
Abstract
Background:
There are no statistical analyses on the association between the configuration of medial meniscus tears and the location of focal cartilage lesions.
Purpose:
To investigate the association between the configuration of medial meniscus tears and focal cartilage lesions and analyze whether the location of medial meniscus tears corresponds with that of focal cartilage lesions.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
The authors retrospectively evaluated the medical records of 317 patients with isolated medial meniscus tear who underwent arthroscopic surgery from January 2016 to December 2020. The configuration of the medial meniscus tear was determined based on the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS) classification. Patients with flap, radial, and longitudinal tears were included in the vertical tear group. For subgroup analysis, vertical tears were divided into medial meniscus posterior root tears and remaining tears. The location of the medial meniscus tear was categorized as anterior, middle, or posterior according to the ISAKOS classification. The cartilage of the medial femoral condyle (MFC) and that of the medial tibial condyle (MTC) were divided into 6 and 4 zones, respectively, and the location of cartilage lesions on the MFC and MTC was evaluated by preoperative magnetic resonance imaging.
Results:
There was a higher incidence of focal cartilage lesions with vertical versus horizontal medial meniscus tears (P < .001). For middle and posterior vertical tears with focal cartilage lesions, there was a significant concordance in location between the tear and the lesion (P < .001). In a subgroup analysis of medial meniscus posterior root tears, there was significantly more discordance in location between the tear and the lesion with medial meniscus posterior root tears (23/26 tears; 88.5%) compared with the remaining vertical tears (60/177 tears; 33.9%) (P < .001); instead, the focal cartilage lesions were mainly distributed in the lateral anterior and central portions of both the MFC and MTC.
Conclusion:
Vertical tears of the medial meniscus were significantly associated with the presence of focal cartilage lesions, whereas horizontal tears were not. Additionally, middle and posterior vertical tears with focal cartilage lesions showed significant concordance in location between the tear and the lesion.
The role of meniscal lesions in the pathogenesis of articular cartilage lesions remains unclear. Previous studies have shown that increasing the disruption of the circumferential meniscal fibers leads to an increase in contact pressure and is associated with cartilage degeneration of increasing severity in both the medial and lateral compartments of the knee. These studies evaluated the association between diffuse degenerative changes in cartilage and the configuration of meniscal tear.3,6,9,18,20
Christoforakis et al 2 reported that complex and horizontal cleavage meniscal tears were associated with a higher incidence and severity of cartilage degeneration than other types of meniscal tears. Furthermore, Lewandrowski et al 10 reported that longitudinal, bucket-handle, and complex tears of the medial meniscus were significantly associated with a higher incidence of articular cartilage damage than horizontal cleavage, flap, or radial tears. Conversely, several studies found no significant relationship between meniscal tears and cartilage degeneration.13-15 Controversy exists between the studies, and previous studies did not perform statistical analysis to determine which configuration of meniscal tear is associated with cartilage lesions; in addition, they only focused on the association between meniscal tear and diffuse cartilage degeneration.
In this study, we aimed to evaluate the relationship between the configuration of medial meniscus tears and the presence of focal cartilage lesions. We also aimed to analyze whether the location of medial meniscus tears was concordant with the location of focal cartilage lesions. We hypothesized that medial meniscus tears would be associated with the incidence of focal cartilage lesions and there would be a concordance in location between the medial meniscus tear and the focal cartilage lesion.
Methods
Study Population
The protocol for this study was approved by our internal institutional review board. We retrospectively reviewed the records of 378 consecutive patients who had been diagnosed with isolated medial meniscus tear based on history, physical examination, and magnetic resonance imaging (MRI) findings and were treated with arthroscopy between January 2016 and December 2020. All patients underwent arthroscopy because of knee pain or locking and failure of nonoperative treatment for the medial meniscus tear. The inclusion criteria were the presence of a single isolated medial meniscus tear, intact cruciate and collateral ligaments, no prior knee surgery, and no diffuse arthritic change on MRI. We excluded patients with diffuse cartilage lesions due to arthritic changes (n = 22), prior knee surgery (n = 33), and concomitant ligament injuries on the same knee (n = 12). However, 6 patients had previously undergone knee surgery specifically for ligament injuries, leading to an overlap between exclusion criteria. Consequently, 317 patients were included in the study.
Using coronal and sagittal T2-weighted MRI scans performed within 6 months preoperatively, we evaluated the locations of the medial meniscus tears and focal cartilage lesions in all included patients.
Medial Meniscus Tear Configuration and Location
The medial meniscus tears were all confirmed on arthroscopic evaluation at the time of treatment. All arthroscopies were performed by 3 surgeons (J.M.K., B.S.L., and S.I.B.) using a standard technique (ie, general anesthesia, tourniquet after exsanguination, approached via anterolateral and anteromedial portals), and the findings after each arthroscopy were recorded. During arthroscopic treatment, the 3 surgeons inspected both the medial and lateral compartments. Arthroscopic assessment on the configuration of the medial meniscus tear and grade of cartilage lesion was performed using arthroscopic images and videos.
The pattern of the medial meniscus tear was determined according to the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS) classification: radial, flap, longitudinal, or horizontal. 19 The overall configuration of the medial meniscus tear was classified based on the direction of the tear from the transverse plane of the medial meniscus: vertical or horizontal. Patients with flap, radial, and longitudinal tear patterns were included in the vertical tear group because these 3 patterns were caused by disruption of circumferential fibers of the medial meniscus; the remaining patients were included in the horizontal tear group. Within the vertical tear group, a subgroup of patients with posterior root tears was created. Posterior root tears were defined as radial tears situated within 1 cm from the meniscal attachment or a bony root avulsion. 16 In addition, the location of the medial meniscus tear was divided into anterior, middle, or posterior according to the ISAKOS classification (Figure 1).

Radial locations of the medial meniscus tear according to the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine classification. 19
Cartilage Lesion Grade and Location
During arthroscopy, articular cartilage lesions were evaluated using the International Cartilage Regeneration & Joint Preservation Society (ICRS) articular cartilage classification system. 1 On MRI and arthroscopy, single-zone cartilage lesions on both MFC and MTC, or single-zone cartilage lesions of a higher ICRS grade than surrounding lesions on both MFC and MTC, were defined as focal cartilage lesions. Cartilage lesions distributed in >4 zones were defined as diffuse cartilage lesions.
Using coronal and sagittal T2-weighted MRI scans performed within 6 months preoperatively, we evaluated the locations of the meniscal tears and focal cartilage lesions. The medial femoral condyle (MFC) cartilage was divided into 6 zones (F1, F2, F3, F4, F5, and F6), and the medial tibial condyle (MTC) cartilage was divided into 4 zones (T1, T2, T3, and T4) based on the surface in contact with the radial location of the meniscus (Figure 2).

Mapping of the articular cartilage in the medial femoral (F) condyle and medial tibial (T) condyle according to zones. Zones F1, F2, and T1 (anterior portion) defined concordant cartilage locations in the anterior part of the medial meniscus; zones F3 and T2 (middle portion) defined concordant cartilage locations in the middle part of medial meniscus; and zones F5, F6, and T4 (posterior portion) defined concordant cartilage locations in the posterior part of the medial meniscus.
Concordance in Location Between Focal Cartilage Lesions and Medial Meniscus Tears
Patients with focal cartilage lesions were classified into a concordant group or a discordant group based on whether there was a concordance in location between the medial meniscus tear and the focal cartilage lesion. Zones F1, F2, and T1 were defined as concordant cartilage locations in the anterior part of the medial meniscus. Zones F3 and T2 were defined as concordant cartilage locations in the middle part of the medial meniscus. Zones F5, F6, and T4 were defined as concordant cartilage locations in the posterior part of the medial meniscus. Zones F6 and T4 were defined as concordant cartilage locations in the posterior root of the medial meniscus (Figure 2).
Statistical Analysis
The Mann-Whitney U test was used to examine the differences in patient factors between the vertical and horizontal tear groups, and the chi-square test was used to compare the incidence of focal cartilage lesions between the groups. For further analysis of the concordance in location between medial meniscus tears and focal cartilage lesions, the locations of the tears and lesions were stratified into middle versus nonmiddle as well as posterior versus nonposterior portions of the MFC and MTC (Figure 3). The concordance in location between tears and lesions found in the middle and nonmiddle and the posterior and nonposterior portions was evaluated using chi-square analysis. Statistical significance was set at P < .05. SPSS for Windows (Version 26.0; IBM Corp) was used for the statistical analyses.

The locations of the medial meniscus tears and focal cartilage lesions were stratified into (A) middle (zones F3 and T2) versus (B) nonmiddle (zones F1, F2, F4-F6, T1, T3, and T4) portions and (C) posterior (zones F5, F6, and T4) versus (D) nonposterior (zones F1-F4 and T1-T3) portions of the medial femoral condyle and medial tibial condyle.
Results
Of the 317 study patients, there were 260 patients with vertical medial meniscus tears, and 57 patients with horizontal medial meniscus tears. The mean ages of the vertical and horizontal tear groups were 58.2 and 52.0 years, respectively, with the vertical tear group being significantly older than the horizontal tear group (P < .05). There were no other significant differences in patient characteristics between these groups (Table 1).
Characteristics of the Patient Population According to Medial Meniscus Tear Configuration (N = 317 Patients/Tears) a
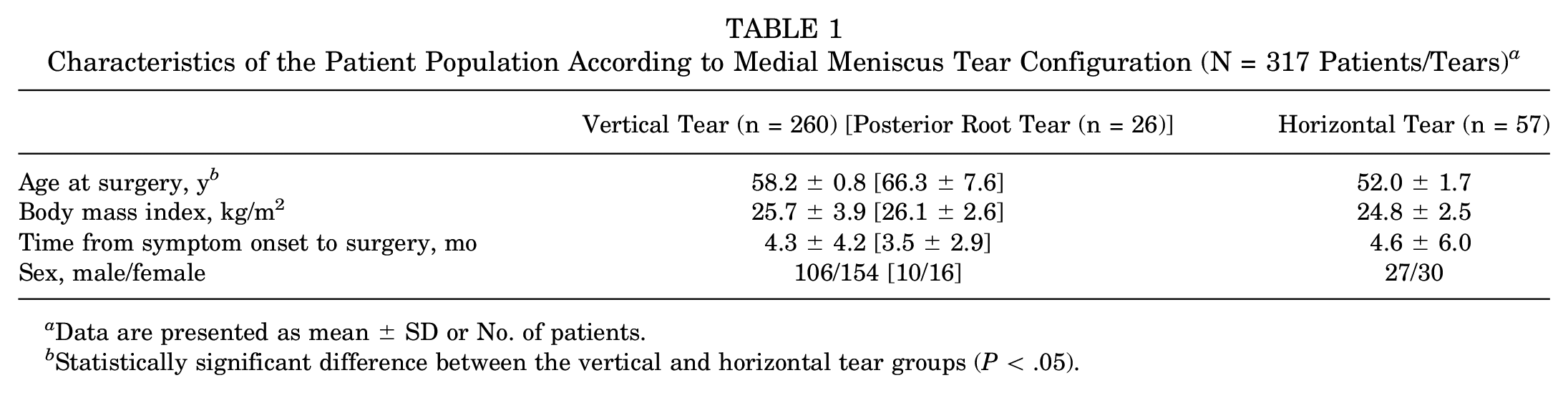
Data are presented as mean ± SD or No. of patients.
Statistically significant difference between the vertical and horizontal tear groups (P < .05).
Presence of Focal Cartilage Lesion According to Tear Configuration
Of the 260 patients with vertical tears, 203 patients (78.1%) had cartilage lesions, and of the 57 patients with a horizontal tear, 12 patients (21.1%) had cartilage lesions. The ICRS grade of the cartilage lesions stratified by meniscal tear pattern is listed in Table 2. The incidence of cartilage lesion was significantly higher in patients with vertical tears than in those with horizontal tears (P < .001; OR, 13.36) (Table 3).
ICRS Grade of Focal Cartilage Lesions According to Medial Meniscus Tear Pattern (n = 215 Lesions) a

Data are presented as No. of lesions.
Incidence of Focal Cartilage Lesions According to Medial Meniscus Tear Configuration (N = 317 Tears) a
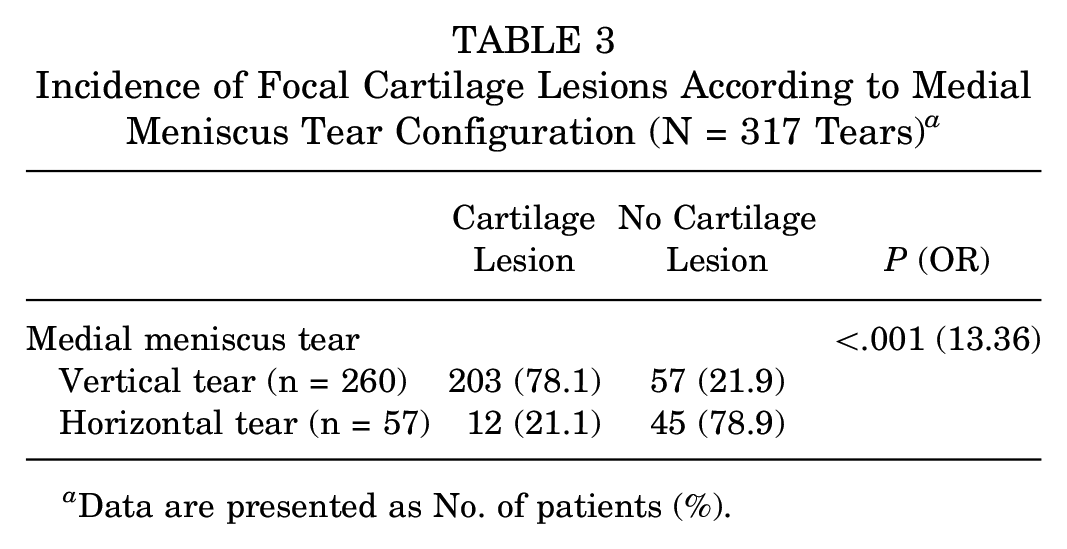
Data are presented as No. of patients (%).
Concordance in Location Between Focal Cartilage Lesions and Medial Meniscus Tears
In all 12 patients with horizontal tears and focal cartilage lesions, the cartilage lesions were located posteriorly, and 11 of the 12 patients (91.7%) had discordant cartilage lesions. Most of the discordant cartilage lesions were in the F4 and T3 zones. Of the 203 patients with vertical tears and focal cartilage lesions, 80 patients had vertical tears in the middle and 121 patients had vertical tears in the posterior portions. Of the 80 patients with vertical tears in the middle, 51 (63.8%) had concordant cartilage lesions. Of the 121 patients with posterior vertical tears, 69 (57.0%) had concordant cartilage lesions (Table 4).
Concordance Between Vertical Tears and Focal Cartilage Lesions (n = 203) a

Data are presented as No. of patients (%).
Concordant group: patients with vertical tears and concordance in location between the medial meniscus tear and focal cartilage lesion.
Discordant group: patients with vertical tears and no concordance in location between the medial meniscus tear and focal cartilage lesion.
In the comparative analysis according to tear/lesion location in the MFC and MTC, there was a significant concordance in location between cartilage lesions in the middle portion and middle vertical tears versus cartilage lesions in the middle portion and nonmiddle vertical tears (P < .001; OR, 41.43). Likewise, there was significant concordance between cartilage lesions in the posterior portion and posterior vertical tears versus cartilage lesions in the posterior portion and nonposterior vertical tears (P < .001; OR, 157.26) (Table 5).
Concordance of Vertical Tears and Focal Cartilage Lesions According to the Middle and Posterior Portions of the MFC and MTC (n = 203) a
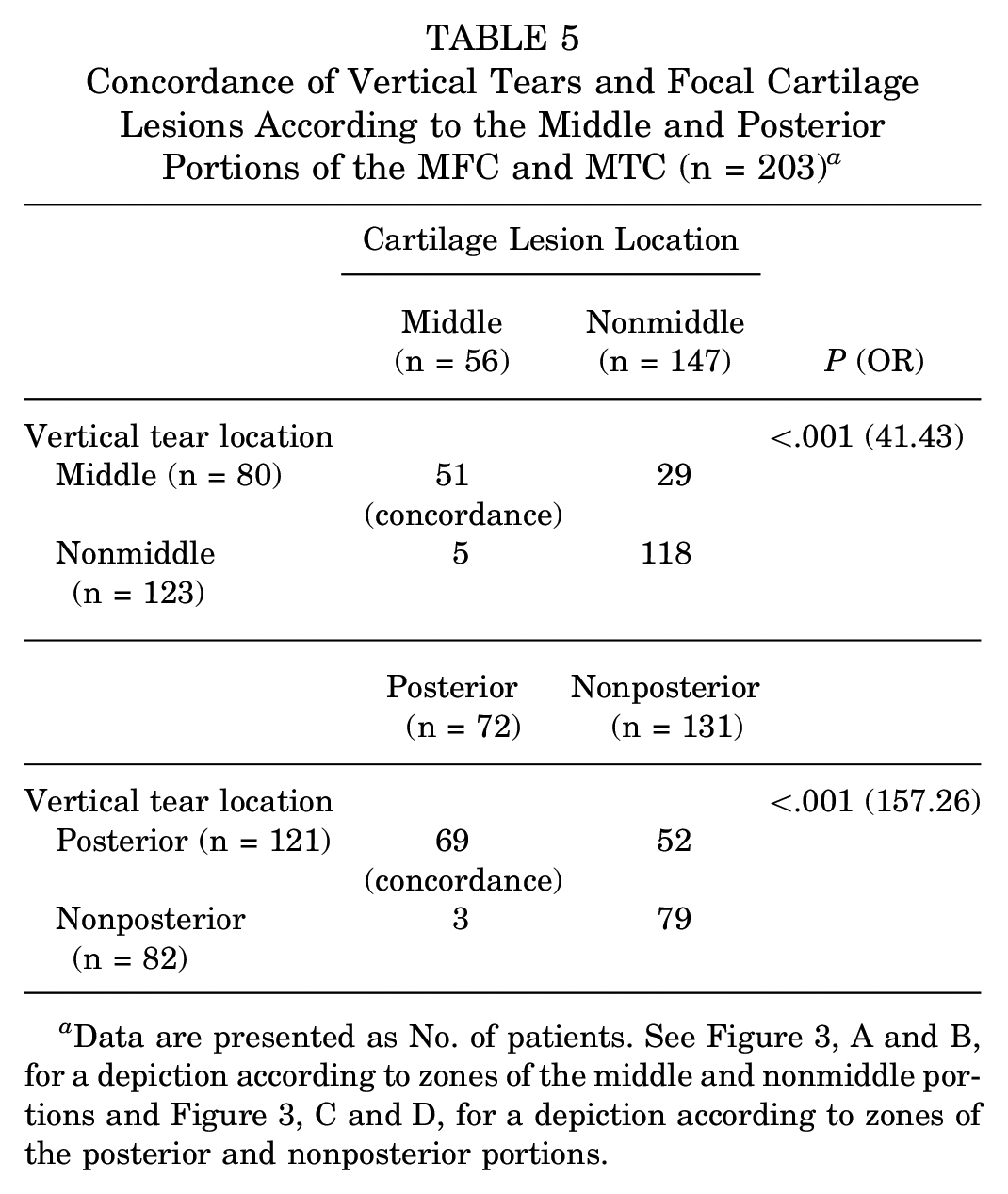
Data are presented as No. of patients. See Figure 3, A and B, for a depiction according to zones of the middle and nonmiddle portions and Figure 3, C and D, for a depiction according to zones of the posterior and nonposterior portions.
Distribution of Focal Cartilage Lesions in Medial Meniscus Posterior Root Tears
When comparing medial meniscus posterior root tears with the other vertical tears, there was significantly more discordance between the tear and lesion with medial meniscus posterior root tears (23/26 tears; 88.5%) than with the remaining vertical tears (60/177 tears; 33.9%) (P < .001) (Table 6). Instead, the focal cartilage lesions associated with medial meniscus posterior root tears were mainly distributed in the lateral anterior and central portions of both the MFC and MTC (Figure 4).
Comparison of Concordance Between Medial Meniscus Posterior Root Tears and Other Vertical Tears (n = 203) a

Data are presented as No. of patients (%).

Distribution of cartilage lesions associated with medial meniscus posterior root tears in the (A) medial femoral condyle and (B) medial tibial condyle.
Discussion
The most important finding of this study was that there was a significant association between vertical tears of the medial meniscus and focal cartilage lesions. Vertical tears had a significantly higher incidence of focal cartilage lesions than horizontal tears (P < .001; OR, 13.36). In addition, there was significant concordance in location between vertical tears and adjacent focal cartilage lesions (middle vs nonmiddle MFC/MTC: P < .001 [OR, 41.43]; posterior vs nonposterior MFC/MTC: P < .001 [OR, 157.26]).
A meniscal tear is a strong risk factor for developing osteoarthritis. 4 Therefore, it is important to better understand the association between meniscal tears and cartilage lesions in order to establish an appropriate treatment plan to prevent osteoarthritis. The few studies that have analyzed the association between meniscal tears and cartilage lesions have shown conflicting results. Christoforakis et al 2 evaluated cartilage lesions during arthroscopic treatment of 497 meniscal tears and reported that complex and horizontal cleavage meniscal tears were associated with a higher incidence of degenerative cartilage lesions than other types of meniscal tears. Lewandrowski et al 10 reported that longitudinal, bucket-handle, and complex tears of the medial meniscus were associated with higher rates of articular cartilage damage than horizontal cleavage, flap, or radial tears. Conversely, Henry et al 5 prospectively evaluated 103 patients diagnosed with isolated medial meniscus tears and reported that radial and flap tears were associated with degeneration of the MFC and that root and complex tears were associated with degeneration of the medial tibial plateau. These authors 5 did not evaluate which medial meniscus tear type was associated with cartilage lesions, nor did they statistically analyze the association between the location of meniscal tears and that of focal cartilage lesions.
Our study showed that the incidence of focal cartilage lesions was significantly higher in vertical tears than in horizontal tears. Studies on biomechanical changes after meniscal tear have reported that radial, flap, and longitudinal meniscal tears lead to increased shear stress and redistribution of stress on both femoral and tibial condyles. Biomechanically, these previous findings explain the higher incidence of focal cartilage lesions in vertical tears.7,11,12,21,22
In our analysis of the concordance in location between medial meniscus tears and focal cartilage lesions, we found that when vertical tears occurred in the middle or posterior portion of the medial meniscus with focal cartilage lesions, there was significant concordance between the location of the focal cartilage lesions on both the MFC and MTC and that of medial meniscus tears. Our findings provide an improved understanding of the association between medial meniscus tears and adjacent focal cartilage lesions before the development of osteoarthritis.
In a previous study, root tears caused total compromise of the ability of the meniscus to generate hoop stress and alter transitional and rotational knee biomechanics, possibly leading to increased loading of the MFC and MTC. 7 Because there is less coverage of the meniscus on the medial aspect of both the MFC and MTC, the cartilage lesion may occur more medially in posterior root tears of the medial meniscus.8,17 For these reasons, we predicted that the location of focal cartilage lesions in medial meniscus posterior root tears would be different from that of other vertical tears. In our subgroup analysis, there was no significant concordance in location between medial meniscus posterior root tears and focal cartilage lesions, and the focal cartilage lesions of medial meniscus posterior root tears were mainly distributed in the lateral anterior and central portions of both the MFC and MTC.
Limitations
This study has several limitations. First, this study has a retrospective design. Second, we focused only on the medial meniscus and did not evaluate the lateral meniscus. Third, owing to the small sample size, we could not conduct a subgroup analysis according to tear configuration in our evaluation of the concordance in location between tears and lesions. Fourth, evaluating medial meniscus tears and focal cartilage lesions at a single time point limits our conclusions; whether the cartilage lesions are due to medial meniscus tears remains unclear. Further studies on whether there is a causal relationship between focal cartilage lesions and medial meniscus tears is required.
Conclusion
In this study, vertical tears were significantly associated with the incidence of focal cartilage lesions, whereas horizontal tears were not. In addition, there was significant concordance in location between vertical tears and focal cartilage lesions. However, significantly more discordance in location between tear and lesion was found in medial meniscus posterior root tears than in the remaining vertical tears.
Footnotes
Final revision submitted April 28, 2024; accepted June 11, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Asan Medical Center (reference No. 2022-1458).