitendinosus Tendon and the Doubled Gracilis Tendon
The mean diameters of the tendons were 6.5 ± 0.8 mm for ST×2 and 5.0 ± 0.7 mm for G×2. There was a moderate to strong positive association between these diameter measurements, regardless of patient sex (men: r = 0.678; women: r = 0.654; P < .001 for both). The diameter of ST×2 was significantly larger than that of G×2 (P < .001; paired t test). The mean difference between ST×2 and G×2 diameters was 1.5 ± 0.6 mm (95% CI, 1.4-1.5 mm; Cohen d = 2.5), and 22% of patients had a G×2 with a diameter <4.5 mm, compared with 0% for ST×2 (P < .001; Fisher exact test) (Figure 3).

Comparing the distribution of the doubled harvested tendon diameters among the study patients.
The diameter of G×2 increased with an increasing diameter of ST×2. The proportion of patients having a G×2 diameter that was <4.5 mm was 61%, 41%, and 6% when the diameter of ST×2 was 5 mm, 6 mm, and 7 mm, respectively (Table 2).
Relationship Between the Diameters of the Doubled Semitendinosus Tendon and Doubled Gracilis Tendon in the Study Patients (N = 314) a

Dashes indicate no patients fell into that category. G×2, doubled gracilis tendon; ST×2, doubled semitendinosus tendon.
Diameter of 4-Stranded ACLR Graft
The diameter of the 4-stranded ACLR graft was 8.2 ± 0.9 mm (range, 6-11.5 mm) (Figure 4). The diameter of the graft was ≥8 mm in 65.9% of the patients.

Distribution of the 4-stranded ACLR graft diameter among the study patients. ACLR, anterior cruciate ligament reconstruction.
Results of ROC Analysis
The results of the ROC analysis on the relationship between the diameter of ST×2 and the diameter of the 4-stranded ACLR graft with a diameter of ≥8 mm (Figure 5). The under the ROC curve was 0.917 (P < .001), indicating excellent discrimination.

Sensitivity and specificity of the doubled semitendinosus tendon diameter (ST×2) in predicting a 4-stranded ACLR graft with ≥8-mm diameter. ACLR, anterior cruciate ligament reconstruction
When the diameter of ST×2 was <6 mm, the diameter of the ACLR graft was always <8 mm (P < .001; OR, 3.96; 95% CI, 3.23-4.85) (Table 3). The sensitivity, specificity, positive predictive value, and negative predictive value of an ST×2 with a diameter of <6 mm leading to a 4-stranded graft of <8 mm was 34.6%, 100%, 100%, and 74.7%, respectively.
Relationship Between the Cutoff Value of the Diameter of the Doubled Semitendinosus Tendon and the Diameter of the ACLR Graft a
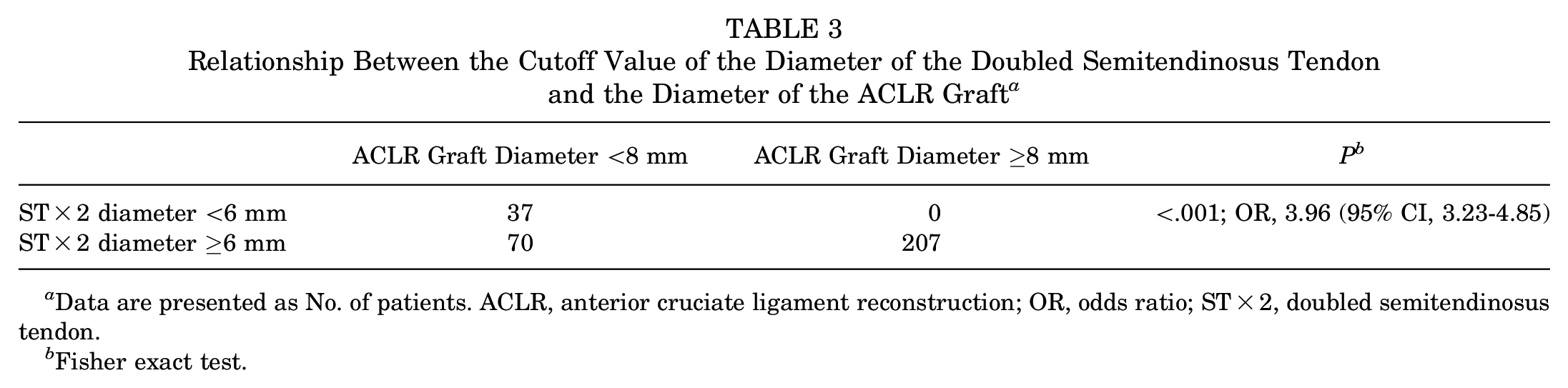
Data are presented as No. of patients. ACLR, anterior cruciate ligament reconstruction; OR, odds ratio; ST×2, doubled semitendinosus tendon.
Fisher exact test.
The effect of adding a G×2 to the ST×2 on the odds of the resultant 4-stranded grafts having a diameter of ≥8 mm is reported in Table 4. When the measured diameter of the ST×2 was <6 mm, the addition of a G×2 did not result in an ACLR graft with a ≥8 mm diameter, regardless of patient sex or the diameter of the G×2.
Relationship Between the Diameter of the Doubled Semitendinosus Tendon and the Percentage of 4-Stranded ACLR Grafts Having a Diameter of ≥8 mm a

Dashes indicate areas not applicable. ACLR, anterior cruciate ligament reconstruction; GT×2, doubled gracilis tendon; ST×2, doubled semitendinosus tendon.
Discussion
The most important finding of this study was that the diameter of a doubled semitendinosus tendon alone can be used to predict whether the resultant ACLR graft can have a diameter of ≥8 mm, even without the information about the diameter of the gracilis tendon. This provides the opportunity to avoid harvesting the gracilis tendon if its addition does not result in a clinically important change in the size of the resultant ACLR graft.
A moderate to strong positive association was found between the diameter of the doubled semitendinosus tendon and that of the doubled gracilis tendon (men: r = 0.678; women: r = 0.654; P < .001 for both). When the diameter of the doubled semitendinosus tendon was <6 mm, the further addition of the doubled gracilis tendon did not result in a 4-stranded ACLR graft with a minimum diameter of 8 mm; this was true regardless of patient sex or the diameter of the doubled gracilis tendon. Surgeons should consider alternative methods to increase the size of the final ACLR graft, such as tripling or even quadrupling the semitendinosus tendon. If it is found that tripling or quadrupling the semitendinosus tendon can result in an ACLR graft with a diameter of ≥8 mm, the surgeon can consider not harvesting the gracilis tendon.
The focus of the literature on the use of the medial hamstring as a graft for ACLR is on the influence of anthropometric factors on the diameter of the resultant 4-stranded ACLR graft.9,11,12,14,18,19 The majority of the reported data on the diameter and area of the medial hamstring come from measurements using preoperative magnetic resonance imaging (MRI). 13 There are only a few studies in the literature reporting the diameter of both the semitendinosus tendon and the gracilis tendon through intraoperative measurements.4,6,15,20 The author is not aware of any publication reporting a significant correlation between the diameter of the semitendinosus tendon and the diameter of the gracilis tendon, although this relationship seems apparent. The current study confirms that a moderate to strong correlation exists between the diameter of these 2 tendons. Hence, the size of the semitendinosus tendon alone can be used to predict that of the gracilis tendon and the resultant ACLR graft prepared in an ST×2 + G×2 configuration.
The diameter of the ACLR graft can be increased by increasing the number of strands of hamstring tendon used to construct it.12,14,19 Nazari et al 14 measured the diameter of ACLR grafts prepared using 4 different graft configurations, including 3-stranded (ST×3), 4-stranded (ST×2 + G×2), 5-stranded (ST×3 + G×2), and 6-stranded (ST×3 + G×3). They found that only 19% of the 4-stranded ACLR grafts with the ST×2 + G×2 configuration had a minimum diameter of 8 mm. Despite increasing the number of hamstring tendon strands in the ACLR graft construct, 17% to 31% of the ACLR grafts composed of 3 strands of the semitendinosus tendon and 2 strands of the gracilis tendon (ST×3 + G×2) did not have a minimum diameter of 8 mm. 14 In a study of 1681 ACLRs, Ramkumar et al 16 showed using multiple regression analysis that the addition of a third strand of semitendinosus by tripling the tendon significantly increased the ACLR graft diameter; on the other hand, the inclusion of thin gracilis tendons into a 4- or 5-stranded graft as additional tissue did not significantly change the final graft size.
Harvesting of the medial hamstring can be associated with complications.1,10 Flexion strength deficits and reduction in active flexion of the knee are common. 10 Although the majority of flexion strength deficits are transient, a persistent shift of peak torque angle to the shallow angle and a reduction of flexion angle have been observed at a follow-up of 2 years after surgery, which can affect athletes who are required to flex their knees deeply and powerfully in their performance. 1 Thus, if it is known that the addition of gracilis tendon to the ACLR graft will not result in a clinically important change in the final graft size, the gracilis tendon should not be harvested to minimize the chance of these complications.
Recognizing the relative contribution of the semitendinosus tendon and gracilis tendon to the final graft size, some surgeons routinely harvest only the semitendinosus tendon and triple or even quadruple it to form the ACLR graft, while leaving the gracilis tendon intact. 5 However, this practice results in a short ACLR graft, which requires the use of suspensory fixation on both the femoral and the tibial sides. Additionally, neither tripling nor quadrupling the semitendinosus tendon alone always yields a long and large enough ACLR graft. According to Nazari et al, 14 only 27% of grafts prepared by tripling the semitendinosus alone have a diameter of ≥8 mm. Janssen et al 11 found that the length of the semitendinosus was not always sufficient for quadrupling. The minimum length of the semitendinosus for tripling and quadrupling was suggested to be 210 mm and 280 mm, respectively. The length of the semitendinosus was shorter than 280 mm in ≥32% of patents in that study, making quadrupling semitendinosus an infeasible method for all patients. 11
The results of this study provide additional information on whether the inclusion of the gracilis tendon can result in an ACLR graft with a diameter of ≥8 mm and facilitate the surgeon's decision on whether to harvest the gracilis tendon. The most important anthropometric factor predicting the diameter of a 4-stranded ACLR graft is body height. 18 When a short patient is scheduled to have an ACLR using hamstring tendon autograft, the surgeon can consider harvesting only the semitendinosus tendon initially. If the diameter of the doubled semitendinosus tendon is found to be <6 mm, the inclusion of a doubled gracilis tendon to it is unlikely to result in a 4-stranded ACLR graft with a diameter of ≥8 mm. Alternative methods to increase the size of the graft, such as tripling or quadrupling the semitendinosus graft, harvesting the semitendinosus tendon of the contralateral knee, harvesting other autografts (eg, peroneus longus graft), or using allografts, should be considered. Because the inclusion of the gracilis tendon will not lead to a clinically important change in the size of the ACLR graft, its harvest should be avoided to minimize complications such as flexion strength deficits, a shift of peak flexion torque angle to a smaller flexion angle, and loss of knee flexion.
Limitations
The first limitation was that this was a retrospective study and was therefore prone to bias, despite the prospectively collected data regarding hamstring diameter. Second, the smallest diameter that could be measured by the graft sizer used was 4.5 mm; thus, the extremely thin grafts were collectively grouped as “<4.5 mm,” which introduced bias in the analysis. Additionally, the tension used to pass the graft through the graft sizer was not measured and likely not standardized. Also, other methods of standardizing the size, such as measuring the diameter of the hamstring on preoperative MRI, were not performed.
Furthermore, the tendon was folded directly in half for all measurements in the current study. Because the diameter of the tendon changes along the length of the harvested tendon, offsetting the folding point of the gracilis tendon may optimize the thickness of a 4-stranded graft in some patients and address concerns about an extremely thin gracilis tendon. However, the amount of offsetting is likely case specific, and it is not easy to standardize in scientific research. Finally, the interobserver and intraobserver reliability of measuring the tendon and ACLR graft diameter were not available.
Conclusion
When the diameter of a doubled semitendinosus tendon was <6 mm, the addition of a doubled gracilis tendon was unlikely to produce a 4-stranded ACLR graft with a diameter of ≥8 mm. Surgeons should consider alternative methods such as tripling or quadrupling the semitendinosus tendon to increase the size of the ACLR graft, rather than the routine harvesting of the gracilis tendon.
Footnotes
Acknowledgements
The author acknowledges the trainees, residents, and fellows who were rotated to the Division of Sports and Arthroscopic Surgery, Department of Orthopaedics & Traumatology, Queen Mary Hospital, between 2008 and 2018. They assisted in collecting the data for this research.
Final revision submitted June 23, 2024; accepted July 17, 2024.
The author declared that he has no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The University of Hong Kong/Hospital Authority Hong Kong West Cluster (reference No. UW 24-120).