
Abstract
Background:
Quadriceps performance after anterior cruciate ligament reconstruction (ACLR) is typically characterized by peak force/torque, but the ability to generate consistent knee extensor torque may be clinically meaningful.
Purpose/Hypothesis:
The purpose of this study was to evaluate knee extensor torque steadiness and quadriceps activation variability in collegiate athletes 4 to 12 months after ACLR. It was hypothesized that between-limb asymmetries in torque steadiness and activation variability would be observed and that steadiness would be associated with activation variability and peak knee extensor torque symmetry.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 30 National Collegiate Athletic Association Division I athletes completed maximal voluntary isometric contractions 4, 6, and 12 months after ACLR. Torque and surface electromyography of the superficial quadriceps were recorded. Torque steadiness was calculated as the mean difference between initial and low-pass filtered torque signals and was expressed as a percentage of peak torque. Quadriceps activation variability was calculated similarly and was expressed as a percentage of peak electromyography. Linear mixed models were used to assess change in torque steadiness and activation variability over time. Associations between torque steadiness of the operated limb, activation variability, and quadriceps strength symmetry were evaluated using the Spearman correlation coefficient.
Results:
Limb-by-time interactions were detected for torque steadiness and activation variability (P < .001), with reductions (improvements) in limb steadiness and activation variability observed with increasing time since surgery. Between-limb differences in torque steadiness and activation variability were observed at 4 and 6 months postoperatively (P < .05). Significant associations between operated limb torque steadiness and quadriceps activation variability were observed at 4 months (P < .001) and 6 months (P < .01). Torque steadiness of the operated limb was associated with peak knee extensor torque symmetry at 4 months (rS = −0.49; P < .01) and 6 months (rS = −0.49; P < .01).
Conclusion:
In collegiate athletes, impaired knee extensor torque steadiness of the operated limb and associated abnormal quadriceps activation patterns were observed 4 to 12 months after ACLR, and the consistency of knee extensor torque production was associated with greater quadriceps strength asymmetries, particularly 4 to 6 months after surgery. Operated limb torque steadiness and activation variability improved from 4 to 12 months after ACLR. Clinical assessment of knee extensor torque steadiness after ACLR may improve prognosis and specificity of rehabilitation efforts.
Quadriceps neuromuscular dysfunction is universal after anterior cruciate ligament (ACL) reconstruction (ACLR). 16 Persistent quadriceps muscle weakness,3,20 atrophy, 9 and altered excitability19,43 are common, may undermine a successful return to athletic activity, 8 and contribute to long-term knee joint dysfunction. 1 Quadriceps performance is often characterized by measurements of peak force or peak knee extensor torque production, 21 but measuring only the peak force-generating capacity of the muscle does not capture the deficits in force steadiness that may be present after ACLR.
Force or torque steadiness quantifies the capacity to produce smooth and consistent contractile forces 10 and is typically evaluated as the variability in force production during a sustained contraction. 11 Previous investigations have reported reduced force steadiness or force control of the involved limb quadriceps in individuals after ACL injury4,28,35,37 and surgical reconstruction.13,14,26,30,32,33 Reduced force steadiness after ACL injury and surgery is associated with lower central activation ratio, 13 worse single-leg hop performance, 28 and failure of a functional testing battery. 26
Decreases in quadriceps activation and/or motor unit firing frequency commonly occur with ACL injury and reconstruction7,41 and may result in poor force steadiness. These neurological changes can be challenging clinical barriers to recovery of quadriceps neuromuscular function and may contribute to undesirable outcomes, such as protracted return-to-sports time frames, diminished athletic performance, and increased future injury risk. Further, investigations of upper extremity force control in healthy individuals have found significant coherence between low-frequency fluctuations in force and muscle activation patterns, 22 but no studies have explored the relationship between quadriceps activation patterns and force or torque steadiness after ACLR.
Although previous investigations have reported altered quadriceps force control or force steadiness or impairments in knee extensor torque steadiness after ACLR, the majority of these studies were cross-sectional in nature,30,32 with significant variability in the postsurgical time of participant populations13,14 or entailing participants >1 year after surgery.26,33 The influence of time after surgery on quadriceps force variability during a more clinically relevant interval, where deficits could potentially be addressed more readily, has not been explored. In addition, the underlying muscle activation patterns, which directly correspond to the contractile output during a voluntary contraction, 6 have not been evaluated in relation to force or torque steadiness in individuals after ACLR. Establishing the timeline of torque steadiness and quadriceps activation impairments throughout the first year after ACLR would help inform the design of physical therapy rehabilitation protocols for athletes aiming to return to sport.
The purposes of this study were to (1) evaluate knee extensor torque steadiness and quadriceps activation variability in both limbs of collegiate athletes at 4, 6, and 12 months after ACLR; (2) determine the associations between knee extensor torque steadiness and quadriceps activation variability; and (3) evaluate the relationship between peak torque symmetry and torque steadiness. We hypothesized that between-limb asymmetries in knee extensor torque steadiness and activation variability would be most prominent at 4 months postoperatively, that knee extensor torque steadiness would be significantly associated with quadriceps activation variability, and that torque steadiness of the operated limb would be associated with peak knee extensor torque symmetry.
Methods
Participants
Institutional review board approval was obtained for the study protocol. This investigation was an observational analysis of prospectively collected data from the Badger Athletic Performance database. National Collegiate Athletic Association (NCAA) Division I student-athletes at the University of Wisconsin–Madison who undergo ACLR complete a standardized battery of neuromuscular and biomechanical performance assessments at regular intervals after surgery. Participants whose data was included in this study were athletes who had undergone ACLR and completed performance testing at 3 distinct intervals between 4 and 12 months after surgery. Athletes who underwent a follow-up surgical procedure within 12 months after ACLR were excluded from this dataset.
Assessment Protocol
As part of a battery of tests, athletes performed voluntary isometric knee extension contractions to assess quadriceps muscle performance of each limb. Participants were secured in the chair of an instrumented dynamometer (Biodex System 4 Pro; Biodex Medical Systems) with hips flexed to 85° and knees at 90° of flexion. The knee adapter pad was reversed from the commercially standardized alignment to minimize compliance within the system and was affixed to the shank roughly 5 cm proximal to the medial malleolus. The nonoperated limb was always tested first. Skin preparation was completed, and surface electromyography (EMG) electrodes (Delsys Trigno) were placed over the muscle bellies of the vastus lateralis (VL), rectus femoris (RF), and vastus medialis (VM), consistent with SENIAM (Surface ElectroMyoGraphy for the Non-Invasive Assessment of Muscles) guidelines. 15 Athletes completed submaximal warmup trials at 50%, 75%, and 90% of maximum effort followed by a minimum of 2 ramp-and-hold maximal isometric knee extension contractions. Athletes were instructed to attempt to extend the knee with maximal effort and to maintain the contraction for 5 seconds. Loud verbal encouragement and visual feedback of the torque signal were used to facilitate maximal torque production. One minute of rest was provided between subsequent efforts. If maximal knee extensor torque increased by >10% between trials, additional trials were completed until maximal torque production plateaued.
Signal Sampling and Processing
Torque and EMG signals were recorded at 2000 Hz. Torque signals were filtered with a 60-Hz low-pass filter.
Torque Steadiness
The torque-time signal of each repetition was visually inspected, and the period of signal plateau was identified. This plateau region excluded the increase in torque at the initiation of contraction and the dissipation of torque production as the athlete relaxed. The plateau region was required to be at least 3 seconds in length and was truncated at a maximum of 4 seconds. Within this 3- to 4-second window, the torque signal was low-pass filtered with a third-order Butterworth filter (2-Hz cutoff). The mean of the difference between the initial and 2-Hz filtered torque signals was normalized to the maximal torque production of the corresponding repetition to produce the torque steadiness. This value was multiplied by 100 to produce a value that could be interpreted as a percentage of peak torque (%PT) production (Figure 1). Our method built on previous approaches23,32 in an attempt to best quantify the inconsistencies in voluntary torque output associated with neuromuscular dysfunction.

Sample knee extensor torque-time signals from the operated and nonoperated limbs of a representative participant 4 months after anterior cruciate ligament reconstruction. The plateau region (shaded boxes) illustrates the raw torque signal (in gray) and the 2-Hz filtered signal (in black). The line graphs in the bottom row depict the difference between the raw torque signal and the 2-Hz filtered signal (in gray) and the mean value of this difference (dark dotted line). The mean value is divided by the peak torque (marked on each torque-time curve) of the raw signal to produce the torque steadiness.
Quadriceps Activation Variability
Surface EMG data were processed with a 500-ms root-mean-square (RMS) filter. Quadriceps activation data for each muscle that aligned with the torque plateau window were extracted for each repetition. The RMS filtered signal was then low-pass filtered with a third-order Butterworth filter (2-Hz cutoff). Similar to the torque data, the difference between the RMS filtered signal and the further processed, low-frequency EMG signal was used to represent the muscle activation variability of the VL, RF, and VM. The difference between the filtered signals was then normalized to the peak EMG of the 500-ms RMS signal for each muscle (Figure 2). Custom algorithms created using Matlab (MathWorks) were used for signal processing and computation of key outcomes.
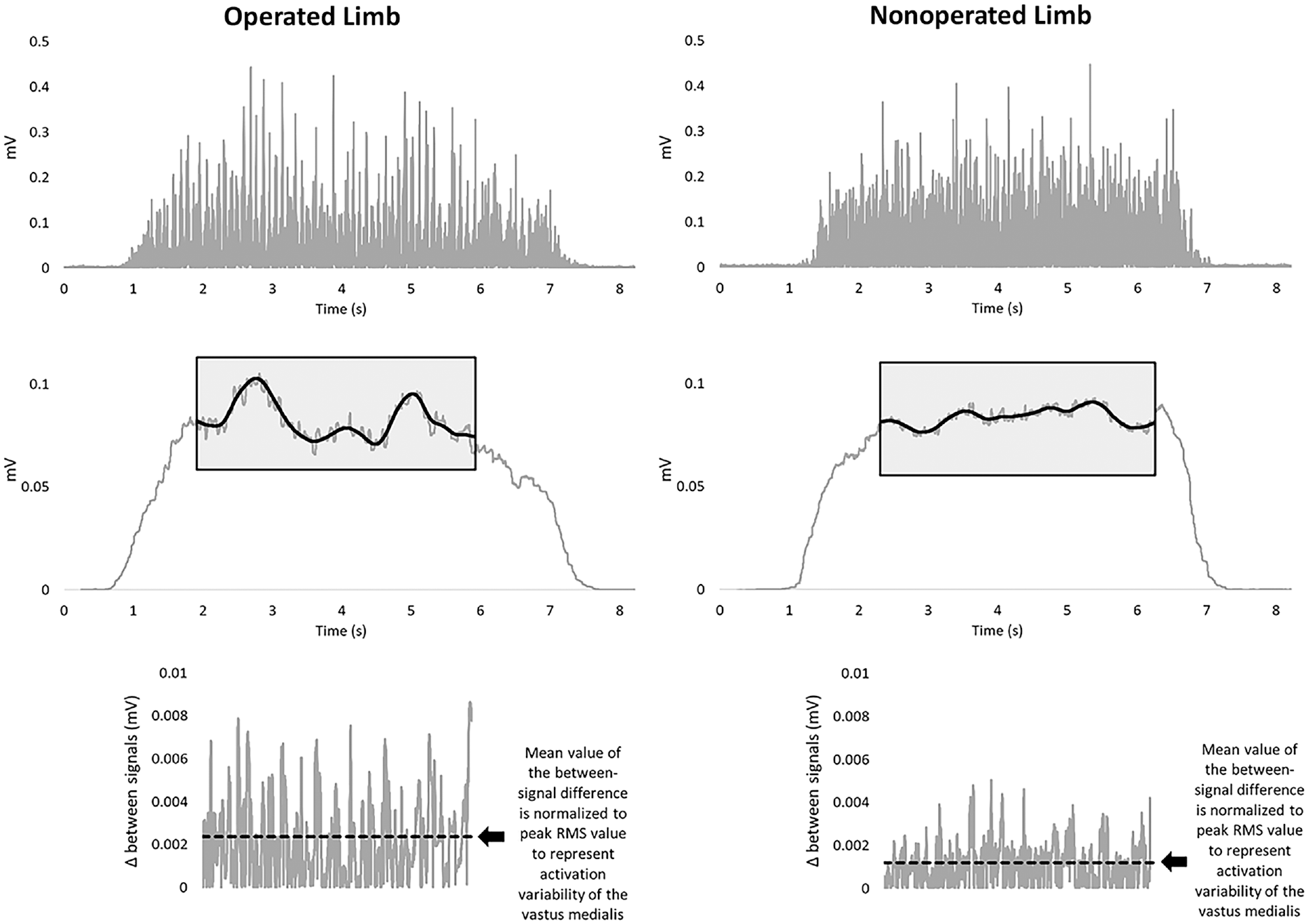
Sample vastus medialis surface electromyography (EMG) signal collected from each limb during the voluntary isometric knee extension efforts displayed in Figure 1. The rectified EMG signals are displayed in the top row, whereas the middle row illustrates the 500-ms root-mean-square (RMS) filtered signal. The plateau region and the 2-Hz filtered signal (black line) are displayed in the shaded boxes. The line graphs in the bottom row depict the difference between the 500-ms RMS-filtered signal and the 2-Hz filtered signal (in gray) and the mean value of this difference (dashed black line). This mean value is normalized to the peak value of the 500-ms RMS-filtered signal and represents the activation variability of the vastus medialis.
Statistical Analysis
All statistical analyses were performed using SPSS (Version 28.0; IBM). Means and associated standard deviations were reported for all variables of interest. Linear mixed-effects models were used to assess changes in torque steadiness and activation variability of both limbs over time and the limb-by-time interactions. Participant and limb were assigned as random effects, whereas time, limb, and their interaction were assigned as fixed effects. A sensitivity analysis excluding athletes with previous ACLR was performed for torque steadiness and activation variability models. The Spearman correlation coefficient (rS) was used to evaluate the associations of operated limb torque steadiness with activation variability and peak knee extensor torque limb symmetry index (calculated as [peak torque of the operated limb ÷ peak torque of the nonoperated limb] × 100). The threshold for significance was P≤ .05.
Results
Participant Characteristics
Records for 30 athletes met the inclusion criteria for this study. Surgery for 27 of the athletes was performed by 1 of 4 fellowship-trained team physicians, whereas the other 3 athletes underwent surgery at an outside facility. Athletes participated in basketball (n = 2), spirit squad (n = 3), football (n = 7), softball (n = 2), soccer (n = 11), track and field (n = 2), volleyball (n = 2), and hockey (n = 1). The majority of the sample (27/30) underwent reconstruction with bone-patellar tendon-bone autografts. Of the 30 athletes, 6 had undergone prior ACLR. Five of these subsequent ACLRs entailed secondary injuries (2 ipsilateral limb, 3 contralateral limb), and 1 ACLR entailed a quaternary injury (this athlete underwent 2 previous ipsilateral ACLRs and 1 previous contralateral ACLR). Concomitant meniscal procedures were performed in 17 of the 30 participants, entailing 9 meniscectomies and 8 meniscal repairs. In addition to undergoing ACLR, 1 athlete underwent medial patellar femoral ligament reconstruction and 1 athlete had concomitant lateral collateral ligament reconstruction. All athletes followed the same postoperative protocol and completed rehabilitation in the same sports medicine facility. The protocol was developed collaboratively by sports medicine physicians and rehabilitation providers, consisting of 5 phases through which the athletes progressed by achieving objective performance criteria based on range of motion, joint effusion, gait mechanics, strength, and functional testing. Participant characteristics are provided in Tables 1 and 2.
Participant Characteristics (N = 30) a

Data are reported as mean ± SD or No. of patients. IKDC, International Knee Documentation Committee Subjective Knee Evaluation.
IKDC scores were missing for 3 patients at the 4-month follow-up, 2 patients at the 6-month follow-up, and 1 patient at the 12-month follow-up.
Peak Isometric Knee Extensor Torque for the Operated and Nonoperated Limbs a
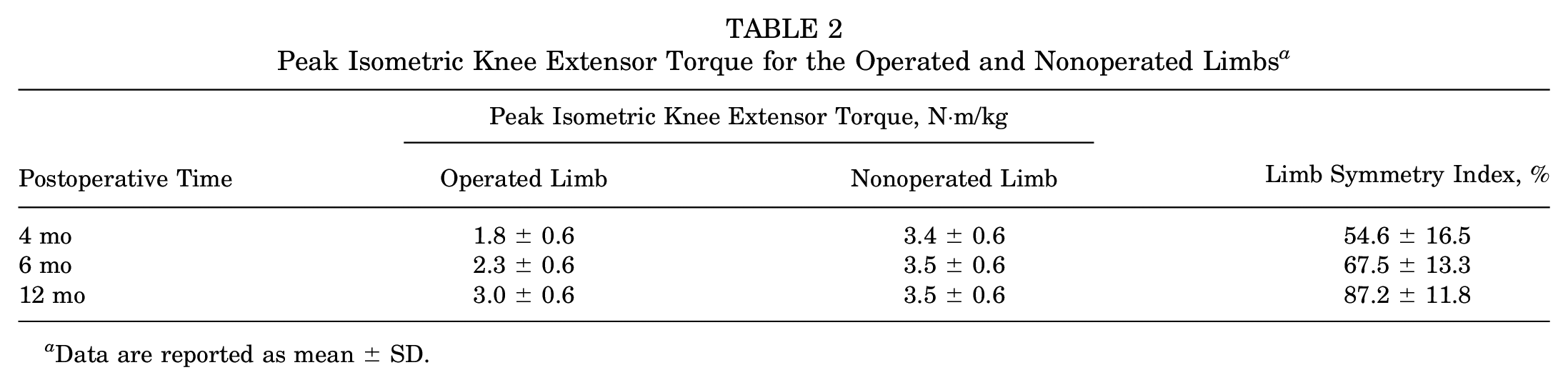
Data are reported as mean ± SD.
Torque Steadiness
A significant limb-by-time interaction effect was observed for torque steadiness (P < .001). Torque steadiness for the operated limb was significantly different between all postoperative timepoints (4 months, 1.45 ± 1.16 %PT; 6 months, 0.82 ± 0.71 %PT; 12 months, 0.50 ± 0.36 %PT; P≤ .01 for all). Torque steadiness for the nonoperated limb at 6 months (0.35 ± 0.16 %PT) was significantly different from that at 12 months (0.41 ± 0.19 %PT; P = .04). Significant between-limb differences were detected at 4 months (mean difference [MD], 1.05 ± 1.00 %PT; P < .001) and 6 months (MD, 0.48 ± 0.61 %PT; P < .001) postoperatively (Figure 3).

Box plots illustrating knee extensor torque steadiness for the nonoperated and operated limbs at 4, 6, and 12 months after surgery (as a percentage of peak torque production). Higher values represent more unsteadiness or greater signal variability. Error bars extend to minimum and maximum values, and circles denote outliers (ie, values outside of quartile ±1.5 × interquartile range). Significant differences between limbs at each time point are shown by vertical asterisks placed between box plots. Significant differences within limbs over time are shown by gray horizontal bars above (operated limb) or black horizontal bars below (nonoperated limb) box plots. The dashed line represents a y-axis break to illustrate a significant outlier in the operated limb group at 4 months postoperatively. *P < .05. **P < .01. ***P < .001.
Quadriceps Activation Variability
A significant limb-by-time interaction effect was observed for activation variability of each quadriceps muscle (P < .001 for all). RF activation variability in the operated limb was 1.57 ± 0.28, 1.40 ± 0.22, and 1.29 ± 0.19 percent of peak EMG (%pEMG) at 4, 6, and 12 months after surgery, respectively, and was significantly reduced with increasing time from surgery (P≤ .02). Significant between-limb differences in RF activation variability were detected at 4 months (MD, 0.29 ± 0.28 %pEMG; P < .001) and 6 months (MD, 0.10 ± 0.25 %pEMG; P = .04) after surgery, with the operated limb demonstrating greater variability (Figure 4A).

Box plots illustrating quadriceps activation variability (as a percentage of the peak 500-ms root-mean-square filtered signal [% pEMG]) of the (A) rectus femoris (RF), (B) vastus lateralis (VL), and (C) vastus medialis (VM) of each limb at 4, 6, and 12 months after surgery. Higher values represent greater signal variability. Error bars extend to minimum and maximum values, and circles denote outliers (identified as values outside of quartile ±1.5 × interquartile range). Significant differences between limbs at each time point are shown by vertical asterisks placed between box plots. Significant differences within limb over time are shown by gray horizontal bars above (operated limb) or black horizontal bars below (nonoperated limb) box plots. *P < .05. **P < .01. ***P < .001.
VL activation variability in the operated limb was 1.75 ± 0.43, 1.55 ± 0.34, and 1.40 ± 0.28 %pEMG at 4, 6, and 12 months after surgery, respectively, which was a significant difference between all time points (P≤ .03). Significant between-limb differences in VL activation variability were detected at 4 months (MD, 0.43 ± 0.41 %pEMG; P < .001) and 6 months (MD, 0.20 ± 0.35 %pEMG; P < .01) after surgery (Figure 4B).
VM activation variability in the operated limb was 1.79 ± 0.41, 1.52 ± 0.22, and 1.45 ± 0.21 %pEMG at 4, 6, and 12 months after surgery, respectively. VM activation variability was significantly reduced between 4 and 6 months (P < .001) and 4 and 12 months (P < .001) but not between 6 and 12 months after surgery. Nonoperated limb VM activation variability was also significantly different between 4 and 6 months after surgery (P < .01) and 6 and 12 months after surgery (P = .03). Significant between-limb differences in VM activation variability were detected at 4 months (MD, 0.45 ± 0.41 %pEMG; P < .001), 6 months (MD, 0.26 ± 0.25 %pEMG; P < .001), and 12 months (MD, 0.11 ± 0.18 %pEMG; P < .01) after surgery (Figure 4C).
Relationships Between Torque Steadiness and Quadriceps Activation Variability
Significant associations between operated limb torque steadiness and quadriceps activation variability were observed for all muscles, such that greater activation variability was associated with more unsteadiness of the torque signal. At 4 months after surgery, operated limb torque steadiness was associated with RF activation variability (rS = 0.65; P < .001), VL activation variability (rS = 0.78; P < .001), and VM activation variability (rS = 0.88; P < .001). At 6 months after surgery, operated limb torque steadiness was associated with VL activation variability (rS = 0.63; P < .001) and VM activation variability (rS = 0.57; P = .001). At 12 months after surgery, operated limb torque steadiness was associated with VL activation variability (rS = 0.49; P < .01) but not RF or VM activation variability (Figure 5).

Scatterplots illustrating the relationships between operated limb quadriceps activation variability of the (A) rectus femoris (RF), (B) vastus lateralis (VL), and (C) vastus medialis (VM) and the operated limb torque steadiness at 4, 6, and 12 months postoperatively. Mean variability for each muscle is displayed on the y-axis as a percentage of the peak 500-ms root-mean-square filtered signal (% pEMG), whereas torque steadiness is displayed on the x-axis as a percentage of peak knee extensor torque (% PT). Spearman r values for the correlation between activation variability and torque steadiness are shown for each muscle and postoperative time period. **P < .01. ***P < .001.
Relationship Between Torque Steadiness and Knee Extensor Peak Torque Symmetry
We observed significant associations between operated limb torque steadiness and peak knee extensor torque symmetry at 4 months (rS = −0.49; P < .01) and 6 months (rS = −0.49; P < .01) after surgery but not at 12 months after surgery (Figure 6).

Scatterplot illustrating the relationship between knee extensor peak torque limb symmetry index (LSI; x-axis) and operated limb knee extensor torque steadiness (y-axis; as a percentage of peak knee extensor torque [% PT]) at 4, 6, and 12 months postoperatively. Higher torque steadiness values represent more unsteadiness or greater signal variability. The Spearman r values for the correlation between torque steadiness and knee extensor peak torque symmetry are shown for each postoperative time period. **P < .01.
Sensitivity Analysis
The sensitivity analysis excluding the 6 athletes with previous ACLR demonstrated no differences in torque steadiness interaction effects or between-limb differences. Further, no discrepancies were found in activation variability interaction effects or between-limb differences for VL and VM activation variability. Marginal statistical changes were seen in RF activation variability between-limb differences (Supplemental Tables S1 and S2).
Discussion
The purposes of this novel investigation were to evaluate knee extensor torque steadiness and quadriceps activation variability in both limbs of collegiate athletes throughout the first year after ACLR and to determine the associations between knee extensor torque steadiness, quadriceps activation variability, and peak torque symmetry. Our primary hypothesis was largely supported: Between-limb differences were observed in knee extensor torque steadiness and quadriceps activation variability at 4 and 6 months after surgery and in VM activation variability at 12 months after surgery. We also observed that operated limb torque steadiness was significantly associated with operated limb activation variability of all quadriceps muscles at 4 months after surgery, with the VM at 6 months after surgery, and with the VL at 6 and 12 months after surgery. Last, we found that operated limb torque steadiness was significantly associated with peak knee extensor torque symmetry at 4 and 6 months after surgery.
This is the first study to investigate the influence of time after ACLR on changes in knee extensor torque steadiness and to evaluate the relationships between underlying quadriceps activation patterns and the consistency of knee extensor torque production in this population. Arthrogenic muscle inhibition contributing to impaired voluntary quadriceps motor output after ACLR is a well-studied topic, 27 but most clinical recommendations for ACLR rehabilitation related to quadriceps inhibition focus on the first few weeks or months after surgery.2,39 The results of the current investigation illustrate that on a group level, the majority of athletes at 6 months after surgery presented with abnormal quadriceps activation patterns and torque steadiness impairments. These findings suggest that interventions to facilitate volitional quadriceps activation or mitigate quadriceps inhibition should be included in standard post-ACLR rehabilitation beyond 3 months after surgery.
On an individual athlete level, assessment of torque steadiness may help individualize rehabilitation approaches in the later stages of rehabilitation (ie, >6 months after surgery). Significant outliers in operated limb torque steadiness were observed at 6 and 12 months after surgery (Figure 3). Unsurprisingly, these outliers presented with considerably greater quadriceps weakness than their peers. Five operated limb outliers at 6 months after surgery had a mean knee extensor peak torque limb symmetry of 51.9% compared with the group mean of 67.5%. Three operated limb outliers at 12 months after surgery had a mean peak torque symmetry of 72.8% compared with the group mean of 87.2%. Patients with persistent torque steadiness impairments may have greater potential to benefit from continued use of interventions to treat arthrogenic muscle inhibition. 24 A more individualized approach has potential to improve both prognosis and rehabilitation outcomes.
Operated limb torque steadiness was significantly associated with quadriceps strength symmetry. This finding is consistent with our hypothesis, given that impairment of voluntary quadriceps activation results in reduced force output and can thus impair response to voluntary strengthening exercises (consistent with the findings of Goetschius and Hart 13 ). Of note, for all athlete collections in which knee extensor peak torque symmetry was >80%, operated limb torque steadiness was <0.67%, with the exception of 1 outlier (81% peak torque symmetry and torque steadiness of 1.34%). Thus, it appears that restoration of knee extensor torque steadiness may be a prerequisite to restore quadriceps strength symmetry after ACLR.
Quadriceps activation variability differed by specific quadriceps muscle. We observed asymmetrical activation variability of the VM at 6 and 12 months after surgery and of the VL at 6 months, with a number of outliers observed at 12 months after ACLR (Figure 4B). In addition, activation variability of the VL and VM was significantly associated with torque steadiness at 4, 6, and 12 (VL only) months after surgery. Comparatively, we observed a significant association between torque steadiness and activation variability of the RF at 4 months only (Figure 5). These findings are consistent with the results of previous investigations reporting more significant neuromuscular impairments of the large uniarticular vasti muscles (VM, VL) than the smaller and biarticular RF.40,42 A recent investigation of quadriceps motor unit discharge patterns in patients approximately 8 months after ACLR found that knee extension strength deficit was related to reduced neural drive to the vasti muscles. 25 Similar to our findings, that previous study reported that neuromuscular deficits of the VL were most closely associated with quadriceps weakness.
In this investigation, we evaluated the torque steadiness of only maximal effort isometric contractions. Previous research suggests a nonlinear relationship between force variability and magnitude of force production. 5 Knee extensor torque steadiness during submaximal efforts may provide additional insight into quadriceps neuromuscular dysfunction after ACLR and should be a target for future research. Previous investigations of quadriceps force or knee extensor torque steadiness in individuals with ACL injury or surgery used a target-matching design, where participants were provided real-time feedback of results and were encouraged to attempt to produce a consistent motor output.26,30,31,33,37 Our study design prevented us from determining whether our participants were capable of reducing unsteadiness with use of real-time feedback. In addition, athletes in our study performed isometric contractions at 90° of knee flexion. Previous research has shown that both mode of contraction 18 and knee joint angle 17 can influence force steadiness. Thus, our results cannot be directly compared with those of studies with divergent knee joint angles or contraction types.
The results of this study have important clinical implications. The ability to produce a consistent motor output is crucial to successful performance of daily and athletic activities. An increase in the variability of force output indicates a motor control issue that could inhibit the ability to execute voluntary limb movements with accuracy and precision. 10 This is of particular importance for high-level athletes, as a fundamental component of success in athletic performance is skilled and effective performance of complex, sports-specific tasks. Our findings suggest that abnormal quadriceps firing patterns are present at 6 months after surgery in the majority of athletes who have undergone ACLR and are associated with persistent quadriceps weakness. Individual outliers, with increased torque unsteadiness associated with more abnormal muscle recruitment patterns, are identified 1 year after surgery and present with more pronounced quadriceps muscle impairments. Individuals with persistent torque steadiness deficits after ACLR may be more likely to benefit from the use of clinical strategies to maximize success in the presence of quadriceps inhibition, such as neuromuscular electrical stimulation, eccentric exercise, contralateral limb training, vibration, focal joint cooling, or other emerging interventions. 24
Limitations
This study is not without limitations. All participants were from a single institution and were a relatively homogeneous population of collegiate student-athletes, which may limit the generalizability of our findings. All athletes completed postoperative rehabilitation in the same sports medicine facility using a standard post-ACLR protocol with unrestricted access to sports medicine facilities and resources. This was a sample of convenience and thus was not appropriately powered to assess potential confounding variables, such as sex, sport, or concomitant surgical procedures. Most athletes in this study underwent ACLR with ipsilateral bone-patellar tendon-bone autografts, but 3 patients had reconstruction with a different graft. Recent investigations have shown differences in quadriceps strength recovery by graft type, with an increased magnitude of quadriceps weakness associated with knee extensor mechanism autografts compared with hamstring tendon autografts.29,34 Quadriceps neuromuscular dysfunction related to torque steadiness may also vary by graft type.
It is well established that ACL injury and ACLR can impair quadriceps strength 38 and activation 36 and lower extremity biomechanics 12 of both limbs. For the specific method used in this study, we did not have a healthy comparison group and consequently do not know what constitutes typical knee extensor torque steadiness and quadriceps activation variability. However, the minimal changes observed from 4 to 12 months after surgery in the nonoperated limb suggest that those values might represent an appropriate goal for the operated limb. We also did not evaluate the correlations between torque steadiness and functional testing results or return-to-sport outcomes, which is a target for future investigations in better understanding the clinical relevance of these measurements. Last, the sample for this study included 6 athletes with secondary ACLR, which has the potential to influence the results due to contralateral injury or the compounding effects of repeat injury or surgery. However, when we excluded the data of these 6 athletes, none of our primary torque steadiness or activation variability outcomes changed, with the one exception being that between-limb asymmetry in RF activation variability at 6 months after surgery was no longer significant. As a result, we elected to include the data from these participants in our analysis.
Conclusion
Impaired knee extensor torque steadiness of the operated limb was observed 6 months after ACLR in NCAA Division I collegiate athletes, whereas quadriceps activation patterns associated with reduced torque steadiness were observed up to 1 year after surgery. Involved limb torque steadiness and quadriceps activation variability improved from 4 to 12 months after surgery. Reduced torque steadiness of the operated limb was associated with quadriceps strength asymmetries. Clinical assessment of knee extensor torque steadiness in patients after ACLR may improve prognosis and help improve specificity of rehabilitation efforts.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241253843 – Supplemental material for Knee Extensor Torque Steadiness and Quadriceps Activation Variability in Collegiate Athletes 4, 6, and 12 Months After ACL Reconstruction
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241253843 for Knee Extensor Torque Steadiness and Quadriceps Activation Variability in Collegiate Athletes 4, 6, and 12 Months After ACL Reconstruction by Daniel G. Cobian, Zachary R. Oppenheim, Tyler J. Roehl, Mikel R. Joachim and Bryan C. Heiderscheit in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted October 25, 2023; accepted November 16, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.C.H. has received consulting fees from Biocore, is an advisory board member for Springbok Analytics, and has an ownership interest in Science of Running Medicine LLC. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The University of Wisconsin–Madison (ref No. 2018-0049).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.