
Abstract
Background:
Numerous single- and double-row repair techniques with simple and modified stitches have been described for subscapularis tendon tears.
Purpose/Hypothesis:
This study aimed to uniformly evaluate the influence of 4 different repair techniques on the biomechanical performance of fixation for full-thickness subscapularis tendon tears. It was hypothesized that (1) the 2 modified single-row repair techniques would require more cycles to result in 3- and 5-mm gap formation and have a higher load to failure after cyclic loading than the simple single-row repair technique and (2) the double-row repair technique would also require more cycles to result in 3- and 5-mm gap formation and have a significantly higher load to failure after cyclic loading compared to the simple single-row repair technique.
Study Design:
Controlled laboratory study.
Methods:
Full-thickness subscapularis tendon tears were created in 32 fresh-frozen cadaveric shoulders, and the tears were treated in 1 of 4 ways: (1) single-row repair with the mattress stitch, (2) single-row repair with the modified lasso-loop stitch, (3) single-row repair with the modified Mason-Allen stitch, or (4) double-row repair. After repair, specimens were progressively cyclically loaded to 200 N, and the number of cycles to obtain a 3- and 5-mm gap was recorded. After cyclic loading, the specimens were loaded to failure at 500 mm/min, and ultimate failure loads were measured.
Results:
There were no significant differences between either of the modified single-row repair techniques and the simple single-row repair technique. Double-row repair withstood significantly more cycles until 3-mm (P < .001) and 5-mm (P = .004) gap formation and had a higher ultimate failure load (P = .015) compared to the simple single-row repair technique, and double-row repair withstood more cycles until 3-mm gap formation (P = .003) compared with single-row repair with the modified lasso-loop stitch. No significant differences were found between double-row repair and single-row repair with the modified Mason-Allen stitch.
Conclusion:
Findings indicated that (1) there was no significant biomechanical advantage of the modified single-row repair techniques over the simple single-row repair technique and (2) while the double-row repair technique was biomechanically superior to the simple single-row repair technique, there was no significant difference between single-row repair with the modified Mason-Allen stitch and double-row repair.
Clinical Relevance:
Considering that double-row repair might not be useful in some tears because of the risk of overtensioning, modified single-row repair techniques appear to be an adequate refixation alternative.
Keywords
The subscapularis muscle represents the only anterior component of the rotator cuff and therefore is an important dynamic anterior stabilizer and internal rotator at the glenohumeral joint, establishing anterior-posterior equilibrium as part of the transverse force couple of the rotator cuff (subscapularis vs infraspinatus and teres minor muscle).4,13,28 Consequently, tears of the subscapularis tendon can induce significant functional impairments, and thus, surgical repair is indicated in the majority of cases. 31 Nevertheless, their frequency has long been underestimated, as they are difficult to diagnose. 16 With improved arthroscopic techniques and high-resolution magnetic resonance imaging, a higher prevalence of subscapularis tendon tears has been demonstrated in recent years (eg, 37%-69% in arthroscopic rotator cuff repair), thus revealing their true significance, although they have mostly occurred as partial ruptures involving the upper portion of the subscapularis only.1,6
Analogous to improvements in diagnostic methods, minimally invasive arthroscopic techniques for rotator cuff repair have considerably evolved through the development of suture anchor systems with high pull-out strength and improved arthroscopic instruments over the years, leading to results comparable with those of open surgical repair.2,21 In addition to biological conditions (eg, bone and tendon quality), outcomes significantly rely on biomechanical and technical reconstruction factors such as the suture anchor design, its insertion angle and positioning, thread number and thickness, and particularly suture technique and configuration.5,11 Regarding the latter, numerous reconstruction techniques including simple and modified single- and double-row repair techniques have been described for arthroscopic rotator cuff repair.15,18,22,29 Few studies have been performed to individually compare subscapularis tendon repair for full-thickness subscapularis tendon tears.32,33,36 Sufficient biomechanical evidence for an unequivocal recommendation is lacking because of the limited number of studies and the varying study designs. 34
Considering the central biomechanical importance of the subscapularis regarding shoulder function and stability, we aimed to uniformly evaluate the influence of multiple different repair techniques on the biomechanical performance of arthroscopic repair for complete subscapularis tendon tears. 28 Taking into account that double-row repair techniques might not be available in retracted tears because of insufficient arthroscopic exposure of the lateral-caudal portion of the tendon or might not be useful because of the risk of overtensioning, modified single-row repair techniques (the modified Mason-Allen stitch by Scheibel and Habermeyer 29 and the modified lasso-loop stitch by Lafosse et al 15 ) were included in addition to single- and double-row repair techniques with simple stitches.14,15,26,29 It was hypothesized that (1) the modified single-row repair techniques would require more cycles to result in 3- and 5-mm gap formation and have higher loads to failure than the simple single-row repair technique and (2) the double-row repair technique would also require more cycles to result in 3- and 5-mm gap formation and have a higher load to failure compared to the simple single-row repair technique.
Methods
Specimen Collection
After receiving institutional review board approval for the study protocol, 32 fresh-frozen upper extremity specimens were obtained from Science Care. There were 15 male and 17 female specimens, the mean age of the donors was 79 ± 13 years (range, 52-95 years), and 27 of the specimens were left-sided extremities, while 5 of them were right-sided extremities. The mean bone mineral density of the humeral head as measured with dual-energy X-ray absorptiometry was 0.57 ± 0.16 g/cm2. The specimens were stored at −20°C and were thawed at room temperature 24 hours before dissection and biomechanical testing. Fluoroscopic and clinical examinations were performed to exclude specimens with restricted range of motion as a result of osteoarthritis or previous surgery and trauma to the shoulder. None of the 32 specimens had to be excluded. The specimens were kept moist during biomechanical testing by irrigation with 0.9% saline solution.
Specimen Dissection
Dissection of the specimens was performed as previously published.8,10 Transection of the proximal humerus was performed 10 cm distal to the most lateral aspect of the greater tuberosity. Soft tissue around the shoulder was carefully removed, leaving the rotator cuff and the long head of the biceps tendon intact. The rotator cuff muscles were then dissected off the scapula from medial to lateral until exposure of the glenohumeral capsule was achieved. Circumferential transection of the capsule and the long head of the biceps tendon at its origin at the superior labrum was then performed to dislocate the glenohumeral joint and to remove the scapula. The supraspinatus, the infraspinatus, and the teres minor were removed, leaving only the subscapularis intact. None of the specimens showed relevant rotator cuff tears after a thorough inspection of the bursal and articular sides. After verification of a normal insertion, the subscapularis tendon was sharply dissected off the lesser tuberosity. The horizontal and vertical dimensions of the footprint of the subscapularis were measured using a digital caliper, and the footprint area was subsequently calculated (in mm2). The thickness of the rolled upper border of the subscapularis tendon was measured with the same caliper 1 cm medial to the tendon insertion.
Repair Techniques
The specimens were randomly organized according to age, sex, side, weight, bone mineral density, footprint area, and tendon thickness into 1 of 4 groups: single-row repair with the mattress stitch 8 (SR group), single-row repair with the modified lasso-loop stitch 15 (LL group), single-row repair with the modified Mason-Allen stitch 29 (MA group), or double-row repair with the simple stitch (DR group). In each of the 4 groups, the respective specimens underwent 1 of the 4 repair techniques in a standardized fashion as described below. All repair procedures were performed by the same surgeon (M.H.) with the adducted shoulder in neutral rotation in a simulated beach-chair position. All knots were tied using a double-sliding half-hitch knot, followed by alternating half-hitches for a total of 5 throws.
Single-Row Repair With Mattress Stitch
There were 2 single-loaded, 4.75-mm BioComposite SwiveLock suture anchors (Arthrex) placed at the lesser tuberosity according to the manufacturer's recommendations. The first anchor was placed 10 mm medial to the bicipital groove at the upper border of the subscapularis footprint. The second anchor was placed 15 mm distal to the first one. A vertical mattress stitch in line with the longitudinal axis of the humerus was used with both anchors. The respective No. 2 FiberWire (Arthrex) limbs of each anchor were placed through the tendon 5 mm apart from each other using the Scorpion suture passer (Arthrex), and the sutures were subsequently tied and cut (Figure 1A).

Repair techniques. The left and middle columns show images of tendon threading, and the right column shows images of completed repair. (A) Single-row repair with mattress stitch, (B) single-row repair with modified lasso-loop stitch, (C) single-row repair with modified Mason-Allen stitch, and (D) double-row repair.
Single-Row Repair With Modified Lasso-Loop Stitch
There were 2 single-loaded, 4.75-mm suture anchors placed at the lesser tuberosity according to the manufacturer's recommendations as stated above. Analogously, the paired sutures of the suture anchors were each positioned under the subscapularis tendon and passed through the tendon 5 mm apart from each other with the suture passer. While the inferior limbs of each suture anchor were simply passed through tissue, the superior limbs were not completely pulled through the tendon, forming a loop at the upper tendon surface, and were then each passed from posterior through the corresponding loops. After pulling on the ends one by one, the suture was secured by half-stitch locking knots (Figure 1B).
Single-Row Repair With Modified Mason-Allen Stitch
There were 2 double-loaded, 4.75-mm suture anchors placed at the lesser tuberosity according to the manufacturer's recommendations as stated above. Combined vertical and horizontal stitches were used for both anchors, starting with the vertical mattress stitch in line with the longitudinal axis of the humerus. The pairwise color-coded sutures of each anchor were placed through the tendon 10 mm vertically apart to each other using the aforementioned suture passer. Before knotting the sutures to secure the vertical mattress stitch, the other color-coded suture pairs of the anchors were placed through the tendon horizontally between the previous sutures using the suture passer. The vertical mattress stitch was knotted first, followed by the horizontal mattress stitch, which was locked on top of it (Figure 1C).
Double-Row Repair With Simple Stitch
There were 4 single-loaded, 4.75-mm suture anchors placed at the lesser tuberosity according to the manufacturer's recommendations. The first anchor of the lateral row was placed medial to the lateral border of the bicipital groove. The second anchor of the lateral row was introduced 12 mm distal. The 2 anchors of the medial row were placed 12 mm medial to the lateral row next to the articular surface. A vertical mattress stitch was used with the medial-row suture anchors as described above, whereas a simple stitch was used for the lateral-row suture anchors (Figure 1D).
Biomechanical Testing
Biomechanical testing was performed with a servohydraulic testing machine (Model Z010; Zwick Roell) as previously published.8,10 The proximal humerus was mounted horizontally onto the testing machine with a custom-made testing rig with the lesser tuberosity facing anterior (Figure 3B). Medical gauze was wrapped around the muscle belly of the subscapularis and tightly secured with suture material before an adjustable interdigitating custom-made metal clamp was firmly affixed to it 3 cm proximal to the medial border of the tendon. The clamp was then attached to the mobile traverse of the testing machine. Thus, upward movements of the mobile traverse of the testing machine resulted in a physiological pulling force on the subscapularis tendon.
After pretensioning of the repaired tendon with 5 N for 1 minute, cyclic loading at a speed of 350 mm/min and a frequency of 0.5 Hz was performed according to a previously published protocol. 27 The specimens were first loaded between the minimum load of 5 N and the maximum load of 60 N for 50 cycles. Then, the maximum load was incrementally increased by 20 N for every 50 cycles until 200 N was reached (ie, 50 cycles each for 5-80 N, 5-100 N, 5-120 N, 5-140 N, 5-160 N, 5-180 N, and 5-200 N) (Figure 2). If the specimens did not fail during cyclic loading, they were loaded to failure at a speed of 500 mm/min. The number of cycles until displacement of 3 mm and 5 mm was evaluated as well as the number of cycles until ultimate failure of the repair construct occurred. The ultimate failure load was also recorded.

Test setup. DR, double-row repair; LL, single-row repair with modified lasso-loop stitch; MA, single-row repair with modified Mason-Allen stitch; SR, single-row repair with mattress stitch.
Optical Measurement of Displacement
A high-resolution 3-dimensional camera system consisting of 2 monochrome digital cameras (Q400-3D; LIMESS Messtechnik and Software) recorded the subscapularis tendon during cyclic loading of the specimens as previously published (Figure 3, A and B).8,10 Gap formation at the tendon-bone interface was analyzed through digital image correlation with the use of Istra4D software (Dantec Dynamics) (Figure 3C). Digital image correlation relies on a speckle pattern on the surface of the specimen being examined. Therefore, the tendon-bone interface was first homogeneously covered with matte white paint, and subsequently, small spray spots of matte black paint were randomly applied. Small subsets of these speckle patterns were chosen in their initial position and followed during videographic recording of the motion. The change in the position of 2 center points of a subset to each other during loading was analyzed precisely to calculate their displacement in space and time (accuracy: 0.01 pixels; resolution: 2452 × 2052 pixels). The spatial displacement of points on the curved surface of the bone was captured by 2 cameras looking from different angles.9,35 The number of cycles that occurred until the formation of a 3- and 5-mm gap at the tendon-bone interface was recorded.

Data analysis. (A) A 3-dimensional camera system, (B) the subscapularis tendon with a speckle pattern on the surface being examined during cyclic loading, and (C) analysis through digital image correlation.
Statistical Analysis
Means, standard deviations, and ranges were calculated for all biomechanical parameters. The Shapiro-Wilk test was applied to ensure a normal distribution of the data. One-way analysis of variance with the post hoc Bonferroni test was performed to assess significant differences between the 4 repair techniques regarding age, weight, bone mineral density, footprint area, and tendon thickness as well as to evaluate significant differences in gap formation and ultimate failure load, while the chi-square test was used to determine differences regarding sex and side. The significance level was set at P < .05. Statistical analysis was performed using SSPS Statistics software (Version 25.0.0.0; IBM).
With 32 specimens and an effect size f = 0.33 (η2 = 0.097; α = 0.05), the study had 98.2% power to detect any difference in the 3 outcome variables (number of cycles until 3- and 5-mm gap formation, ultimate failure load) between the 4 repair groups (G*Power; Version 3.1.9.4).
Results
No significant differences between the groups were observed regarding sample size, age, sex, side, weight, bone mineral density, footprint area, and tendon thickness (Table 1).
Specimen Characteristics (n = 32) a

Data are presented as mean ± SD unless otherwise indicated. DR, double-row repair; LL, single-row repair with modified lasso-loop stitch; MA, single-row repair with modified Mason-Allen stitch; SR, single-row repair with mattress stitch.
The number of cycles until the formation of a 3-mm gap at the tendon-bone interface occurred was 182 ± 42 (range, 119-240) for the SR group, 203 ± 34 (range, 166-255) for the LL group, 227 ± 39 (range, 181-272) for the MA group, and 278 ± 37 (range, 212-323) for the DR group. The DR group withstood significantly more cycles than the SR group (P < .001) and the LL group (P = .003) but not compared to the MA group (P = .073). No other significant differences were found regarding the number of cycles until 3-mm gap formation between the 4 groups (P≥ .159).
The number of cycles until 5-mm gap formation at the tendon-bone interface occurred was 232 ± 59 (range, 144-288) for the SR group, 265 ± 47 (range, 212-328) for the LL group, 289 ± 51 (range, 221-328) for the MA group, and 329 ± 41 (range, 277-381) for the DR group. Once again, significantly more stability was seen in the DR group than in the SR group (P = .004). No other significant differences were found regarding the number of cycles until 5-mm gap formation between the 4 groups (P≥ .103).
Overall, 2 specimens in the SR group and 1 specimen in LL group failed during cyclic loading. The ultimate load to failure was 256 ± 75 N (range, 140-354 N) for the SR group, 293 ± 66 N (range, 160-388 N) for the LL group, 340 ± 49 N (range, 252-404 N) for the MA group, and 361 ± 59 N (range, 267-411 N) for the DR group. Again, a significantly higher ultimate failure load was seen in the DR group than in the SR group (P = .015). No other statistically significant differences were observed with regard to ultimate failure load (P≥ .078). The results for cyclic loading and ultimate failure load are outlined in Figure 4.
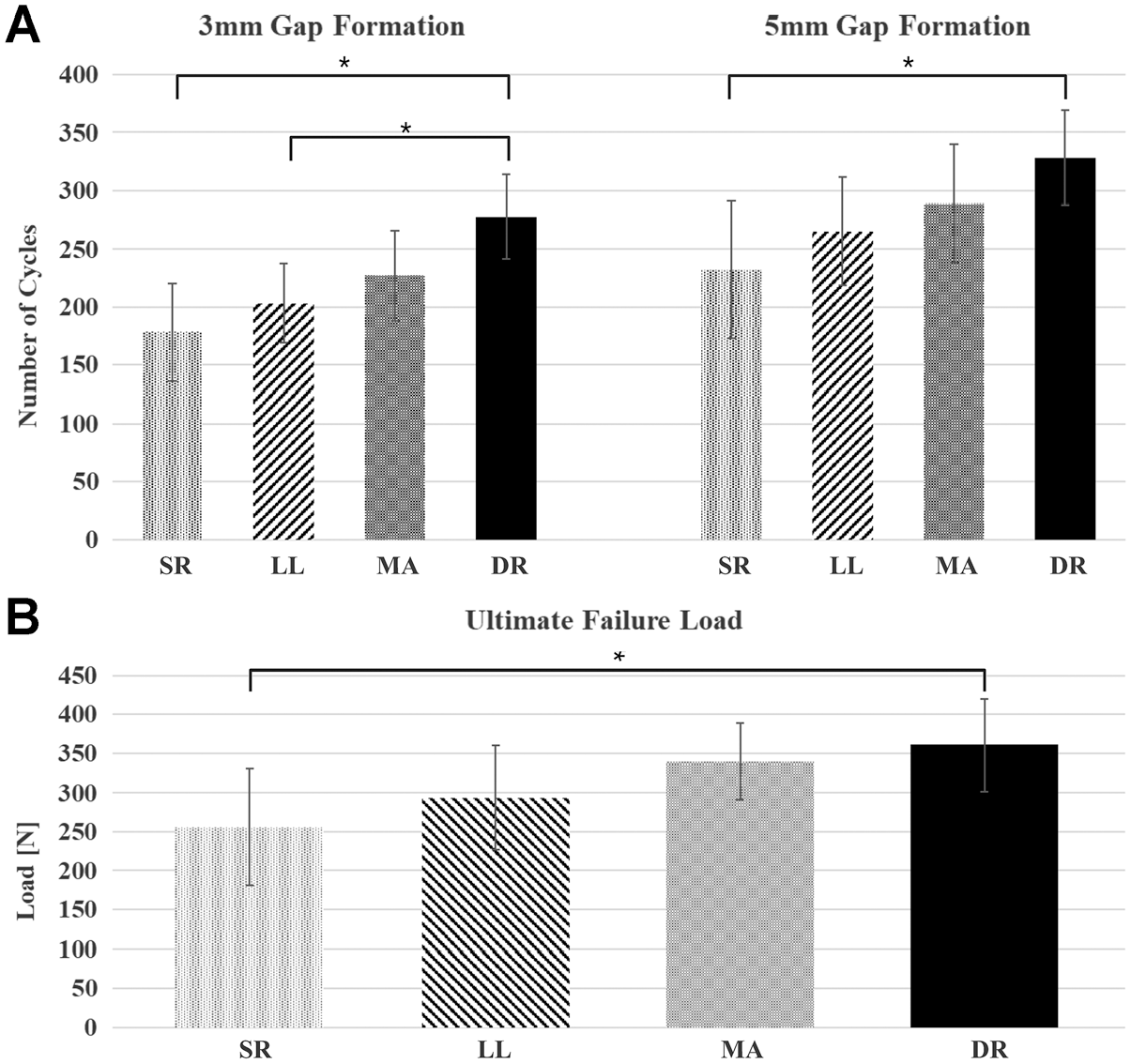
Results for (A) cyclic loading and (B) ultimate failure load. *Significant differences between groups (P < .05). DR, double-row repair; LL, single-row repair with modified lasso-loop stitch; MA, single-row repair with modified Mason-Allen stitch; SR, single-row repair with mattress stitch.
Discussion
This investigation showed that the simple single-row repair technique required a significantly lower number of cycles until 3- and 5-mm gap formation, and had a lower ultimate failure load, while single-row repair with the modified lasso-loop stitch required a significantly lower number of cycles until 3-mm gap formation compared to double-row repair. Overall, the double-row repair technique demonstrated the highest number of cycles to 3- and 5-mm gap formation and the greatest ultimate load to failure. Our first hypothesis, that the modified single-row repair techniques would be biomechanically superior to the simple single-row repair technique, was not confirmed. However, our second hypothesis, that the double-row repair technique would be biomechanically superior to the simple single-row repair technique, was validated. Additionally, specimens treated with single-row repair with the modified Mason-Allen stitch showed no significant differences on any examined biomechanical parameter compared to those treated with double-row repair.
While previous biomechanical studies have shown that a single suture anchor is sufficient for tears of the subscapularis tendon that involve only the upper third, 2 suture anchors are typically used in the configuration of single-row repair and 4 in cases of double-row repair for complete full-thickness subscapularis tendon tears.3,20,32 Also, a retrospective analysis of clinical cases after arthroscopic single-row repair of the subscapularis showed that 1 to 2 suture anchors were used according to the extent of the subscapularis tendon tear. 30 As complete full-thickness tears were induced in the present study, 2 suture anchors were applied for the single-row repair techniques.
Prior studies comparing single- and double-row repair techniques on human cadaveric supraspinatus tendons 7 and sheep infraspinatus tendons 12 led to the conclusion that an increased number of sutures through tissue provided improved biomechanical performance. A study specifically comparing the clinical outcomes and repair integrity of arthroscopic single- versus double-loaded single-row labral repair for chronic anterior shoulder instability showed no significant difference in the retear rate in both groups, but the number of suture anchors in the single-loaded single-row repair group was slightly higher (4 vs 3, respectively). 17 In the present study, single-loaded suture anchors were used for single-row repair with the modified lasso-loop stitch, while double-loaded anchors were applied for single-row repair with the modified Mason-Allen stitch, which withstood the highest number of cycles to 3- and 5-mm gap formation and had the greatest load to failure of the 3 single-row repair techniques assessed. The higher number of sutures passed through tissue might have contributed to these results.
Previous comparative clinical and biomechanical studies regarding single- and double-row repair techniques for full-thickness subscapularis tendon tears have shown inconsistent results.32,33,36 Wellmann et al 32 reported in their biomechanical study that double-row repair was stronger and stiffer compared to single-row repair with the modified Mason-Allen stitch for full-thickness subscapularis tendon tears. In contrast, the results of this investigation showed that there was no significant difference in biomechanical performance between double-row repair and single-row repair with the modified Mason-Allen stitch, with the latter being easier to perform, being less time consuming, requiring less soft tissue dissection and suture anchors, and therefore likely involving significant cost savings compared to double-row repair.18,23,34 While a conventional double-row repair technique with simple and mattress stitches was performed in the present study, Wellmann et al 32 used a double-row suture-bridge repair technique with the modified Mason-Allen stitch for the medial-row suture anchors.
Corresponding comparative studies have demonstrated the biomechanical superiority of the suture-bridge repair technique as opposed to the double-row repair technique with simple and mattress stitches for supraspinatus tendon tears.24,25 No respective biomechanical studies are available for subscapularis tendon tears. However, a comparative clinical study on 56 patients with subscapularis tendon tears by Yoon et al 36 showed no significant differences between arthroscopic single- and double-row repair in terms of structural integrity and clinical outcomes at 2-year follow-up, although a suture-bridge repair technique was used. As single-row repair with the modified Mason-Allen stitch demonstrated a higher mean ultimate failure load than single-row repair with the mattress stitch in the present study, one could assume that double-row suture-bridge repair with the modified Mason-Allen stitch for the medial-row suture anchors might offer even higher biomechanical stability compared to the conventional suture-bridge repair method. 34 However, a biomechanical comparison by Wheeler et al 33 performed on full-thickness subscapularis tendon tears found no differences between transosseous repair with 3 modified Mason-Allen stitches and repair with 4 mattress stitches for 2 double-loaded suture anchors.
Considering only the repair techniques examined in the present study, a biomechanical study on supraspinatus tendon tears by Nelson et al 23 in which single-row repair with the modified Mason-Allen stitch was compared to conventional double-row repair with single and mattress stitches also found no statistically significant difference with regard to biomechanical strength. Similar results were shown in a biomechanical study on multiple repair techniques for infraspinatus tendon tears by Lorbach et al, 19 also coming to the conclusion that modified stitches might provide improved relative and absolute stability over simple stitches. While they found higher stability with single-row repair with the modified Mason-Allen stitch compared to the simple single-row repair technique, it showed no biomechanical superiority over double-row repair. 19 Both modified single-row and conventional double-row repair techniques with maximum failure loads around 400 N did not achieve mean ultimate failure loads of approximately 750 N in intact subscapularis tendons. 32
Regarding single-row repair with the modified lasso-loop stitch, data from comparative studies concerning the subscapularis were available for only upper-third tendon repair with 1 suture anchor. 3 The biomechanical study by Borbas et al 3 similarly showed higher mean stiffness and ultimate loads to failure in the knotted lasso-loop mattress group compared to the knotted mattress group, but the difference was not statistically significant. The knotted lasso-loop mattress technique was superior to the knotted horizontal mattress technique only in regard to pressurized footprint coverage. 3
Although not unequivocally comparable, the findings of the current investigation appear to be largely consistent with earlier study results for rotator cuff refixation techniques, showing that a modified single-row repair technique (ie, single-row repair with the modified Mason-Allen stitch) was comparable to the conventional double-row repair technique.
Limitations
It is important to point out that the present study is limited by the fact that the number of sutures through tissue varied by the single-row repair technique used and only single-row repair with the modified Mason-Allen stitch was performed with double-loaded suture anchors. This study is also limited by the fact that only one conventional double-row repair technique was included. However, the main aim of the study was to evaluate the biomechanical properties of different single-row repair techniques, as arthroscopic double-row repair of the subscapularis is less common, is more time consuming, and requires more soft tissue dissection. Moreover, a basic limitation consists of the in vitro study design inherent to all biomechanical cadaveric studies. While ultimate failure load was defined as the maximum strength before anchor pullout and/or suture knot failure, the mode and site of failure were not specifically documented for each specimen and therefore not included in the evaluation. Furthermore, a limited number of 8 specimens per group, resulting in a total sample size of 32 specimens, was available for this investigation, which however is slightly higher than in comparable biomechanical studies.3,23,32,33
Another limitation consists of the rather elevated mean age of the donors (mean age at the time of death, 79 years) compared to the typical age of patients undergoing surgical rotator cuff repair. However, no subscapularis tendon tears were observed during specimen preparation and dissection. While the specimens were matched according to age, side, weight, bone mineral density, footprint area, and tendon thickness, a slight differing distribution in terms of sex (P = nonsignificant) (Table 1) was accepted on behalf of the former depicted factors.
Conclusion
This investigation showed that (1) there was no significant biomechanical advantage of the modified single-row repair techniques over the simple single-row repair technique and (2) the double-row repair technique was biomechanically superior to the simple single-row repair technique, but there was no significant difference between single-row repair with the modified Mason-Allen stitch and double-row repair. Hence, an argument can be made for the use of the latter as an alternative to double-row repair, as it is easier to perform.
Footnotes
Final revision submitted May 20, 2024; accepted May 23, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: The implants used in this study were provided by Arthrex. K.W., L.P.M., and M.H. have received consulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Faculty of Medicine of the University of Cologne (No. 15-318).