
Abstract
Background:
The Functional Movement Screen (FMS) is used to evaluate fundamental movement patterns in patients. It is unknown whether the FMS can be used as a predictive tool for the occurrence of pitching injuries in baseball players.
Purpose:
To prospectively investigate the relationship between shoulder and elbow injuries and individual components of the FMS during the preseason in high school baseball pitchers and determine which components of the FMS can be used as screening tools to predict shoulder and elbow injuries.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Eligible participants comprised 133 male high school baseball pitchers aged 15 to 17 years who underwent a preseason medical examination in 2017. Included participants were right-handed pitchers who had been involved in preseason practices without restrictions in baseball activities. The physical examination included assessments of background factors, bilateral shoulder and elbow range of motion, and grip and shoulder strength as well as the FMS. A shoulder or elbow injury was defined as any condition causing the inability to pitch for ≥8 days. Injuries occurring in the season immediately after the preseason medical examination were recorded. Logistic regression analysis was performed to identify risk factors associated with an injury.
Results:
Overall, 90 high school baseball pitchers were enrolled in this study. The incidence of injuries was 22.2%. A comparison of FMS scores revealed significantly higher values for shoulder mobility on both sides (dominant side: P = .025; nondominant side: P = .034) and lower values for rotary stability on the dominant side (P < .001) in the injured versus noninjured group. Logistic regression analysis identified poor rotary stability on the dominant side as a significant independent risk factor for baseball injuries (odds ratio, 5.30; P = .009).
Conclusion:
In right-handed high school baseball pitchers, a low FMS score for rotary stability on the dominant side during the preseason was a significant independent risk factor for injuries in the following season. The FMS score for rotary stability may be used as a predictive tool for the occurrence of pitching injuries in high school baseball pitchers.
Shoulder and elbow injuries as well as pain pose significant challenges for baseball athletes.10,23,39 Risk factors related to physical findings, including those of the shoulder,7,13,26,29-32 hip, 15 and ankle, 34 have been identified for shoulder and elbow injuries in baseball players. Other risk factors include the number of pitches thrown 36 and baseball loads (practice, training, and competition hours). 35 Based on these findings, intervention and prevention27,28,37,38 studies have been conducted. However, previous studies were based on conventional physical examinations and did not evaluate dysfunction or compensation in motor patterns, which may not be evident in conventional physical examinations.
The Functional Movement Screen (FMS)8,9 is a tool used to evaluate movement patterns and identify limitations or asymmetries in a patient’s movement mechanics. The FMS consists of 7 fundamental movement patterns believed to be essential for efficient and coordinated motion: deep squat, trunk stability push-up, hurdle step, inline lunge, shoulder mobility, active straight-leg raise, and rotary stability (Figure 1). The FMS has been widely studied as an injury prediction tool,12,14,19,20,41 but there is still no consensus on its usefulness.
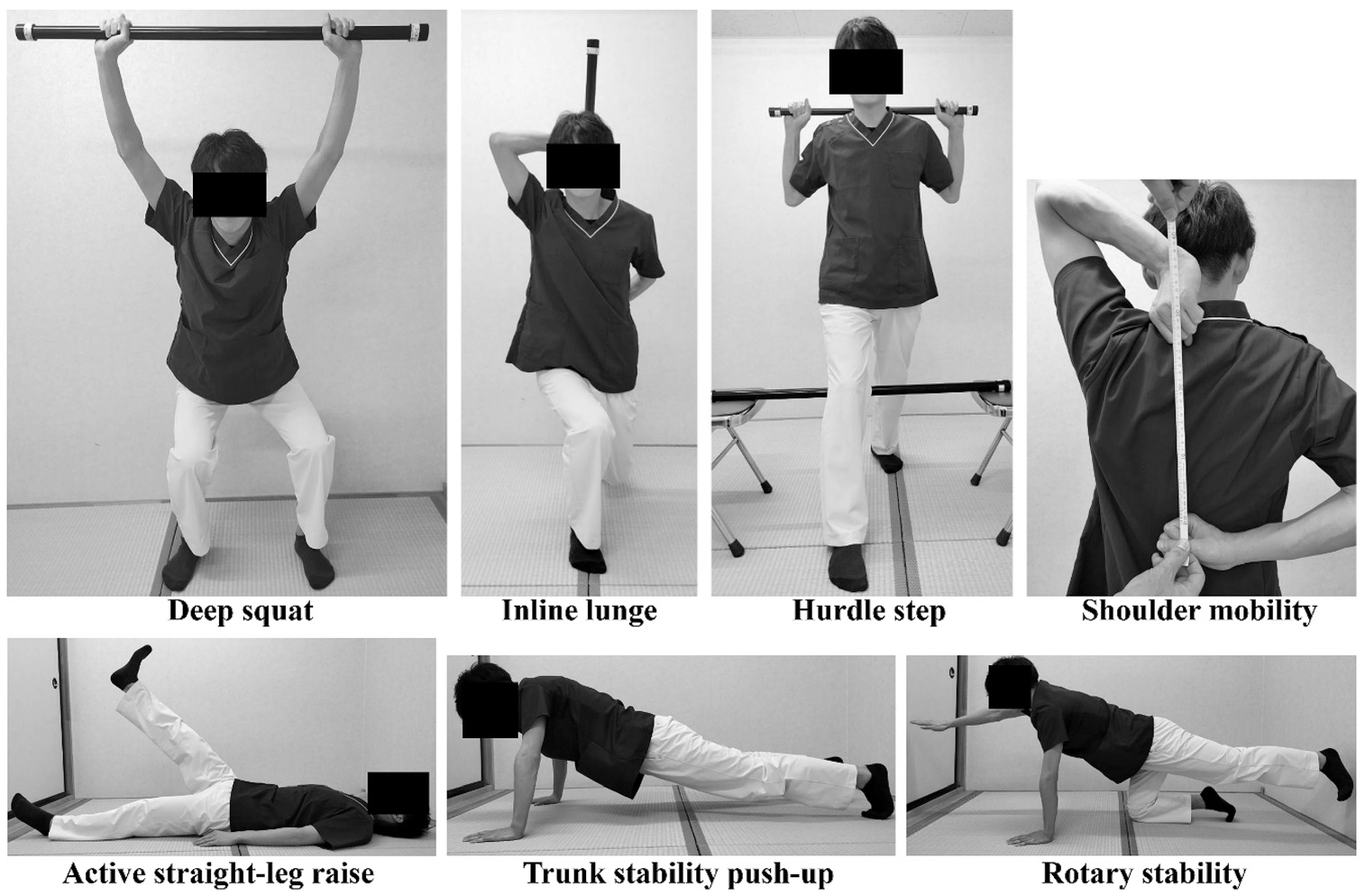
The 7 fundamental movement patterns of the Functional Movement Screen.
A previous study has suggested that the FMS can reliably screen for injuries in emergency services personnel. 3 However, other researchers have cautioned against using the FMS for injury prediction, highlighting its focus on movement quality in athletes. 24 Concerns have been raised about the predictive validity of the FMS because of research limitations. A meta-analysis of studies on active adults, such as firefighters, officer candidates, and athletes, indicated that patients identified as “high risk” by the FMS were 51% more prone to injuries, although the evidence quality of the included studies was very low. 11
Among several studies exploring the link between the FMS and baseball injuries, one study found no significant correlation between the FMS score and past shoulder or elbow surgery in collegiate players, 5 while another cautioned against using the FMS for injury prediction in high school baseball players. 22 Because the FMS composite score represents the result of a whole-body movement pattern, we hypothesized that it might be possible to predict impairment based on baseball-specific movement pattern impairments rather than composite scores. In other words, instead of composite scores, we thought it necessary to prospectively investigate the relationship between the scores of individual components of the FMS and the occurrence of disability. Furthermore, to our knowledge, no prospective study has examined whether the FMS can be used as a predictive tool for the occurrence of pitching injuries in baseball players.
In the current study, we aimed to prospectively investigate the relationship between shoulder and elbow injuries and individual components of the FMS in the preseason rather than composite scores in high school baseball pitchers and determine which components of the FMS can be used as screening tools to predict shoulder and elbow injuries during the baseball season.
Methods
Participants
Eligible participants comprised 133 male high school baseball pitchers aged 15 to 17 years who underwent a preseason medical examination at Gunma University Hospital in 2017. Based on the inclusion criteria in previous studies,31,38 we included pitchers who (1) underwent an annual preparticipation medical/physical examination in the preseason; (2) participated in preseason practices as an active pitcher; (3) had no restrictions in baseball activities, such as throwing, running, and batting, at the time of the preparticipation medical/physical examination; and (4) were right-handed because side-to-side differences in glenohumeral external rotation and humeral torsion angles have been shown to vary significantly between right- and left-handed pitchers among young baseball players.16,40 The exclusion criteria31,38 were (1) past or current shoulder/elbow pain on the dominant side at the time of the preparticipation medical/physical examination; (2) prior injuries (eg, fractures) of the throwing arm; and (3) inability to play baseball because of foot, ankle, knee, hip, spine, shoulder, or elbow problems at the time of the preparticipation medical/physical examination. The protocol for this study received institutional review board approval, and all procedures were conducted in compliance with relevant regulations and guidelines. Before enrollment, informed consent was obtained from the participants and their parents.
Physical Examination
As in previous reports,31,38 the preparticipation medical/physical examination during the preseason was performed as a baseline medical examination to evaluate the preseason condition of the participants’ shoulders and elbows. To avoid confirmation bias, the examiners (N.H. and R.M.), both certified orthopaedic surgeons, were blinded to the participants’ hand dominance. They evaluated the following: (1) background factors (eg, age, body mass index, and baseball experience), (2) bilateral shoulder and elbow range of motion (ROM), (3) grip and shoulder strength, and (4) FMS score.
Shoulder/Elbow ROM
The intrarater validity and reliability of ROM measurements using a digital protractor have been established. 19 The examiners performed all passive ROM measurements using a digital protractor. Consistent with the methodologies employed in prior research,19 passive elbow ROM in flexion and extension, passive shoulder ROM in horizontal adduction, and external rotation and internal rotation at 90° of abduction were assessed bilaterally with the participant in a supine position.
Shoulder/Grip Strength
The intrarater validity and reliability of shoulder strength measurements obtained using handheld dynamometers have been established. 19 In accordance with previous studies,31,38 participants were instructed to adopt a prone position with their humerus abducted at 90° and the elbow flexed at 90°. Subsequently, the examiners measured the prone external rotation (PER) and prone internal rotation (PIR) strengths of the prone shoulder on both sides using the Commander PowerTrack II handheld dynamometer (J-Tech Medical). Each measurement was performed 3 times and recorded, and the median values of the data were analyzed. Subsequently, the dominant-to-nondominant ratios of PER and PIR strengths, along with the PER/PIR ratio on the dominant side, were computed for each participant, and the median values of the data were analyzed. Bilateral grip strengths were measured using a digital dynamometer (Takei Scientific Instruments).
FMS Score
During the screening process, the participants received verbal instructions without any coaching. Regarding FMS scoring, each of the 7 movement tasks (deep squat, trunk stability push-up, hurdle step, inline lunge, shoulder mobility, active straight-leg raise, and rotary stability; the last 5 tasks were assessed on both the dominant and nondominant sides) was evaluated using an ordinal scale ranging from 0 to 3, graded as follows:
0 = presence of pain during the movement,
1 = performing the movement with complete compensations or an inability to execute it,
2 = executing the movement with specific compensations, and
3 = correctly performing the movement without any compensation.
These scores were then summed to derive a composite score ranging from 0 to 21. Although the composite score is usually determined using the lower score from the bilaterally assessed tasks for each movement pattern, in this study, we calculated a separate composite score for each side.
Definition of Shoulder or Elbow Injury
Based on prior research, we defined a shoulder or elbow injury as any condition causing the inability to pitch for ≥8 days.25,31,38 We excluded injuries incurred from instances in which the pitcher was hit by a ball, was involved in a collision with another player, or was injured because of a fall. To avoid recall bias, the participants were instructed to complete a daily self-recorded questionnaire, documenting the presence of shoulder and/or elbow pain, any restrictions in pitching caused by shoulder or elbow discomfort, and the occurrence of other injuries. Injuries occurring in the season immediately after the preseason medical examination were recorded.
Statistical Analysis
Because there are no previous studies on the relationship between the individual components of the FMS and shoulder/elbow injuries, and no investigation on the effect size of each component of the FMS, a sample size could not be calculated for this study. Hence, instead of predicting disability using the FMS, the sample size was determined by referring to risk factor studies on pitching disability in high school baseball pitchers. Thus, a priori power analysis was performed to determine the required sample size, which indicated that a total of 70 participants would be necessary to achieve statistical significance with a statistical power of 80% at an alpha level of .05. This calculation assumed an incidence rate of 20% and an odds ratio (OR) of 2.5. 43
The results of univariate analyses of baseline characteristics and the FMS are presented as the mean ± standard error of the mean. Differences in baseline characteristics between the injured and noninjured groups were evaluated using the Mann-Whitney U test. After controlling for significant variables identified through univariate analyses, logistic regression analysis was performed to identify risk factors associated with an injury. Initially, explanatory variables were selected for inclusion in the model based on the outcomes of univariate analyses (P < .05). 33 Subsequently, the Pearson correlation coefficient was computed to avoid multicollinearity among the explanatory variables. In cases in which a significant correlation was observed between variables, explanatory variables were chosen based on previous research findings and clinical significance. All statistical tests performed in this study were 2-sided, with the significance level set at P < .05. Finally, post hoc power analysis was performed for parameters with P values between .05 and .1 in univariate analyses. All statistical analyses were performed using SPSS Statistics (Version 25; IBM).
Results
Among the 133 eligible participants, 90 high school baseball pitchers were ultimately enrolled in this study. The reasons for exclusion were refusal to participate (n = 13) and left-handedness (n = 30). The incidence of injuries was 22.2% (n = 20 [shoulder: n = 14; elbow: n = 4; both shoulder and elbow: n = 2) (Figure 2).
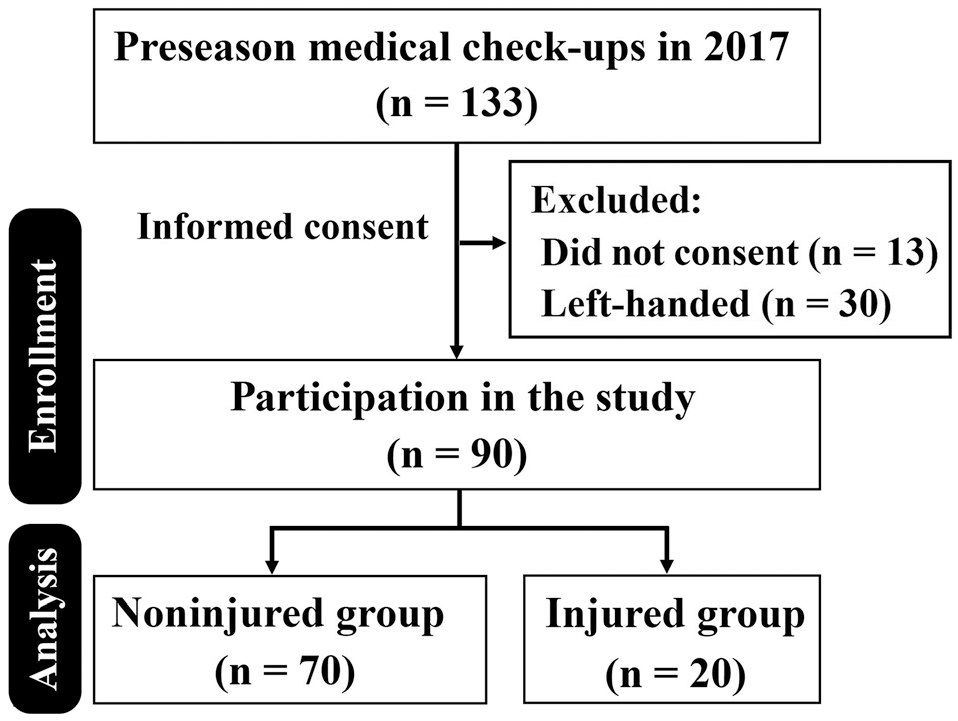
Flow chart of high school pitchers included in this study.
Baseline Characteristics
Comparisons of patient and shoulder/elbow characteristics between the noninjured (n = 70) and injured (n = 20) groups are shown in Table 1. There were no significant differences in patient information, shoulder ROM, elbow ROM, or strength measurements/ratios between the groups (Table 1).
Patient and Shoulder/Elbow Characteristics a

Data are shown as mean ± standard error of the mean. ABER, 90° of abduction and external rotation; ABIR, 90° of abduction and internal rotation; GS, grip strength; HA, horizontal adduction; PER, prone external rotation; PIR, prone internal rotation; ROM, range of motion; total arc, ABER + ABIR.
Difference = ROM on dominant side – ROM on nondominant side.
GS, PER, and PIR ratios = strength on dominant side to strength on nondominant side; PER/PIR ratio = PER/PIR on dominant side.
FMS Scores
A systematic review and meta-analysis 4 revealed that the FMS has excellent interrater and intrarater reliability; the intraclass correlation coefficients in that study were 0.81 (95% CI, 0.69-0.92) for intrarater reliability and 0.81 (95% CI, 0.70-0.92) for interrater reliability. In the present study, the intraclass correlation coefficients for interrater and intrarater reliability were 0.90 and 0.85, respectively, indicating almost perfect agreement for both. 21 The post hoc power for the differences in elbow extension and rotary stability on the nondominant side was 0.24 and 0.43, respectively.
Comparisons of FMS scores between the noninjured and injured groups are shown in Table 2. There was no significant group difference in the FMS composite score on either the dominant side (P = .658) or the nondominant side (P = .620). The FMS score for the shoulder mobility task on both sides was significantly higher in the injured group than in the noninjured group (dominant side: P = .025; nondominant side: P = .034). In contrast, the FMS score for the rotary stability task on the dominant side was significantly lower in the injured group than in the noninjured group (P < .001) (Table 2).
Functional Movement Screen Scores a
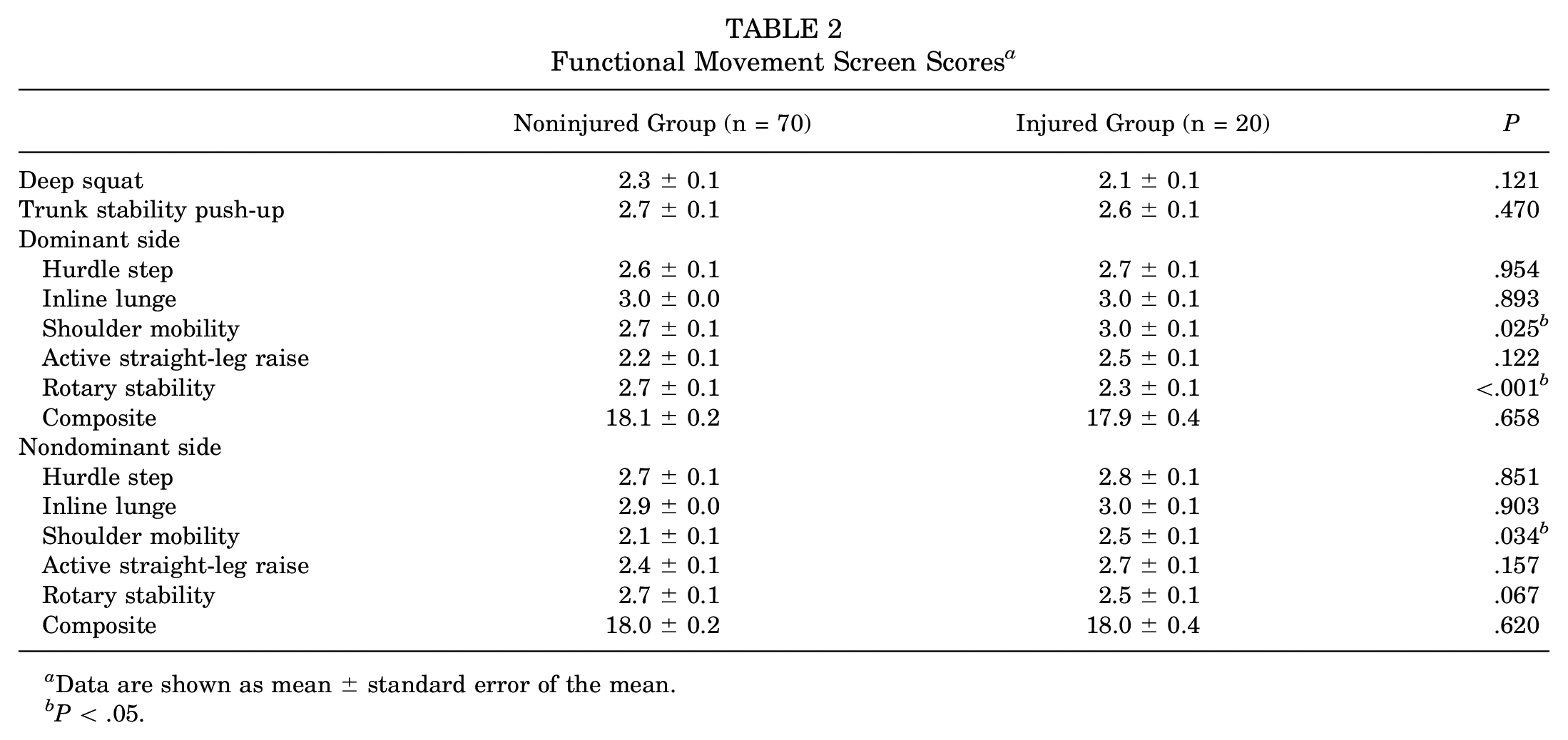
Data are shown as mean ± standard error of the mean.
P < .05.
Logistic Regression Analysis
Based on the results of univariate analyses (P < .05), the shoulder mobility task on both sides and the rotary stability task on the dominant side were selected as potential explanatory variables. Shoulder mobility on both sides was highly correlated (r = 0.467; P = .009), shoulder mobility on the nondominant side was removed, and shoulder mobility and rotary stability on the dominant side were selected for logistic regression analysis.
Logistic regression analysis showed that decreased rotary stability on the dominant side was a significant independent risk factor (OR, 5.30 [95% CI, 1.50-18.65]; P = .009) for baseball injuries (Table 3).
Risk Factors for Baseball Injuries

P < .05.
Discussion
The most important finding of this study was that a low FMS score for rotary stability on the dominant side was a significant independent risk factor for injuries in right-handed high school baseball pitchers. Each 1-point decrease in the FMS score for the rotary stability task was associated with a 5.3-fold increase in the risk of shoulder and elbow injuries. To our knowledge, this is the first prospective study to demonstrate that rotary stability on the FMS may be used as a predictive tool for the occurrence of pitching injuries in high school baseball pitchers.
FMS for Injury Prediction in Athletes
The usefulness of the FMS as an injury prediction tool remains controversial. Kiesel et al 19 evaluated the FMS as a tool for injury prediction in professional American football players over a 4.5-month competitive season. They found that players with an FMS score ≤14 had an 11-fold increased risk of serious injuries compared to those with an FMS score >14. Additionally, a subsequent study of 286 football players with asymmetries and FMS composite scores <14 demonstrated high specificity (0.87 [95% CI, 0.84-0.90]) in predicting time lost due to an injury. 20
In professional-, club-, representative-, international-, and collegiate-level rugby athletes aged ≥18 years, lower composite scores have also been associated with increased time lost due to an injury.12,14,41 Conversely, in a cohort of professional basketball players, the FMS composite score did not demonstrate a predictive ability for the injury risk. 1 Remarkably, a single component of the FMS, the hurdle step, exhibited a positive relationship between the score and injury rate, indicating that higher scores were associated with a greater injury risk. 1
In noncontact sports, Warren et al 42 found no correlation between lower composite scores (<14) and movement asymmetries with overuse injuries among 167 National Collegiate Athletic Association Division I collegiate athletes, including those in basketball, football, volleyball, cross-country, track and field, swimming/diving, soccer, golf, and tennis. Similarly, Bardenett et al 2 found no predictive relationship between the FMS score and injury occurrence in a group of 167 high school athletes, including those in cross-country, football, soccer, swimming, tennis, and volleyball. The inconsistency in findings among these studies could be attributed to methodological variations and differences in outcome measures, thus complicating the ability to make definitive conclusions on this subject.
FMS for Injury Prediction in Baseball Players
Busch et al 5 conducted preseason assessments on collegiate baseball players, employing solely the “shoulder mobility” component of the FMS. They found that a history of shoulder or elbow surgery was not related to performance on the shoulder mobility component evaluated in the preseason in 176 collegiate baseball players. 5 Furthermore, a retrospective study revealed that poor FMS performance, characterized by scores of 0 or 1, was linked to a heightened probability of suffering at least one overuse symptom during the preseason, irrespective of grade and position (adjusted OR, 5.14; P = .03). 6 The aforementioned studies controlled solely for the influences of grade and position as potential confounding factors; furthermore, only 1 of the 7 FMS tasks was evaluated. Therefore, it is essential that studies include and adjust for other potential confounding factors, such as ROM, muscle strength, and appropriate background factors related to the injury occurrence.
Monaco and Schoenfeld 24 reviewed the current literature on the utility of the FMS as a screening tool to identify athletes’ injury risk and reported that future investigations should explore the individual components of the FMS and their predictive efficacy rather than focusing on the composite score. In the present study, we focused on individual components of the FMS and found that one component of the FMS (rotary stability on the dominant side) was a significant risk factor for shoulder or elbow injuries. Furthermore, we evaluated background factors previously reported to be associated with the occurrence of injuries and confirmed that their lack of influence had no impact on the results of this study.
Because there have been no previous studies on the association between rotary stability impairments and baseball-related injuries, we can only speculate. Rotary stability assesses asymmetric trunk stability in both the transverse and sagittal planes during asymmetric upper and lower extremity movements. Poor performance on the rotary stability task can be attributed to insufficient stability of the trunk stabilizers. 9
Pitching movements are executed through activation of the kinetic chain in which discrete body segments, such as the lower extremities, pelvis, trunk, and upper extremities, synchronize their movements through coordinated muscle activity and body positioning. This orchestration facilitates the generation, summation, and transmission of energy throughout the body, culminating in arm propulsion.17,18,29 Therefore, trunk instability, which is the relay point of the kinetic chain, contributes to injuries by increasing the burden on the peripheral trunk (shoulders and elbows).
Limitations
This study had several limitations. First, we did not evaluate external load factors, such as the total number of pitches thrown and number of innings pitched, which could be risk factors during the season. Second, we did not investigate other potential risk factors related to ankle, hip, and knee function during the physical examination. Although the unmeasured confounding factors could affect the results of this study, the major risk factors reported in previous studies (ie, shoulder ROM and muscle strength) were evaluated, and it was confirmed that there were no significant differences between the noninjured and injured groups. Thus, we believe that this did not have a significant impact on the outcome. Third, our investigation was not designed in a way that might have clarified the mechanism underlying the relationship between a low FMS score for rotary stability on the dominant side and the incidence of shoulder and elbow injuries. Further studies are warranted to elucidate the mechanism underlying the relationship.
A fourth limitation was that left-handed pitchers were excluded from this study. This was done because among young baseball players, right- and left-handed pitchers vary significantly in terms of side-to-side differences in glenohumeral external rotation and humeral torsion angles. 40 Thus, further studies are required on left-handed pitchers. Fifth, we did not identify the limiting factor when participants achieved an FMS score <3 for shoulder mobility. Therefore, we did not discuss why better performance on the FMS for shoulder mobility significantly increased the injury risk in univariate analyses. Although multivariate analysis showed that the FMS score for shoulder mobility was not an independent risk factor, further study is required. Finally, we did not collect detailed data on the injuries. Although it is essential for clinicians to consider the location and severity of injuries, the inability to pitch among baseball pitchers is a significant issue, even if persistent elbow/shoulder pain is attributed only to inflammation without any detectable anatomic failure. As our investigation primarily focused on the athlete’s perspective, the correlation between injury severity and the FMS score remains indeterminate.
Conclusion
In right-handed high school baseball pitchers, a low FMS score for rotary stability on the dominant side during the preseason was a significant independent risk factor for shoulder or elbow injuries in the following season. The FMS score for rotatory stability may be a useful predictor for the occurrence of pitching injuries in right-handed high school baseball pitchers.
Footnotes
Acknowledgements
The authors thank the personnel, players, coaches, and staff of the Gunma High School Baseball Federation for their assistance and cooperation in this study. They also thank Kureha Special Laboratory for its assistance with statistical analysis and Editage for English language editing.
Final revision submitted June 16, 2024; accepted June 25, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Gunma University Hospital (No. 1003).