
Abstract
Background:
The importance of monitoring both physical and mental health in athletes across different levels of sport is increasingly acknowledged due to potential injury risks. However, for the Chinese-speaking population, there has not yet been an appropriate assessment tool available.
Purpose:
To translate, culturally adapt, and assess the validity and reliability of the Chinese versions of the updated Oslo Sports Trauma Research Center Overuse Injury Questionnaire (OSTRC-O2) and the Health Problems Questionnaire (OSTRC-H2) among Taiwanese collegiate athletes.
Study Design:
Cohort study (diagnosis); Level of evidence: 3.
Methods:
The OSTRC-O2 and OSTRC-H2 questionnaires were translated from English to Chinese following international guidelines. Subsequently, 80 and 84 collegiate athletes, respectively, were invited to complete these questionnaires on a weekly basis for 8 weeks. Internal consistency was evaluated using Cronbach alpha coefficient, while test-retest reliability was assessed with the intraclass correlation coefficient (ICC). Severity scores from the questionnaires were also documented.
Results:
High response rates of 90% (n = 72/80) and 90.5% (n = 76/84) were achieved in the OSTRC-O2.CH and OSTRC-H2.CH groups, respectively, demonstrating strong acceptance among athletes, with no significant issues in back-translation. High content validity was observed across the different body parts in the translated OSTRC-O2, with Cronbach alpha values of .82, .83, .82, and .83 for the knee, shoulder, elbow, and lower back, respectively. The translated OSTRC-H2 also showed excellent internal consistency, with a Cronbach alpha of .95. The ICC values for test-retest reliability were 0.88, 0.82, 0.92, and 0.92 for the knee, shoulder, elbow, and lower back in the OSTRC-O2, and the ICC for the OSTRC-H2 was 0.90, indicating very good reliability for both questionnaires.
Conclusion:
The Chinese versions of the OSTRC questionnaires were found to be valid and reliable for monitoring overuse injuries and health issues among Chinese-speaking collegiate athletes.
Monitoring the physical and mental health of athletes across various sports and levels of competition has been increasingly emphasized. 7 Numerous studies have delved into epidemiological factors that could act as potential risk factors for injuries and preinjury status, leading to the development of consensus on potential injury events by several sports associations through injury surveillance.14,24,26 The value of injury surveillance has also been validated in studies where the implementation led to a decrease in the prevalence of sports-related injuries, underscoring its vital role in injury prevention.4,19,28 While objective parameters have proven crucial for preventing injuries, recent research has also highlighted the importance of subjective aspects such as pain intensity, functional limitations, psychological impact, and readiness to return to sports in injury prevention efforts.17,31 Another concern is the underestimation of potential injury conditions among elite athletes, especially those with overuse injuries who might continue their training and competition routines despite enduring symptoms and limitations.3,9
The Oslo Sports Trauma Research Center Overuse Injury Questionnaire (OSTRC-O) was developed by Clarsen et al 10 in 2013 to record the extent of overuse injuries by means of a series of self-reported questions to evaluate possible injury status. This questionnaire was distributed periodically to all participants during a surveillance period, capturing all physical complaints across various anatomical areas through a comprehensive definition of injury. It comprised 4 sections aimed at assessing the impact of overuse injuries on athletes. By issuing the questionnaire at consistent intervals (ie, every week), therapists, physicians, and researchers were able to track fluctuations in the impact of overuse injuries over time. In 2024, the Oslo Sports Trauma Research Center Questionnaire on Health Problems (OSTRC-H), which records health problems, was developed. 11 The effectiveness of this questionnaire was assessed and confirmed during the training of Norwegian elite athletes for the 2012 London Olympics; since then, it has been integrated into the daily monitoring systems for Olympic and Paralympic athletes and is utilized in the Olympic and Paralympic programs of various countries. 9 Given its significant outcomes, this approach has been adopted for athletes of diverse sports, across various performance levels and age groups.15,25
The widespread use of both questionnaires in injury surveillance has led to the development and validation of several translations, including Danish, Japanese, Swedish, Spanish, German, Portuguese, and French.6,13,16,18,22,23,27 In addition, updated versions of the original questionnaires (OSTRC-O2 and OSTRC-H2) were published in 2020, with amendments aimed at enhancing convenience and understanding. 9 These updates not only clarified any ambiguity and inconsistencies by revising the phrasing of questions but also introduced a new gatekeeper logic in the initial question to reduce response time for athletes without health issues.
Despite these advancements, a Chinese translation of the questionnaires has not yet been created. The Chinese-speaking world also hosts a large athlete population, with overuse injuries being common across various sports such as baseball, dance, and running, indicating a significant need for these tools in these communities.21,32,34 Hence, this study aimed to translate and culturally adapt the OSTRC-O2 and OSTRC-H2 questionnaires into the Chinese language and to assess their validity and reliability in studying overuse injuries and health problems among Chinese-speaking athletes. We hypothesized that the translated versions would possess adequate validity and reliability for Chinese-speaking athletes.
Methods
The protocol for this study was approved by the institutional review board of Chang Gung Memorial Hospital and complied with the ethical principles of the Declaration of Helsinki. All included athletes were fully informed about the study purpose and process and consented of their own will before their participation.
Translation Procedure
The English versions of the OSTRC-O2 and OSTRC-H2 were utilized for the Chinese translation. The translation of both questionnaires was conducted according to the guidelines produced by Beaton et al 5 and the principles of good practice established by the International Society for Pharmacoeconomics and Outcome Research. 33 We obtained permission from the original developer9,10 to translate the original English versions of the OSTRC-O2 and OSTRC-H2. The translation procedure consisted of the following steps:
Participating Athletes
We contacted the coaches of 2 university volleyball teams, a swimming team, a soccer team, a gymnastics team, and a tennis team to inquire about their interest in participating in our study. After their expression of interest, an introductory meeting was organized for each team, where both the coaches and athletes were informed about the study’s objectives and were asked for their consent to participate through official documentation. Included in this study were athletes who (1) were aged ≥18 years, (2) competed at an elite level, and (3) had Chinese as their first language. Athletes were considered for inclusion irrespective of their current or past injury status. The recruited athletes were randomly assigned to complete either the OSTRC-O2.CH (n = 80) or OSTRC-H2.CH (n = 84).
Content Validity
Content validity was assessed through a 2-step process. Initially, the prevalence of overuse injuries and health issues was gauged using the OSTRC-O2.CH and OSTRC-H2.CH, respectively, across 8 weeks of online self-reporting. Subsequently, 4 binary (yes/no) questions were appended to each submission to inquire (1) if the questionnaire’s queries were pertinent to the athlete’s sport, (2) if completing the questionnaire posed any difficulty, (3) if there was a desire to modify or augment the questionnaire, and (4) if the design of the online questionnaires was satisfactory.13,16 Each question was followed by an area for participants to provide additional comments. The participants were instructed to complete the web-based questionnaires each Friday for 8 weeks. If a response was not received from an athlete within 48 hours, an automatic reminder email was sent.
Test-Retest Reliability
Participants were requested to fill out the questionnaires again within 24 to 48 hours during the third week of the survey to evaluate test-retest reliability. An email notification was sent out in the third week to remind the athletes. If the retest response was not received from an athlete during that week, no additional reminders were issued.
Statistical Analysis
To assess reliability, the intraclass correlation coefficient (ICC) for the severity scores derived from the 4 questions in both questionnaires was calculated based on test-retest measurements, with a value of ≥0.90 recommended for reliability. 12 Internal consistency was evaluated by calculating the Cronbach alpha, where a value of 0 indicates no internal consistency and 1 indicates perfect consistency. This calculation was specifically applied to the 4 main questions of each reported questionnaire. All statistical analyses were conducted using SPSS (Version 25.0.1; IBM Corp).
Results
Translation and Adaptation
As OSTRC-O2.CH and OSTRC-H2.CH are closely related, the translation process for both is collectively summarized. No major problems were reported in the forward translation of the questionnaires. Minor discrepancies included were sentence structure and the selection of synonymic use of nouns to describe the locations or the symptoms of injury and illness. For example, instead of “其他的症狀” (“other complaints”), we utilized “其他的不舒服” (“other discomforts”). Also, instead of “填入解剖位置” (“insert anatomical location”) we utilized a multiple-choice question with “脖子, 肩膀, 手肘, 手腕, 骨盆, 大腿, 膝蓋, 小腿, 腳踝, 或其他 (請自行填入),” or “neck, shoulder, elbow, wrist, pelvis, thigh, knee, calf, ankle, or other (please fill in).” No prominent distortions were seen in the back translations compared with the original versions of the questionnaires.
Cognitive Debriefing
The cognitive debriefing with 10 participants led to no modifications in the OSTRC-O2.CH. During the cognitive debriefing for OSTRC-H2.CH, no alterations were made to the question format within the answering section. Nevertheless, a coach suggested a revision in the section that describes “health problem” at the start of the questionnaire: The phrase “正常健康狀態” (“normal status of full health”) was unclear, so it was replaced with “不受健康影響的狀態” (“normal status without being affected due to altered health”). Additionally, to ensure consistency between the OSTRC-O2.CH and OSTRC-H2.CH, we endeavored to use identical terminology in both questionnaires wherever possible.
Athlete Characteristics
Assuming a power of 0.8, an anticipated reliability of 0.9, an effect size of Cohen d = 0.8, and a significance level set at .05, the estimated number of respondents needed to conduct statistical analyses was determined to be 52. A total of 72 participants for the OSTRC-O2.CH and 76 participants for the OSTRC-H2.CH were closely followed for 8 weeks. The mean response rate for the OSTRC-O2.CH during the 8 weeks was 90% (95% CI, 88.4%-93.1%), and for the OSTRC-H2.CH, the mean response rate was 90.5% (95% CI, 89.8%-95.5%), indicating strong acceptance among the participants. The characteristics of the participating athletes for each questionnaire are shown in Table 1.
Basic Characteristics of the Participating Athletes a
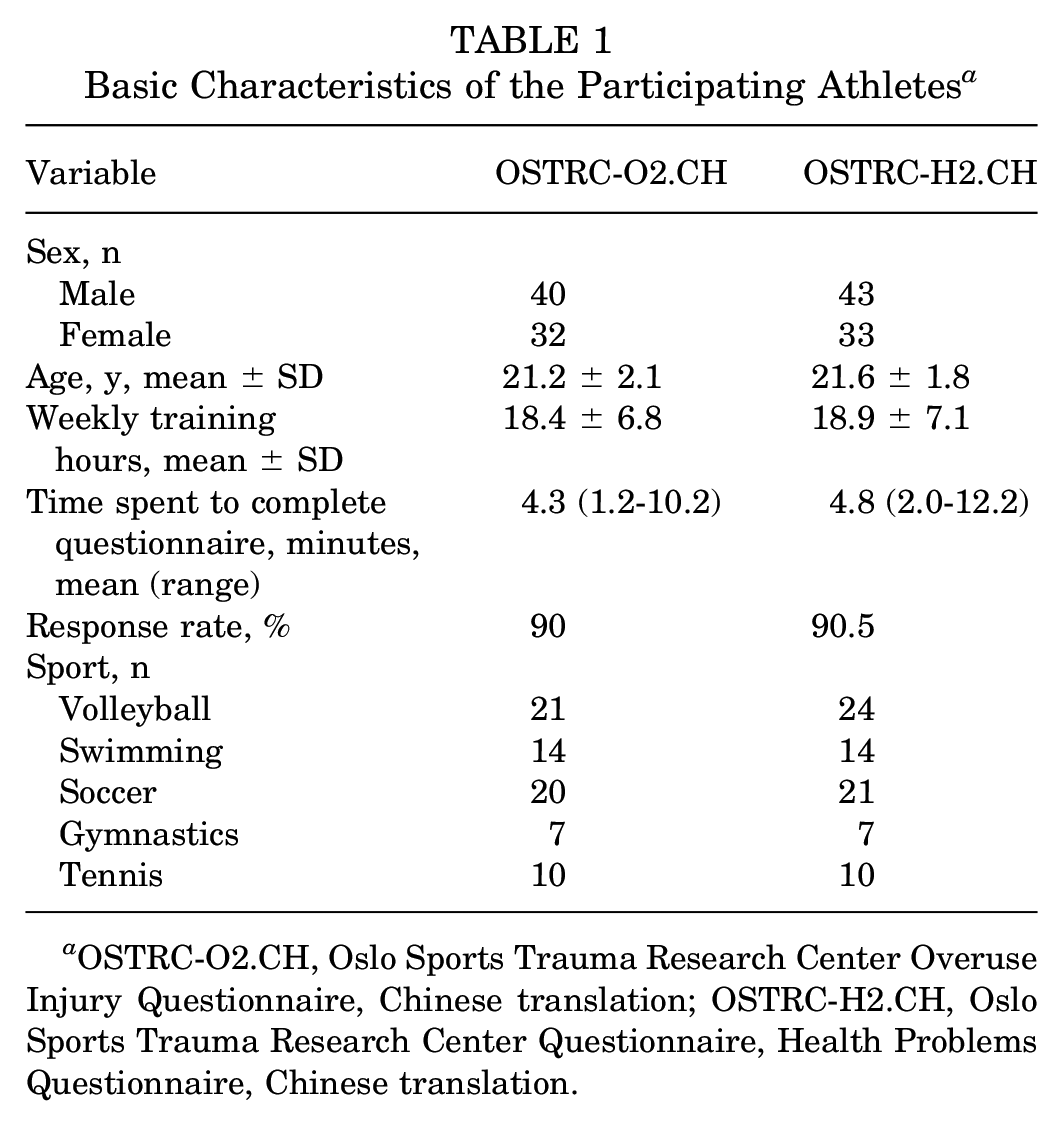
OSTRC-O2.CH, Oslo Sports Trauma Research Center Overuse Injury Questionnaire, Chinese translation; OSTRC-H2.CH, Oslo Sports Trauma Research Center Questionnaire, Health Problems Questionnaire, Chinese translation.
Content Validity
All athletes concurred that the questions in the form were pertinent to their sports and found the questionnaires easy to complete, with no suggestions for changes or additions. Regarding the web-based questionnaires, some athletes mentioned that they were not optimally designed for completion on smartphones, suggesting that developing an application for the questionnaires might improve usability.
Reliability
Test-retest analysis was conducted with 54 participants for the OSTRC-O2.CH and 52 for the OSTRC-H2.CH, who completed the questionnaires again within 24 to 48 hours in the third week. The ICC values for the OSTRC-O2.CH were 0.88 (95% CI, 0.59-0.96) for the knee, 0.82 (95% CI, 0.67-0.94) for the shoulder, 0.92 (95% CI, 0.82-0.96) for the elbow, and 0.92 (95% CI, 0.82-0.96) for the lower back. The ICC for the OSTRC-H2.CH was 0.90 (95% CI, 0.79-0.95) (Table 2). The values indicated very good reliability for both questionnaires.
Reliability and Internal Consistency of OSTRC-O2.CH and OSTRC-H2.CH a
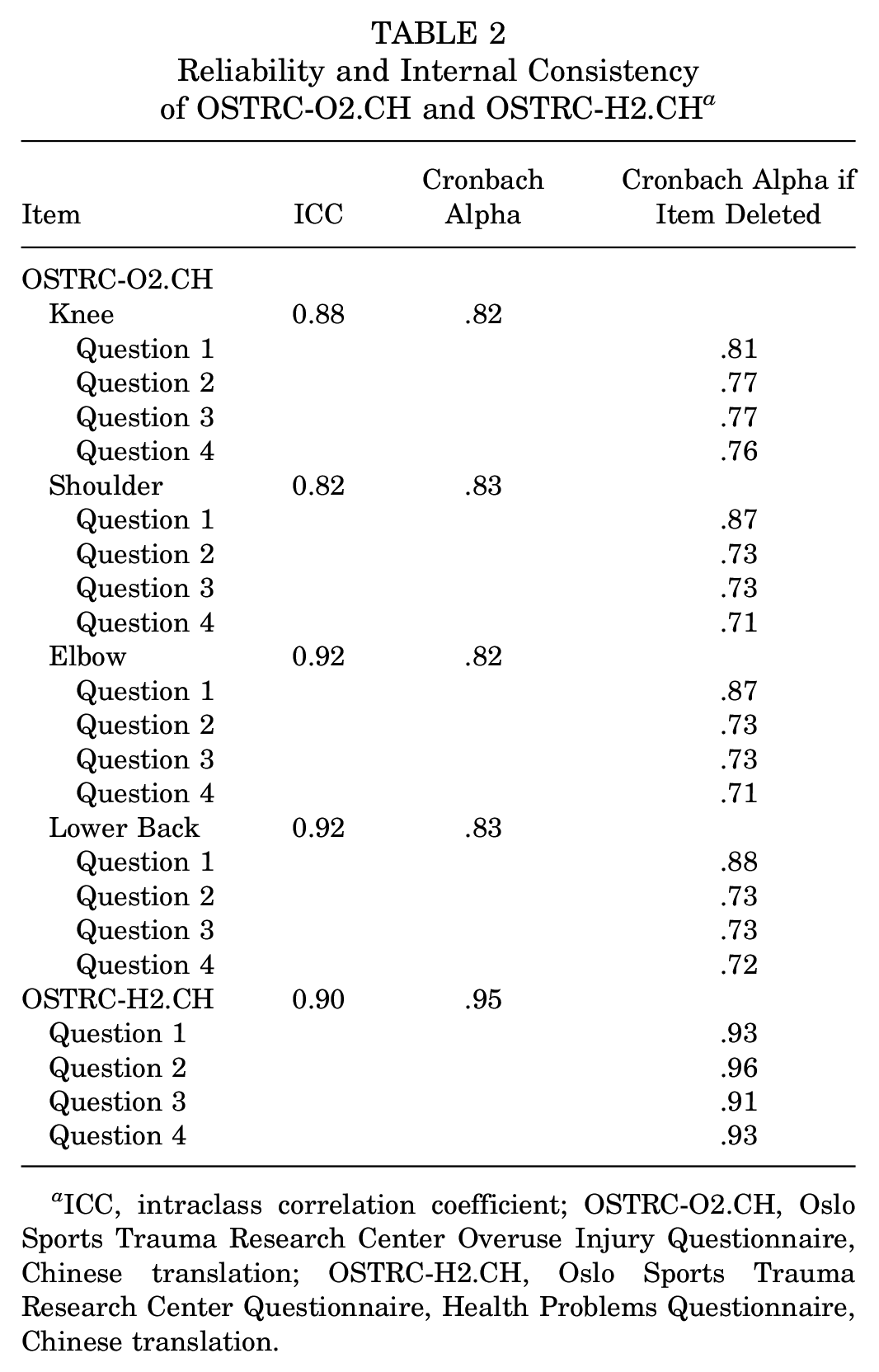
ICC, intraclass correlation coefficient; OSTRC-O2.CH, Oslo Sports Trauma Research Center Overuse Injury Questionnaire, Chinese translation; OSTRC-H2.CH, Oslo Sports Trauma Research Center Questionnaire, Health Problems Questionnaire, Chinese translation.
The internal consistency of the 4 key questions in the OSTRC-O2.CH over 8 weeks showed a Cronbach alpha of .82 (95% CI, .79-.86) for the knee, .83 (95% CI, .80-.86) for the shoulder, .82 (95% CI, .78-.86) for the elbow, and .83 (95% CI, .79-.88) for the lower back. The overall Cronbach alpha for the OSTRC-H2.CH was .95 (95% CI, .93-.97) (Table 2).
Severity Score
Severity scores for overuse injuries and health issues were calculated on a weekly basis following the OSTRC methodology. The severity scores in the original OSTRC.O2 and OSTRC.H2 questionnaires were designed to quantify the impact of health problems and overuse injuries on athletes. These scores were derived from athlete-reported symptoms, functional impairment, and participation restrictions. The higher the score, the more severe the problem. The key aspect of using these questionnaires was not only the absolute severity score at a single point in time but also the trends observed over weekly assessments. In this study, the weekly mean severity scores were 6.2 for the OSTRC-O2.CH and 8.8 for the OSTRC-H2.CH. The trends of these severity scores are depicted in Figure 1.

Line graphs of weekly mean severity scores on the (A) Oslo Sports Trauma Research Center Overuse Injury Questionnaire, Chinese translation (OSTRC-H2.CH) and (B) Oslo Sports Trauma Research Center Questionnaire, Health Problems Questionnaire, Chinese translation (OSTRC-H2.CH)
Discussion
Numerous studies have underscored the rising incidence of overuse injuries, particularly among adolescent and collegiate athletes across various sports.1,2,20 Additionally, the mental health of elite athletes is receiving increased attention.29,30 To tackle these issues, Clarsen et al9-11 developed and refined self-reported questionnaires designed to identify potential problems among athletes. Owing to their effectiveness and ease of use, these questionnaires have been translated into several languages and validated.6,16,18,22,27 Given that Chinese-speaking athletes represent a significant demographic, constituting about 5% of all athletes, the prevalence of overuse injuries in these populations has been documented in recent studies.8,21,34 Despite the growing awareness of these issues among Chinese-speaking athletes, there has yet to be a validated Chinese translation of these questionnaires. As a result, this study sought to translate and culturally adapt the OSTRC-O2 and OSTRC-H2 questionnaires into Chinese, filling the gap in self-reporting tools for evaluating potential overuse injuries and health issues in Chinese-speaking athletes.
Utilizing a well-established translation methodology,5,33 we translated and modified the original OSTRC questionnaires for Chinese-speaking athletes. The back-translation process revealed no significant discrepancies with the original versions, though some adjustments were made to better suit Chinese-speaking athletes. For data collection, we employed web-based questionnaires, distributed via email notifications to prompt athlete responses. The participants found the questionnaires straightforward and quick to complete. Conducted among Taiwanese collegiate athletes, this study leveraged the widespread use of smartphones among this group, making web-based questionnaires a practical choice for easy completion and submission. The use of email notifications also proved effective in ensuring timely responses.
During an 8-week cohort study with collegiate athletes, content validity for both questionnaires was evaluated, revealing very high response rates that indicated strong acceptance and adherence among the participants, mirroring the outcomes seen with other translated versions of the OSTRC questionnaires. The majority of athletes confirmed the relevance of the questionnaire correlates to their sports and reported ease in completing the web-based questionnaires. Furthermore, several athletes noted that the email reminders were effective in prompting them to fill out the questionnaires if they had forgotten. The Cronbach alpha values were high (>.80 in both questionnaires), indicating high internal consistency.
Test-retest reliability, evaluated in the fourth week of our study, demonstrated high ICCs for both questionnaires, suggesting their high reliability. Jorgensen et al 18 observed a lower ICC value for a test-retest interval of 2 weeks as opposed to 1 week, suggesting that a longer interval might allow for natural variations in the severity of injuries and illnesses, potentially affecting perceived reliability. In line with other studies on translating these questionnaires,16,23,27 which conducted the retest within 24 hours of the initial test, we opted for a retest period between 24 and 48 hours. While a shorter interval may introduce memory effects or recall bias, we deemed a longer test-retest interval inappropriate due to the potential for intraindividual severity scores to change even after a single training session.
Concerning the above-mentioned results, the successful translation and validation of the OSTRC-O2 and OSTRC-H2 questionnaires into Chinese provide significant benefits for the Chinese-speaking athletic community. The translated versions allow for consistent and accurate monitoring of overuse injuries and health problems among Chinese-speaking athletes, addressing the unique cultural and linguistic needs of this population. This adaptation ensures that the questionnaires are not only linguistically accurate but also culturally relevant, enhancing the validity of the responses and the reliability of the data collected. The utilization of these translated questionnaires enables health care providers and researchers to monitor athletes’ health conditions effectively, helping to prevent possible overuse injuries. This is particularly important given the high incidence of overuse injuries in this population, as highlighted in recent studies involving Chinese athletes across various sports.21,34
Moreover, the high internal consistency and test-retest reliability demonstrated by the translated versions underscore their robustness as tools for longitudinal monitoring. The integration of these validated instruments into routine practice or during competitive events can significantly enhance injury surveillance and management, ultimately contributing to better health outcomes for Chinese-speaking athletes. These tools also facilitate international research collaborations, allowing for comparative studies and the pooling of data across different linguistic and cultural groups.16,18,23
Limitations
There are some limitations to this study. First, specific diagnoses for the reported overuse injuries or health problems were not recorded, even though some athletes provided this information via email. Second, there is a risk that the responses may not be accurate, with possible errors in the reported anatomical areas or athletes potentially withholding information about their injuries. Third, this study focused exclusively on collegiate elite athletes over an 8-week period during their competitive season, which means the findings may not apply to other athlete populations with different ages and performance levels. The injury trends and health issues could also vary with different times of the year. Additionally, while this study indicates that the OSTRC-O2.CH and OSTRC-H2.CH could be beneficial for other Chinese-speaking athletes, its effectiveness for the broader Chinese-speaking athlete population was not assessed. It is important to acknowledge the linguistic diversity within this group. With various dialects spoken across different regions, further amendments may be necessary to ensure the tools are fully accessible and comprehensible to speakers of different Chinese dialects. Future research should aim to involve a larger and more diverse group of participants and extend the follow-up period to gain more comprehensive insights.
Conclusion
The OSTRC-O2.CH or OSTRC-H2.CH were found to be valid and reliable for monitoring overuse injuries and health issues among Chinese-speaking collegiate athletes.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241303983 – Supplemental material for Chinese Translation and Validation of the Oslo Sports Trauma Research Center Questionnaires on Overuse Injuries and Health Problems
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241303983 for Chinese Translation and Validation of the Oslo Sports Trauma Research Center Questionnaires on Overuse Injuries and Health Problems by Yi Lu, Joe Chih-Hao Chiu, Alvin C. Chen, Kuo-Yao Hsu, Yi-Sheng Chan, En-Chong Zhang and Huan Sheu in The Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgements
The authors express their gratitude to all the athletes for their participation, as well as to Dr Benjamin Clarsen for granting permission to translate and providing support for the Chinese translation of the Oslo Sports Trauma Research Center Questionnaires.
Correction (August 2025):
This article has been updated to correct the IRB approval number.
Final revision submitted May 19, 2024; accepted June 17, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Chang Gung Medical Foundation (ref No. 202400610B0).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.