
Abstract
Background:
Anterior cruciate ligament reconstruction (ACLR) is a commonly performed orthopaedic procedure. As the number of ACLRs continues to increase in incidence, understanding the variability and drivers of cost to the health care system may help target cost-saving measures.
Purposes:
To examine the variability in overall 90-day reimbursements (amount paid for health care services) for ACLR using a national, multi-insurance, administrative database and to assess factors associated with variability.
Study Design:
Cross-sectional study.
Methods:
Using the M151 PearlDiver data set (data from 2010 to April 30, 2021), the authors identified the 90-day total reimbursements in patients who underwent ACLR. Patient age, sex, and comorbidity burden; insurance type; inpatient versus outpatient surgery status; and 90-day postoperative adverse events were determined and were correlated with overall reimbursements using multivariable logistic regression.
Results:
A total of 249,484 patients who underwent ACLR during the study period were identified. The mean patient age was 31.6 ± 13.58 years, 50.3% were female, the mean Elixhauser Comorbidity Index (ECI) was 1.4 ± 1.8, and procedures were performed on an outpatient basis for 245,507 patients (98.4%). Insurance type was commercial for 220,284 patients (88.3%), Medicaid for 17,660 (7.1%), and Medicare for 3500 (1.4%). The mean overall 90-day reimbursement was $4281.91 ± $4982.61 (median [interquartile range], $3032 [$1681-5142]), and the total reimbursement for the patient cohort was $1,049,250,747. On multivariable linear regression, the variables independently associated with the greatest changes in overall reimbursement were (in decreasing order) hospital readmission (+$17,675.23), adverse events (+$1554.14), inpatient procedure (+$1246.51), and emergency department visits (+$784.06). Lesser but significant associations were found with greater ECI (+$252.30) and female sex (+$101.01). Decreased overall reimbursement was associated with older age (−$12.19) and Medicare (−$883.48)/Medicaid (−$493.18) relative to commercial insurance.
Conclusion:
In the current study, large variability was found in overall ACLR reimbursement/cost within the health care system. Hospital admissions (inpatient surgery and readmission) and adverse events were associated with the greatest increase in costs and emphasize the need to optimize these metrics above and beyond patient experience.
Anterior cruciate ligament reconstruction (ACLR) is a commonly performed orthopaedic procedure; in the United States alone, >100,000 ACLRs are performed each year, and this number has continued to rise.2,3,11,15 One estimate was as high as 400,000 to 500,000 ACLRs being performed each year. 16 As such, understanding the related variability and drivers of cost to the health care system may help target cost-saving measures.
Prior studies have examined the economics surrounding ACLR and its large cost variability. A 2017 study by Stewart et al 14 found that adjusting cost data to 2015 US dollars and found ACLR costs (including facility, surgeon, and anesthesia) to vary between $4987 and $14,961, a nearly 4-fold variability. A 2017 study by Herzog et al 7 utilized the 2005-2013 Truven Health Analytics MarketScan insurance database to assess the cost of outpatient ACLR in patients with commercial insurance and found that the cost of ACLR (including any knee-related diagnosis codes) varied between around $6000 and $14,000.
A few studies have sought to analyze the variables associated with ACLR costs. The study by Stewart et al 14 evaluated additional costs associated with minor surgical complications (range, $353-$1059) and major surgical complications (range, $24,543-$73,628). A 2017 meta-analysis found that outpatient ACLR resulted in financial savings of $1371 to $7390 per procedure compared with inpatient surgery. 5 However, these studies used data sources that do not capture the totality of costs through a 90-day postoperative period for privately and publicly insured patients as well as inpatient and outpatient procedure settings. As such, costs including rehabilitation, medication, clinic visits, emergency department (ED) visits, readmissions, adverse events, need for further surgery, and more were not fully considered.
In the current study, we aimed to characterize the variability in reimbursement for ACLR as well as evaluate the variables that affect the associated costs over a 90-day postoperative period using a large multi-insurance administrative database based in the United States. The goal of this analysis was to gain a clearer understanding of the different factors that affect reimbursement for this common procedure and help provide insights that are not captured in the current literature. We hypothesized that adverse events, inpatient surgery, and hospital readmissions would lead to the greatest increase in cost.
Methods
Data Source/Study Population
The current study utilized the M151 data set from 2010 to April 30, 2021, within PearlDiver, a large national multi-insurance administrative database. M151 indicates the 151 million US patients covered in the PearlDiver data set at the time of this study. The use of PearlDiver for research has been well established in the orthopaedic literature.6,8-10,12,13 As data output is aggregated and deidentified, our institutional review board has determined that studies utilizing PearlDiver are exempt from review.
Patients who underwent ACLR were identified based on Current Procedural Terminology code 29888. To be included in the patient cohort, patients had to be active in the PearlDiver database for at least 90 days before and after surgery.
Data Elements/Analysis
Reimbursement (amount paid for health care services in 2010-2021 US dollars) data included all aspects of care including, but not limited to, the surgery, treatment interventions, testing, and clinic visits. The recipients of these reimbursements include physicians, providers, rehabilitation, and hospitals. In the current study, reimbursement analysis started on the day of surgery and continued through the 90-day postoperative period.
The variables collected and included in the analysis are as follows: patient factors (age, sex, and Elixhauser Comorbidity Index [ECI] 4 ), insurance type (commercial, Medicare, or Medicaid), surgery status (outpatient or inpatient), and 90-day postoperative events (adverse event, ED visit, and hospital readmission after surgery/discharge). Adverse events were coded using International Classification of Diseases codes and included cardiac events, surgical site infections, sepsis, deep vein thrombosis, pulmonary embolism, acute kidney injury, urinary tract infection, pneumonia, wound complications, and transfusions.
Data Analysis
First, to gain further insight into the variability of reimbursement among the patient cohort, the reimbursement spread was assessed. The data are reported as both means with standard deviations and medians with interquartile (IQR) ranges.
Next, the patient characteristic, insurance type, surgery status, and 90-day postoperative event variables were analyzed. This analysis was performed using a multivariable linear regression to determine the incremental cost associated with each variable independent from the others. A Bonferroni correction was applied, and the significance was set at P = .0063.
PearlDiver Bellwether was used to collect/abstract data and for statistical analysis.
Results
Patient Cohort
Based on the current study's inclusion/exclusion criteria, 249,484 patients who underwent ACLR were identified. The mean age of the cohort was 31.6 ± 13.58 years (median [IQR], 30 years [19-42 years]), 50.3% were female, and the mean ECI was 1.4 ± 1.8. The insurance type was commercial for 220,284 patients (88.3%), Medicaid for 17,660 (7.1%), and Medicare for 3500 (1.4%). The remaining demographic characteristics are shown in Table 1.
Characteristics of Patient Cohort (N = 249,484) a

Data are reported as n (%) unless otherwise indicated. ECI, Elixhauser Comorbidity Index; ED, emergency department; IQR, interquartile range; postop, postoperative.
Variability of Cost/Reimbursement
The spread/distribution analysis of the overall 90-day postoperative reimbursement revealed the mean reimbursement to be $4281.91 ± $4982.61. With a slight right-tailed/nonnormal distribution, the median (IQR) was $3032 ($1681-4282). The total reimbursement for the patient cohort was found to be $1,049,250,747.
Factors Associated With Cost/Reimbursement
Multivariable linear regression then allowed for the assessment of each variable's independent, incremental impact on cost/reimbursement (Table 2 and Figure 1). The variables independently associated with the greatest changes in overall reimbursement were (in decreasing order): hospital readmission (+$17,675.23), adverse events (+$1554.14), inpatient procedure (+$1246.51), and ED visit (+$784.06) (P < .0001 for all). Lesser, but significant, associations were seen with increased ECI (+$252.30) and female sex (+$101.01 relative to male sex) (P < .0001 for each). As seen in other studies, decreased overall reimbursement was associated with older age (−$12.19 per year increase) and Medicare (−$883.48)/Medicaid (−$493.18) insurance relative to commercial insurance (P < .0001 for all).
Incremental Payment Differences for Each Variable Independently Using Multivariable Linear Regression a

ECI, Elixhauser Comorbidity Index; ED, emergency department; postop, postoperative; —, not applicable.
In 2010-2021 US dollars.
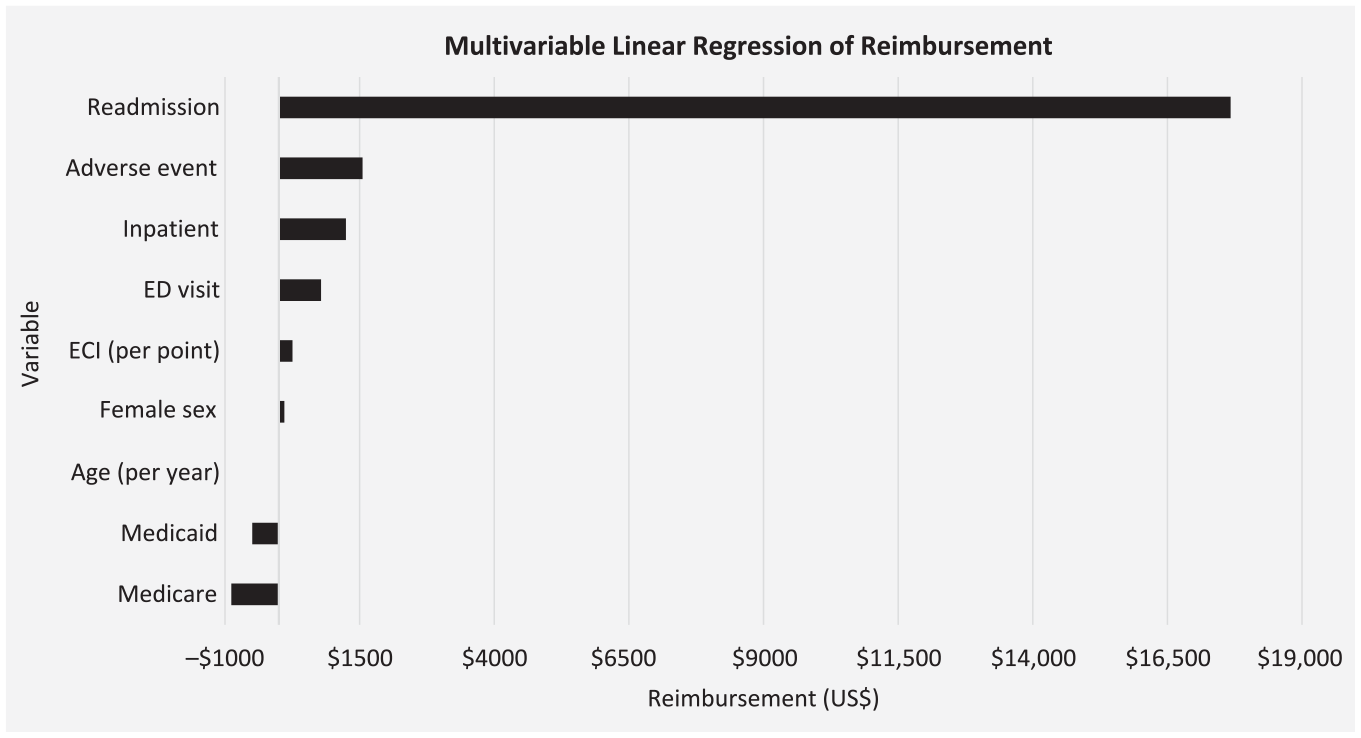
Graph showing the incremental payment differences seen in Table 2. All variables are statistically significant (P < .0001). ECI, Elixhauser Comorbidity Index; ED, emergency department.
Discussion
In the current study, we identified wide variability in 90-day postoperative reimbursement after ACLR as well as large increases in reimbursement associated with hospital readmission, inpatient surgery, and adverse events. The cohort demographics were consistent, as expected: mean age, 31.6 ± 13.58 years, 50.3% female, and low comorbidity burden (mean ECI, 1.4 ± 1.8). Furthermore, the majority of patients had commercial insurance (88.3%) compared with Medicaid (7.1%) and Medicare (1.4%). The overwhelming majority of procedures were performed on an outpatient basis (98.4%), and 90-day postoperative adverse events were low.
The mean reimbursement was $4281.91 ± $4982.61, with a right-tailed/nonnormal distribution and a median (IQR) of $3032 ($1681-4282). The large variation noted in this study is consistent with that of prior studies.5,7,14 The large variability and distribution skew to the right highlight the importance of cost analyses, as it is imperative to understand the causes of the right-tailed skew to optimize health care efficiency and reduce the frequency of postoperative events that lead to increased costs. Underscoring this, the total reimbursement for the patient cohort was $1,049,250,747.
The multivariable linear regression allowed for each variable to be isolated and the independent impact to be studied in relation to overall cost. Hospital readmission was the variable that most significantly increased the 90-day postoperative reimbursement rate (+$17,675.23). Inpatient procedures also resulted in a large increase in reimbursement (+$1246.51). These data demonstrate the increased costs associated with hospitalization, both for the original procedure and for additional postoperative events. ACLR is typically performed in outpatient settings and has a high level of patient satisfaction and functional restoration, comparable to the results of inpatient procedures. 5 In addition, there is no significant difference in risk for postoperative complications when comparing inpatient and outpatient settings. 5 Physicians should note that outpatient ACLR is more cost effective; however, the risk and cost of readmission should be analyzed when considering procedure location.
Other factors that led to a significant increase in reimbursement were adverse events (+$1554.14) and ED visits (+$784.06). These costs are to be expected, as while the effect of postoperative ACLR care on total cost has not been analyzed to date, postoperative care for other orthopaedic procedures has been shown to be associated with additional costs. 1 The way to combat these additional costs is to establish pathways that address adverse events effectively and limit postoperative costs. These pathways could include ways to optimize inpatient versus outpatient surgery while limiting readmissions. Also, further effort can be made to reduce postoperative ED visits, including patient education, telemedicine, and pain management.
Limitations
The current study does have limitations because of the administrative nature of the data. This study is dependent on the accuracy of the claims in the PearlDiver database, and the study is retrospective, so causality cannot be determined. Additionally, the reimbursement data include administrative reimbursements but do not always include out-of-pocket payment and disputed claims. Another limitation is that because we examined reimbursement from surgery through the 90-day postoperative period, we did not include any preoperative costs such as prehabilitation. Next, it was not possible to ascertain if an ED visit or readmission was because of the ACLR procedure; that said, within 90 days of surgery it was likely to be related. This study included a cohort of nearly 250,000 patients with ACLR; however, this is a subsection of the total ACLRs performed in the United States, and we were not able to include revision surgeries as a part of the reimbursement analysis. Also, as the current study examined patients over an 11-year period, the reimbursement trends could have improved over this time period. Lastly, as the patient cohort was based in the United States, the study findings may not represent global trends or data.
Conclusion
The current study examined a large cohort of almost a quarter million patients with ACLR and found large variability in overall reimbursement/cost for the health care system. Hospital admissions (inpatient surgery and readmission) and adverse events were associated with the greatest increase in costs and emphasize the need to optimize these metrics above and beyond patient experience. Further studies could look to examine if reimbursement has changed over the last decade.
Footnotes
Final revision submitted March 4, 2024; accepted March 18, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.J.H. received grant support from the Jane Danowski Weiss Family Foundation Fund at Yale University School of Medicine. M.M.D. received grant support from the Richard K. Gershon, M.D. Fund at Yale University School of Medicine. E.S. has received education payments from Gotham Surgical. M.J.M. has received consulting fees and nonconsulting fees from Smith+Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Yale University (protocol No. 2000028988).