
Abstract
Background:
Atrophy and fatty infiltration of the supraspinatus (SS) muscle are prognostic indicators of poor functional outcomes and higher retear rates after rotator cuff repair. While older patients, female patients, and those with massive and retracted rotator cuff tears are at a higher risk for these indicators, it is unclear whether tear characteristics, acromion morphology, and acromioclavicular (AC) joint arthritis affect SS atrophy in older patients with chronic shoulder pain.
Purpose:
To investigate the multifactorial influences associated with SS atrophy in rotator cuff tears.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A review was conducted on 391 patients with atraumatic shoulder pain (mean age, 60.88 ± 8 years; range, 50-93 years; 200 men and 191 women) who underwent magnetic resonance imaging between May 2019 and April 2020. SS atrophy was calculated using the occupation ratio. Logistic regression was performed to evaluate the association of SS atrophy with patient age and sex, rotator cuff tear type (partial- vs full-thickness), anteroposterior (AP) tear size, AC and glenohumeral (GH) joint arthritis, and acromion shape. A subgroup analysis was performed in patients without tears to investigate whether SS atrophy and fatty infiltration were independent phenomena.
Results:
Overall, 91 patients had full-thickness tears without retraction, 131 had partial-thickness tears, and 169 had no tears. The prevalence of SS atrophy was associated with patient age and was more prevalent in women (67.6%), full-thickness tears (91.1%), an AP tear size of >15 mm (92.6%), and GH joint arthritis (100%) (P < .001 for all). The severity of atrophy (indicated by a decrease in the occupation ratio) increased with older age. In the patients without tears, SS atrophy prevalence was 33.1%. Logistic regression analysis showed significant independent associations of SS atrophy with age (P < .001), female sex (P < .001), nonretracted full-thickness tears (P < .001), an AP tear size of >15 mm (P < .001), and hook-shaped acromion (P = .007). A subgroup analysis of the nontear group revealed a significant association of SS atrophy with fatty infiltration (P < .001).
Conclusion:
This study identified significant associations between SS atrophy and older age, female sex, full-thickness tear without retraction, an AP tear size of >15 mm, and hook-shaped acromion. Notably, partial-thickness tears were not significantly associated with SS atrophy.
Keywords
Supraspinatus (SS) muscle atrophy and fatty infiltration are prognostic indicators associated with poor functional outcomes and higher recurrence tear rates after rotator cuff repair.12,14,22,27,28,36,37 Furthermore, atrophy and fatty infiltration adversely affect functional outcomes after anatomic shoulder arthroplasty.7,20,30,38,43 The natural history of fatty infiltration and atrophy is described as progressive and irreversible.6,14,15 Although these changes are irreversible, repair appears to halt the progression of atrophy.11,12 The presence of atrophy and fatty infiltration in massive or full-thickness tears of the rotator cuff with retraction has been established; nonetheless, it is still unclear exactly how these changes occur, what causes them, and whether they are correlated or separate injury responses.9,13,16,18,24,42 Aging and female sex are risk factors for both atrophy and fatty infiltration. However, it is unknown how radiological parameters—such as rotator cuff tear characteristics, acromioclavicular (AC) joint arthritis, and morphology of the acromion—affect the development of atrophy.
In the present study, we evaluated the prevalence of SS atrophy in patients ≥50 years old with atraumatic shoulder pain to determine the association of degree of SS atrophy and fatty infiltration to factors such as SS tear type, tear thickness, glenohumeral (GH) joint arthritis, AC joint arthritis, and acromion morphology. We also hypothesized that SS atrophy and fatty infiltration are 2 separate and independent phenomena.
Methods
Participants
This cross-sectional study was approved by our institutional review board. We reviewed the Picture Archiving and Communication System (PACS) at our hospital for magnetic resonance images (MRIs) of the shoulder joint performed between May 2019 and April 2020. All MRIs were performed using our standard protocol in neutral rotation based on the plane of the scapula allowing true coronal and axial measurements at the glenoid, with slice thickness set to 3 mm. We evaluated (1) sagittal oblique proton density-weighted fast spin-echo (FSE), (2) coronal-oblique T1-weighted FSE sequences, and (3) coronal-oblique, axial, and sagittal-oblique T2-weighted FSE sequences with fat suppression. All scans were performed using a 3-T system (Discovery MR750w GEM; GE Healthcare).
Included were MRIs of patients ≥50 years old with chronic shoulder pain. Excluded were MRIs from patients ≤50 years old and those with acute shoulder pathologies (trauma, fracture, and calcific tendinitis), neoplastic conditions, previous history of shoulder surgery with metallic implants, and neurological disorders (eg, Turner parsonage syndrome).
Sample Size
A sample size of 380 was estimated using the method described by Hsieh et al 17 and was determined using the a priori test for logistic regression with G*Power software (Heinrich-Heine-Universität Düsseldorf). This calculation took into account a medium effect size (0.405) and a desired power of 0.95 for the primary outcome of SS atrophy. Furthermore, a post hoc analysis was conducted to confirm the statistical power of the study.
A total of 655 shoulder MRIs were initially reviewed. Of these, 264 scans were excluded based on our criteria and sagittal oblique MRIs that lacked adequate scapular Y-views, leaving 391 scans in 391 patients for analysis.
Data Collection
The age and sex of the patient were recorded. The MRI scans were assessed using the RadiAnt Digital Imaging and Communications in Medicine (DICOM) software (Mexidant), which was provided with the PACS workstation. The following parameters were assessed:
SS tear type and anteroposterior (AP) tear size
SS atrophy and fatty infiltration
GH joint arthritis
AC joint arthritis
Acromion morphology
Two assessors (K.S.M. and M.M.D.)—an orthopaedic senior resident and a senior shoulder surgeon, respectively—independently reviewed each MRI scan. Instances where discrepancies arose between them were judiciously reconciled through consensus discussions involving a qualified radiologist who was not involved in the study.
Supraspinatus Tear Type and AP Tear Size
SS tears were evaluated on coronal T2-weighted and proton density-weighted MRI sequences with and without fat suppression. Retracted and massive rotator cuff tears were excluded. Massive rotator cuff tears were defined as larger full-thickness tears involving >1 tendon, according to Gerber et al, 12 and as tears of >5 cm, according to Cofield. 8 SS tears were graded as follows: (1) normal; (2) partial-thickness, which was further classified based on location into bursal, articular, or intrasubstance (intratendinous)10,25,34; or (3) full-thickness without retraction. AP tear size was measured on T2-weighted axial MRI sequences.
Supraspinatus Atrophy and Fatty Infiltration
SS atrophy was measured using the occupation ratio, 40 which is the ratio of the SS muscle belly area to the area of the SS fossa on Y-view MRI. The Y-view is the oblique sagittal plane that crosses the scapula through the medial border of the coracoid process, where the body of the scapula, scapula spine, and medial border of the coracoid are shown; here, the SS fossa is mostly limited by bone. Using the closed polygon tool provided in the RadiAnt DICOM viewer, the boundary of the SS muscle belly was drawn along the muscle's outer border, and the SS fossa was drawn along the inner margins of the Y; the superior limit of the SS fossa was demarcated by the distal clavicle and a line drawn between the distal clavicle anteriorly and the scapular spine posteriorly. The SS muscle was considered normal if the occupation ratio was ≥0.6; moderately atrophic if between 0.59 and 0.40, and severely atrophic if <0.40 (Figure 1). 24

Sagittal oblique T1-weighted magnetic resonance imaging scans at the level of the scapular-Y view. Calculation of the occupation ratio using (A) the closed polygon tool and (B) the negative tool in the RadiAnt Digital Imaging and Communications in Medicine viewer to confirm the slice showing the bony landmark.
SS fatty infiltration was graded on T1-weighted sagittal oblique Y-view MRI using the classification of Goutallier et al, 15 in which grade 0 indicates no atrophy, grade 1 some fatty streaks in the muscle, grade 2 significant fatty infiltration but less than muscle, grade 3 equal amounts of muscle and fat, and grade 4 fat more than muscle. Goutallier grade ≥2 was considered as substantial fatty infiltration (Figure 2).

Sagittal oblique proton density-weighted magnetic resonance imaging sequence showing Goutallier grading of supraspinatus fatty infiltration. (A) No fatty infiltration. (B) Fatty streaks. (C) Substantial fatty infiltration (grade ≥2).
Joint Osteoarthritis and Acromion Morphology
The MRIs were evaluated for signs of AC joint arthritis—capsular thickening of >4 mm, presence of osteophytes, subchondral cysts, bone marrow edema, and contour irregularities. 39 GH joint arthritis was classified with the Samilson and Prieto method, 35 in which a grade of ≥2 signified the presence of arthrosis. Rotator cuff arthropathy and posttraumatic arthritis were excluded. In addition, sagittal oblique MRI scans lateral to the AC joint were assessed for acromion morphology, which was classified as curved, flat, hooked, or convex according to the modified Bigliani classification.5,26,41
Measurement Reliability
Table 1 shows the intraclass correlation coefficients with confidence intervals for the interrater reliability of the various measurements. The results indicated excellent agreement between the 2 reviewers.
Interrater Reliability of the MRI Measurements a

AP, anteroposterior; ICC, intraclass correlation coefficient; MRI, magnetic resonance imaging; SS, supraspinatus.
Statistical Analysis
Statistical analysis was performed using the chi-square test for categorical and ordinal variables. P < .05 was considered statistically significant. Data were tested for normal distribution using the Kolmogorov-Smirnov goodness-of-fit test. Multiple logistic regression analysis was performed for the dependent and independent variables, with Nagelkerke R2 used as the coefficient of determination. Reported values for each independent variable included the coefficient (β) of the logistic regression fit and the odds ratio (OR) calculated from determined coefficients (OR = eβ) with associated 95% CIs. Bonferroni correction for multiple comparisons was applied for P values and confidence intervals.
Results
Among the 391 patients included in the study, 200 (51.2%) were men and 191 (48.8%) were women, with a mean age of 60.88 years (range, 50-93 years). The demographic profile (age and sex distribution) and tear characteristics are summarized in Table 2. Age-wise distribution of the tear characteristics is summarized in Figure 3.
Characteristics of the Study Cohort (N = 391 Patients) a

Data are presented as n (%). AC, acromioclavicular; AP, anteroposterior; GH, glenohumeral; SS, supraspinatus.
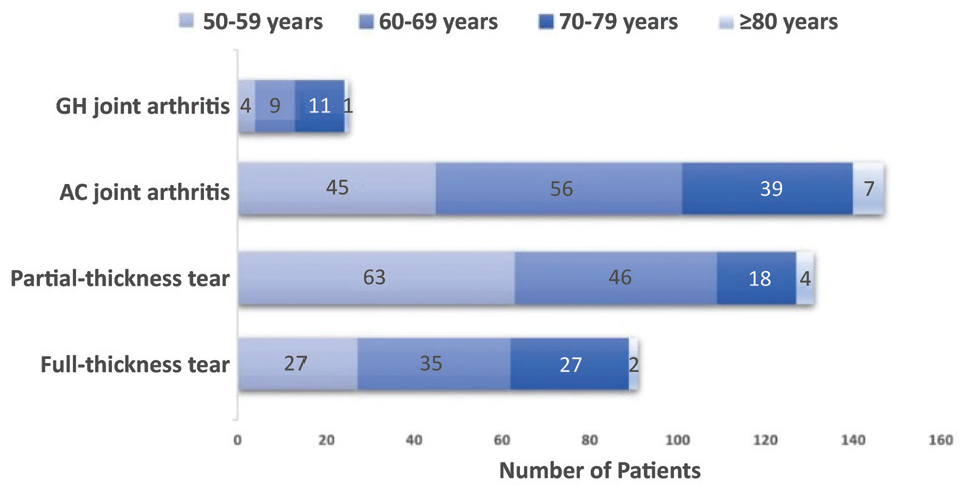
Distribution of tear characteristics according to patient age groups. AC, acromioclavicular; GH, glenohumeral.
The prevalence of SS atrophy was 50.1% (severe atrophy, 11%; moderate atrophy, 39.1%), while the prevalence of substantial fatty infiltration (Goutallier grade ≥2) was 27.4%. The SS atrophy was found to be the highest among patients with full-thickness tears (91.1%), an AP tear size of >15 mm (90.3%), female patients (67.6%), and those with GH joint arthritis (100%). In patients without SS tears (no tear group; n = 169), the prevalence of SS atrophy was 33.1% (moderate atrophy, 27.8%; severe atrophy, 5.3%). A breakdown of SS atrophy prevalence is summarized in Table 3.
Prevalence of Supraspinatus Atrophy a

Data are presented as n (%) unless otherwise indicated. AC, acromioclavicular; AP, anteroposterior; GH, glenohumeral.
A significant association between patient age and prevalence of SS atrophy was noted (P < .001). The severity of atrophy (indicated by a decrease in the occupation ratio) increased with older age—the mean age of patients with severe SS atrophy was 66.11 years, compared with 62.71 years in patients with moderate atrophy and 58.29 years in patients with no atrophy. The linear-fit trendline (Figure 4) also showed a similar relationship between age and SS atrophy, depicting a trend toward decreasing occupation ratio regardless of whether there was no tear, partial-thickness tear, or full-thickness tear (R2 = 0.0369). However, the slope of the occupation ratio tended to be higher for patients with full-thickness tears (R2 = 0.0805) versus no tears (R2 = 0.0369) and modestly higher for patients with partial-thickness tears (R2 = 0.0454) versus no tears. No significant association was found between partial-thickness tears and SS atrophy (articular-sided tear, P = .61; bursal-sided tear, P = .39; intrasubstance tear, P = .46; χ2 test).

The relationship between supraspinatus atrophy and age in patients with no tear, partial-thickness tear, and full-thickness tear. Linear-fit trendline and coefficient of determination (R2) are shown for each group.
A significant association was found between SS atrophy and female sex (prevalence, 67.6% in women vs 33.5% in men; P < .001) (Table 3). Female patients also had a higher prevalence of severe atrophy (10% vs 5% in male patients). The association was independent of SS tears (SS atrophy prevalence in the no-tear group: 47.3% in women vs 22.1% in men; P < .001). Moreover, female patients exhibited more severe atrophy than male patients, as demonstrated by the linear-fit trendline (female patients without SS tears, R2 = 0.017 vs male patients, R2 = 0.117) (Figure 5).

The relationship between supraspinatus atrophy and patient age in female and male patients with no-tear. Linear-fit trendline and coefficient of determination (R2) are shown for each group.
All patients with GH joint arthritis exhibited SS atrophy (severe, 68%; moderate, 32%; P < .001). In addition, we observed a significant association between SS atrophy and hook-shaped acromion (P < .001). SS atrophy was not associated with AC joint arthritis (P = .14).
A multivariate regression analysis was conducted with SS atrophy (defined as present if the occupation ratio was <0.6) as the dependent variable. A negative outcome was considered to be the presence of atrophy. We could not perform regression analysis with GH joint arthritis as an independent variable due to multicollinearity. Table 4 shows the results of the regression analysis for each independent and dependent variable tested. Age >50 years (OR, 1.059; P < .001), female sex (OR, 4.208; P < .001), full-thickness SS tear (OR, 18.781; P < .001), hook-shaped acromion (OR, 3.200; P = .007), and an AP tear size of >15 mm (P < .001) were independently and significantly associated with SS atrophy.
Results of Logistic Regression for Factors Associated With SS Atrophy a

The logistic regression model was statistically significant (χ2 = 167.1; P < .001; R2 = 0.46). Post hoc power analysis reported a power of 0.942. Overall model fit: χ2 = 0.4637; P < .001; R2 = 0.2133. Bold P values indicate statistical significance (P < .05). AC, acromioclavicular; AP, anteroposterior; OR, odds ratio; SS, supraspinatus.
To elucidate the relationship between fatty infiltration and atrophy irrespective of SS tear, a subgroup analysis was conducted on the 169 patients in the no-tear group (Figure 6). In this subgroup, the prevalence of SS atrophy increased with increasing fatty infiltration grade—15.2% of patients with grade 0, 95.8% of patients with grade 1, and 100% with grade 2 fatty infiltration had SS atrophy. Multivariate analysis in this subgroup showed that age (OR, 0.011; P = .001), female sex (OR, 1.686; P = .002), and hook-shaped acromion (OR, 1.838; P = .037) were independently and significantly associated with SS atrophy. Table 5 summarizes the results of the logistic regression analysis for this subgroup.

The relationship between supraspinatus atrophy and fatty infiltration in the no-tear group (n = 169).
Results of Subgroup Analysis in the No-tear Group a

Overall model fit: χ2 = 28.15; P < .001: R2 = 0.2133; post hoc power = 0.891. Bold P values indicate statistical significance (P < .05). AC, acromioclavicular; OR, odds ratio.
Discussion
The overall prevalence of SS atrophy was 50.1% and the prevalence of substantial fatty infiltration (Goutallier grade ≥2) was 27.4% in our study cohort of patients ≥50 years old with shoulder pain. The prevalence of moderate and severe SS atrophy was 39.1% and 11%, respectively.
Melis et al 27 used the positive tangent sign to measure SS atrophy and reported a 13.9% prevalence of SS atrophy and 34% of fatty infiltration in patients with rotator cuff tears. The tangent sign 44 is widely used to assess SS atrophy and allows for quick qualitative assessment. Lim et al 23 concluded that the tangent sign distinguishes mild from severe atrophy, but it does not predict moderate atrophy, as we were able to do with the occupation ratio. Barry et al 4 reported an estimated prevalence of atrophy of 36.1% in groups without tears and 77.6% in groups with complete (full-thickness tears). Our findings suggest a high prevalence of atrophy among patients ≥50 years old without massive or retracted rotator cuff tears in contrast with these previously reported prevalence rates.
Multivariate analysis revealed that age, sex, tear type, AP size, and hooked acromion were independently associated with SS atrophy, regardless of the degree of cuff tearing. All patients with GH joint arthritis had SS atrophy. Older women with full-thickness tears and hooked acromion were more likely to show SS atrophy. The presence of partial-thickness tears and AC joint arthritis did not predict atrophy in partial rotator cuff tears.
In contrast to the findings of Barry et al, 4 we observed that full-thickness tears without retraction were associated with SS atrophy when compared with groups without tears. While Barry et al reported that SS tears—including full-thickness tears—did not predict muscle atrophy, they found a significant association between tear severity and fatty infiltration. Rulewicz et al 33 reported a strong correlation between SS atrophy and tear size, in agreement with our findings.
We evaluated the effect of aging on atrophic changes in patients without rotator cuff tears. The prevalence of muscle atrophy increased with age in patients without rotator cuff tears. This finding is supported by previous muscle studies demonstrating that the aging process can result in a loss of muscle mass with subsequent replacement with fat and connective tissue.21,32
We could not confirm our hypothesis that fatty infiltration and atrophy are 2 separate and independent pathologic processes resulting from tears in the SS. Multivariate regression analysis suggested that SS atrophy and fatty infiltration are associated phenomena after accounting for other independent variables—including age, sex, and tear characteristics. The cause of fatty infiltration and rotator cuff atrophy is complex and not completely elucidated. Both mechanical unloading and denervation, likely play a role in the development of muscle atrophy and fatty infiltration. 19 At a tissue level, full-thickness tears can result in retraction and the development of fatty infiltration via irreversible architectural changes in the musculature. The SS becomes more medialized after a severe tear and retraction. As a result, the suprascapular nerve is subjected to increased tension as it passes through the suprascapular notch, leading to denervation. 1
We observed that hook-shaped acromion is also associated with the development of atrophy. This could be due to a higher association of hooked acromion with full-thickness tears. Andrade et al 2 in their meta-analysis concluded that a larger critical shoulder angle, 29 higher acromion index, 31 lower lateral acromion angles, 3 and a hook-shaped acromion 5 are significantly associated with degenerative full-thickness rotator cuff tears.
Gladstone et al 14 and Gerber et al 12 reported that successful repair did not lead to improvement or reversal of muscle degeneration and a failed repair resulted in significantly more progression. Melis et al 27 suggested poorer outcome with rotator cuff repair with SS atrophy and suggested repair should be performed before the appearance of fatty infiltration (Goutallier grade ≥2) and atrophy (positive tangent sign)—especially when the tear involves multiple tendons. Age-related muscle atrophy may explain the higher failure rates observed in rotator cuff repair with increasing age. Hence, nonoperative approaches should be considered for patients exhibiting these irreversible changes.
Strengths and Limitations
Our study had the following strengths: (1) we selected patients ≥50 years old without massive and retracted tears, which would bias the data toward a higher prevalence rate; (2) MRI was performed at a single facility using a 3-T magnet, which has a better signal-to-noise ratio compared with 1.5-T and is of higher quality; and (3) the relationship between multiple factors was evaluated using multivariate modeling. The relationship between fatty infiltration and rotator cuff atrophy as well as the radiological factors that influence this process may assist orthopaedic surgeons in improving and providing patients with better prognosis information. The study also aids in understanding the various factors associated with the atrophy of the SS muscle, which in turn may help in predicting the failure rates.
Our study had several limitations—including its retrospective cross-sectional nature and its incapability to establish temporal relationships between variables. The study does not represent a prevalence of all patients ≥50 years old, but those with shoulder pain.
Conclusion
This study identified significant associations between SS atrophy and older age, female sex, full-thickness tear without retraction, an AP size of >15 mm, and hook-shaped acromion. Notably, partial-thickness tears did not show a significant association with atrophy. Among patients without rotator cuff tears, atrophy increased with age and female sex independently.
Footnotes
Final revision submitted May 29, 2024; accepted June 14, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seth G.S. Medical College and King Edward Memorial Hospital (reference No. EC/215/2019).