
Abstract
Background:
Superior labrum anterior-posterior (SLAP) lesions are common shoulder injuries. The 10-type classification system has been widely used to diagnose SLAP lesions since it was proposed. However, growing evidence from arthroscopic studies indicates the existence of many SLAP lesions, especially those associated with superior glenoid humeral ligament (SGHL) injuries, that were not included in the initial classification.
Purpose:
To introduce a SLAP classification associated with SGHL injury based on arthroscopic views and discuss the injury mechanism and corresponding treatment options.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Patients with SLAP lesions who underwent shoulder arthroscopic surgical treatment between June 2011 and January 2017 in 6 level 1 centers were evaluated in this study. Preoperative radiographs and magnetic resonance imaging scans were used to diagnose SLAP lesions, and arthroscopic views from the standard posterior portal were recorded. The traditional 10-type classification system for SLAP was used to classify these cases. A classification method for SLAP lesions associated with SGHL injury was introduced. This classification system was investigated by 4 observers to evaluate inter- and intraobserver reliability (kappa coefficient [κ]).
Results:
A total of 828 patients were included in this analysis; 61 patients (7.4%) could not be classified by the 10-type traditional classification, and 44 patients (5.3%) had SGHL lesions. A novel classification for 3 subtypes of SLAP with SGHL lesions was introduced. The mean κ value of the interobserver reliability for the classification approach was 0.796 (range, 0.678-0.854), indicating substantial agreement. The mean κ value for the intraobserver reliability was 0.883 (range, 0.779-0.964), indicating excellent agreement.
Conclusion:
This study demonstrated a novel classification system for SLAP lesions associated with SGHL injury by introducing a series of cases with characteristics that showed high inter- and intraobserver reliability. Such cases have not been reported before, and the classification correlates with surgical treatment. This classification may be used as a supplement to the traditional 10-type classification.
Keywords
Superior labrum anterior-posterior (SLAP) lesions are common shoulder injuries. 3 Snyder et al 17 made the first classification system for SLAP lesions in 1990, comprising types 1 to 4. Maffet et al 13 described SLAP lesion types 5 to 7 in 1995, and Powell et al 16 described lesions 8 to 10 in 2004.
In some cases of SLAP tears, the superior glenoid humeral ligament (SGHL) can be involved in the injury and plays an important role in stabilizing the shoulder joint and preventing excessive movement of the humeral head within the glenoid fossa, with tears leading to instability and pain in the shoulder. 8 However, very few studies have focused on SLAP tears with SGHL tears.
It has been our observational experience that different SLAP tears may not be included in the existing 10 classifications. We have seen cases in which the SGHL is associated with the SLAP tear that may not be considered in the current classification described. Based on our experience, we felt it was important to present a novel new classification because the SLGH is an important stabilizing ligament in the glenohumeral joint.
The purpose of our study was to introduce a SLAP classification associated with SGHL injury based on arthroscopic views and discuss the injury mechanism and corresponding treatment options. We hypothesized that there would be SGHL injury-related classifications in the SLAP classification.
Methods
A retrospective analysis was conducted and included 828 patients with SLAP lesions who were treated with shoulder arthroscopic surgery at 6 hospitals between June 2011 and January 2017. Patients were identified by diagnosis as defined by the International Classification of Diseases, 9th Revision (codes 840.7 [lesion superior glenoid labrum] and 840.8 [tear superior glenoid labrum]) and 10th Revision (codes S43.431 [SLAP lesion of right shoulder], S43.432 [SLAP lesion of left shoulder], and S43.439 [SLAP lesion of unspecified shoulder]). This study was approved by the Chinese PLA General Hospital Institutional Ethics Committee (S2021-19-01).
Patients >18 years of age who underwent surgical treatment for isolated SLAP lesions were included. Patients who received nonoperative treatment and those with concurrent injuries or previous shoulder surgery were excluded from the study. Magnetic resonance imaging (MRI) scans were used to aid in the diagnostic process, providing valuable imaging information. The patients themselves provided information regarding the mechanism of their injuries. T2-weighted axial and coronal MRI sequences (Skyra 3.0-T; Siemens) were used to assist in diagnosis.
The physical examination included 3 examination areas: biceps, labrum, and anterior instability of the glenohumeral joint.7,14 The biceps examination included the Yergason test,6,15 biceps palpation, the biceps tension test,5,15 and the load test 2.9,15,19 The labrum examination comprised the O’Brien test,5,15 compression rotation, 15 and the O’Driscoll test.6,15 The anterior stability examinations included the anterior drawer test and the surprise/release test. 17 The physical examinations were conducted as described in the literature and performed by experienced shoulder surgeons (Q.Z. and F.Z.)
SLAP classification was conducted according to Snyder et al 17 (types 1-4), Maffet et al 13 (types 5-7), and Powell et al 16 (types 8-10) types. The previous classifications are summarized in Figure 1. The patients’ sex, age, positive physical examination findings, injury mechanism, arthroscopic view from the standard posterior portal, and SLAP classification were recorded, with a probe to determine labrum stability.
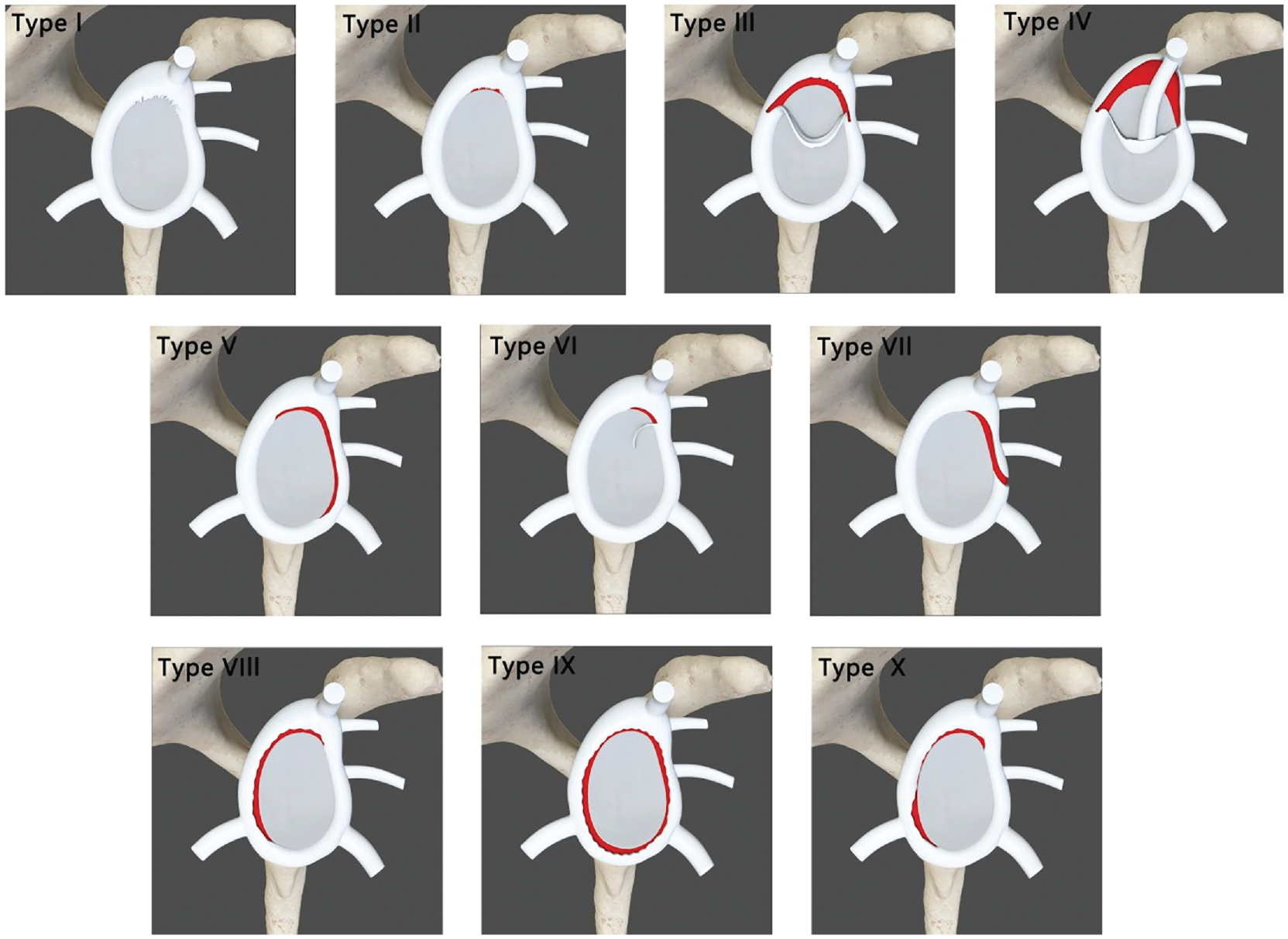
Existing superior labrum anterior-posterior classification. I Fraying of the superior labral attachment with intact biceps and labral attachment II Non-variational detachment of the superior labrum along with the long head biceps tendon III A detached proximal superior labrum displaced into the articular surface. Also referred to as ‘bucket handle’ IV A ‘bucket handle’ tear of the whole labrum with partial displacement of the biceps tendon into the articular surface V An anterior-inferior lesion (Bankart) that extends superiorly reaching the biceps tendon VI An unstable labral attachment with biceps tendon anchor release VII Superior labral tear that extends to the middle glenohumeral ligament VIII Superior labral lesion extending posteriorly and reaching the 6 ‘o’clock’ position IX A ‘pan-labral’ tear involving the whole circumference X A reverse Bankart tear reaching the superior labrum
Statistical Analysis
Four observers (Y.P., F.Z., W.Q. and J.L.), who were sports medicine postresidency professionals with >5 years of experience in shoulder sports medicine training, were recruited for the classification of SLAP lesions in 828 cases using the classification systems. The relevant arthroscopic views were provided by the 6 level 1 centers. It is important to note that the observers did not participate in any arthroscopic surgeries performed on the patients included in this study. Before the classification task, the observers underwent training on the SLAP standard 10-type classification system. They were then instructed to complete a questionnaire based on the arthroscopic view, utilizing the 10-type SLAP classification system. This was then repeated in 1 week. To ensure impartiality, the observers were blinded to the patients’ personal information as well as the order of the views.
We classified the SGHL-associated SLAP injuries into 3 subtypes as depicted in Figure 2. Type A refers to a labrum tear between the long head of the biceps tendon (LHBT) and SGHL with a stable SGHL. Type B refers to a labrum rupture between the LHBT and SGHL and displacement anterior to the SGHL. Type C refers to a labrum bucket-handle tear along the SGHL. Types B and C can be seen in Supplemental Videos S1 and S2.

Superior labrum anterior-posterior–superior glenohumeral ligament (SGHL) lesion subclassification with (A-C) schematics and (a-c) arthroscopic photographs as viewed from the posterior portal with the patient in the lateral position. (A) Type A labrum tear between the long head of the biceps tendon (LHBT) and SGHL. (B) Type B labral tear between the LHBT and SGHL with displacement anterior to the SGHL. (C) Type C labrum bucket-handle tear along the SGHL. HH, humeral head; SL, superior labrum.
The novel SLAP with SGHL injury classification system was analyzed using SPSS software Version 22.0 (IBM Corp). Intraobserver and interobserver levels of agreement based on kappa (κ) values were evaluated according to the guidelines proposed by Landis and Koch, 12 which assigned subdivisions according to the strength of agreement: slight agreement (0.01-0.20), fair agreement (0.21-0.40), moderate agreement (0.41-0.60), substantial agreement (0.61-0.80), and excellent agreement (0.81-1.00).
Results
A total of 828 patients were found to have a SLAP tear from our initial search; 61 patients (7.4%) could not be classified by the traditional 10-type classification system. We found that 44 patients (5.3%) had a SLAP tear associated with an SGHL injury. There were 28 male and 16 female patients with a mean age of 32.14 years (range, 18-46 years). Patient characteristics and physical examinations are shown in Table 1.
Patient Characteristics and Physical Examinations a

F, female; M, male; + means the test result is positive.
We classified these lesions into 3 subtypes: A, B, and C. Type A (27.3%) represented labrum tears between the LHBT and SGHL. In this type, the LHBT and SGHL anchors were stable. Type B (47.7%) represented a labrum rupture between the LHBT and SGHL and labrum displacement anterior to the SGHL. In this type, the LHBT and SGHL anchors were both unstable; if the humerus shifted anteriorly, the labrum was displaced anteriorly. Type C (25%) represented labrum bucket-handle tears along the SGHL. In this type, the LHBT has a stable supraglenoid tubercle, and the SGHL anchor is detached from the labrum. These 44 patients underwent the O’Brien test, Yergason test, biceps palpation test, compression rotation, biceps tension test, biceps load test 2, O’Driscoll test, anterior drawer test, and surprise/release test. Table 2 summarizes the physical examination findings.
Positive Rates of Physical Examination

Interobserver Agreement
The mean κ value for the interobserver reliability of the novel classification was 0.796 (range, 0.678-0.854), indicating substantial agreement.
Intraobserver Agreement
The mean κ value for the intraobserver reliability of the novel classification was 0.883 (range, 0.779-0.964), indicating excellent agreement.
Discussion
This study identified a range of SLAP lesions accompanied by SGHL injuries and established a novel classification system to organize these lesions based on their specific locations around the LHBT and SGHL. We classified these lesions into 3 subtypes: A, B, and C. Type A will not cause instability of the labrum but may progress to type B. Type B may cause glenohumeral joint anterior instability because the SGHL is unstable, and anterior labrum detachment could progress to the middle glenohumeral ligament (MGHL). Type C, which is more frequently seen in a meniscus-type labrum, will cause anterior and posterior labrum detachment. We found that 44 patients (5.3%) had a SLAP tear associated with an SGHL injury. Type A (27.3%) represented labrum tears between the LHBT and SGHL. In this type, the LHBT and SGHL anchors were stable. Type B (47.7%) represented a labrum rupture between the LHBT and SGHL and labrum displacement anterior to the SGHL. In this type, the LHBT and SGHL anchors were both unstable; if the humerus shifted anteriorly, the labrum was displaced anteriorly. Type C (25%) represented labrum bucket-handle tears along the SGHL. In this type, the LHBT has a stable supraglenoid tubercle, and the SGHL anchor is detached from the labrum. Most of the biceps examinations showed positivity in all 3 subtypes. The Yergason test was more sensitive than the other tests. All 3 labrum examinations showed high sensitivity in the 3 subtypes. Subtype B showed 57% to 76% anterior instability in physical examinations, and very few subtype C cases showed anterior instability. This classification aids surgeons in gaining a deeper understanding of injury patterns, facilitating treatment planning, and predicting patient outcomes.
SLAP lesions are common shoulder injuries, and many classification types have been described. The primary classification of SLAP lesions was reported by Snyder et al 17 in 1990 and consists of 4 classic types. The number of arthroscopic surgeries has increased, and our understanding of SLAP lesion pathology has progressed; 10 types of SLAP classifications have now been described. 14 All the classifications focus on the range of the lesion, LHBT, Bankart injury, biceps-labrum anchor, and MGHL. None of them focus on SGHL. In this study, we found that 5.3% of SLAP cases were associated with SGHL. Some of these cases have pain and anterior instability of the glenohumeral joint. These cases cannot be classified using the previous system. Bencardino et al 1 described a kind of SLAP tear at the 2000 meeting of the Radiological Society of North America as a superior labral tear that not only involves the origin of the biceps tendon but also extends to involve the rotator interval structures. However, these descriptions were based on MRI scans, and no arthroscopic view was discussed. SLAP lesions can also cause glenohumeral joint anterior instability. This kind of SLAP lesion has some common pathology and mechanical injuries. We propose that this characteristic should be noted by surgeons. The SLAP injury should be repaired during surgery to reduce the probability of recurrence of postoperative glenohumeral instability and pain.
There are many stable structures on the labrum, including the SGHL, MGHL, LHBT, anterior inferior glenohumeral ligament (IGHL), and posterior IGHL. There are similar anchors for the whole labrum. Injury to one of these anchors will destabilize the labrum. The center of the SLAP lesion, which represents the SLAP, is located from the 11-o’clock position to the 1-o’clock position. The SGHL originates from the upper part of the glenoid cavity and the base of the coracoid process, forms a part of the superior labral complex, along with the superior region of the glenoid labrum and the biceps tendon, and inserts on the humerus near the proximal tip of the lesser tuberosity on the medial ridge of the intertubercular groove.7,10 The SGHL forms an anterior cover around LHBT, and the attachment on the labrum is primarily to the biceps tendon attachment on the supraglenoid tubercle. 2 The traditional classification noted the crucial role of labrum anchors (type 6) but did not relate it to the SGHL and its anchor. We used a probe to examine the labrum stability during the arthroscopic surgery and found that detached SGHL caused instability in patients. We found that the SGHL and its anchor play an important role in stability in some SLAP lesions and classified them accordingly. The SGHL plays a crucial role in ensuring stability for both the glenohumeral joint and the biceps. 11 A biomechanical study demonstrated that the SGHL contributes to glenohumeral stability when the arm is in adduction and undergoing progressive external rotation. 4 Acting as an intra-articular capsular reinforcement within the rotator interval, the SGHL has a close association with the intra-articular portion of the LHBT before it inserts at the fovea capitis. 4 This relationship between the SGHL and the biceps pulley aids in the proper alignment and functioning of the biceps tendon. 4 The biceps-labral complex is formed by the LHBT and the glenoid labrum. The complex is further divided into 3 distinct zones: inside, junction, and bicipital tunnel. 18 We consider that the SGHL-labrum complex also has an SGHL anchor on the superior anterior labrum. Therefore, the most important stability structures in this range were LHBT at the 12-o’clock position and SGHL at the 1-o’clock position. We propose that this area could be referred to as the LHBT-SGHL-labrum complex.
The LHBT and SGHL anchors are the most crucial in terms of stability for SLAP lesions. 11 Most SLAP lesions are posterior to the biceps anchor, but we found a series of cases that were anterior. Many studies have focused on the LHBT, but very few have focused on the SGHL.4,20 The combination of the SGHL with the static stabilizers of the shoulder and the rotator cuff is believed to involve the biceps in shoulder stability. However, the specific role of the SGHL in providing superior stability and its function as an anchor for SLAP lesions have not been completely clarified.
The mean κ value for the intraobserver reliability of the novel classification was 0.883 (range, 0.779-0.964), indicating excellent agreement. The results of this study showed that the inter- and intraobserver agreement have satisfactory reliability in our classification, and it is easy to remember, communicate, and use to guide surgery.
The treatment principle for this kind of SLAP injury is first to stabilize the labrum ring, second to stabilize the ligament anchors, and third to stabilize the labrum. The stability of the labrum has been discussed less frequently in the context of SLAP lesions. We suggest that the stability of the labrum should be noted before surgery from ligament (LHBT, SGHL, MGHL, IGHL) stability to ligament-labrum anchor stability to labrum stability. This approach will guide clinical treatment decisions. The SLAP lesion is not only a superior labrum injury but also a biceps-SGHL-labrum complex injury. Our intention is not to propose the use of additional anchors, but rather to emphasize the importance of achieving precise reduction and fixations. In cases of SLAP lesions with SGHL detachment, the anchor should be placed in the appropriate position of the actual rupture, such as the 1-o’clock anchor position instead of the 12-o’clock position.
This classification of SLAP lesions described the integrity of the labrum ring and anterior instability, which is different from other classifications. In the Snyder classifications, 17 the injury only occurred in the labrum and was not associated with the integrity of the labrum and anterior instability. The existing type 7 SLAP tear through the capsule beneath is associated with labrum ring rupture, but Maffet et al 13 did not mention this. Type 6 SLAP tears with biceps tendon anchor release and SLAP tears with SGHL anchor release were not mentioned either. Therefore, we considered that these cases cannot be classified into Snyder classifications.
Our findings improved understanding of these series of injury patterns. The identification of a progressive nature from type A to type C suggests the importance of early detection and intervention. The SGHL labrum anchor was not stable and tore with the labrum, and the lesion was different from the former classification type 3. All 3 subtype injury ranges were between the LHBT anchor and SGHL anchor to varying degrees. Our findings also can guide decisions on whether to address the labral tear alone or in conjunction with ligament repair, which can affect the shoulder’s stability and overall function.
Limitations
There were some limitations to this study. First, the arthroscopic view of these cases was only from the standard posterior portal, and more views from different portals could help surgeons better understand the classification. Second, this study is a retrospective analysis, and the treatment and outcome for each subtype of SLAP lesion at different centers should be discussed.
Conclusion
Our study demonstrated a novel classification system for SLAP lesions associated with SGHL injury by introducing a series of cases with characteristics that showed high inter- and intraobserver reliability. Such cases have not been reported before, and the classification correlates with surgical treatment. The novel classification types can be used as a supplement to the traditional SLAP classification system and can help surgeons deeply understand the pathology and injury mechanism of SLAP lesions and guide clinical treatment.
Footnotes
Final revision submitted May 28, 2024; accepted June 4, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was received from the Capital’s Funds for Health Improvement and Research (2022-2-5051). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Chinese PLA General Hospital (S2021-19-01).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.