
Abstract
Background:
Trochleoplasty has shown promising results in selected patients with patellar instability. However, concerns persist regarding its potential relationship with long-term osteoarthritis (OA) and the underlying causes.
Purpose:
To evaluate the correlation between postoperative patellofemoral incongruence after trochleoplasty and long-term OA.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The authors conducted a retrospective review of patients who underwent sulcus-deepening trochleoplasty between 2003 and 2013 and identified 43 patients after their initial search. All patients were assessed at a minimum follow-up of 10 years. Preoperative, immediate postoperative, and end-of-follow-up lateral and axial view knee radiographs were used to evaluate patellofemoral OA using the Iwano classification, the patellar articular surface angle (PA), and the trochlear articular surface angle (TA). Data on patellar redislocation, reoperations, and International Knee Documentation Committee (IKDC), Kujala, and patient satisfaction scores were also collected. Pearson correlation analysis was used to evaluate the relationship between articular surface angles and OA, and Spearman rank correlation analysis was used to assess the association between categorical and ordinal variables. A 2-tailed Student t test was used to compare the mean values of the clinical scores between groups.
Results:
Ten patients (10 knees) met the inclusion criteria, with a mean follow-up of 15.3 ± 3.93 years. The PA and TA were 148.5°± 24.75° and 148.5°± 17.85°, respectively, with a mean patellofemoral incongruence of 21.4°± 16.03°. None of the patients had preoperative OA, and 4 (40%) developed postoperative OA: 2 with Iwano grade 1 and 2 with Iwano grade 2. Higher patellofemoral incongruence was found to correlate with the development of patellofemoral OA (P = .017). No independent correlation was found between the TA and OA (P = .553) or the PA and OA (P = .884). The satisfaction, Kujala, and IKDC scores were 8.2 ± 1.75, 82.5 ± 10.09, and 84.4 ± 9.79, respectively. Only 1 patient (10%) reported a traumatic patellar dislocation, none required reoperations, and all (100%) indicated they would undergo surgery again.
Conclusion:
This study demonstrated that patellofemoral incongruence after trochleoplasty was associated with the development of long-term OA without an independent correlation with a flat trochlea or a flat patella.
Trochlear dysplasia is present in 96% of patients with patellar instability. 6 The severity of trochlear dysplasia varies, with high-grade trochlear dysplasia (Dejour grades B and D) characterized by the presence of a supra trochlear spur. 3 Trochleoplasty has been proposed as a surgical technique to eliminate the supratrochlear spur with good results. 5 Among the different techniques described, the thick-flap technique of Dejour involves osteotomies of the trochlear facets, which also allows for correcting the depth and orientation of the facets, thereby recentralizing the groove.
While trochlear dysplasia is the main origin of patellofemoral arthritis, 6 others have expressed concerns regarding the trochleoplasty effect on this arthritis development. Recent studies have found that low-grade patellofemoral osteoarthritis (OA) is still common after trochleoplasty procedures.5,15,16 These studies determined that preoperative arthritis stage largely determined long-term arthritis. However, there is a lack of evidence in the literature regarding other factors that determine the development of OA at mid- and long-term follow-ups after trochleoplasty.
The primary objective of our study was to evaluate whether the lack of congruence between the patellar and trochlear articular angles correlates with long-term patellofemoral OA. The secondary objective was to analyze whether a flat trochlea or a flat patella independently correlates with patellofemoral OA. We hypothesized that a lack of congruence between the femoral articular surface and the patella would lead to worse long-term outcomes regarding arthritis development after trochleoplasty.
Methods
The protocol for this study received ethics committee approval, and all included patients provided informed consent for the use of their data for research and publishing. We evaluated a retrospective series of 43 consecutive patients who underwent sulcus-deepening trochleoplasty between 2003 and 2013 by the senior surgeon (D.H.D.). Patients with full preoperative, postoperative, and 10-year postoperative radiographic examination consisting of weightbearing anteroposterior view, sagittal views at 30° of flexion, and axial view at 20° of flexion were included. The indications for trochleoplasty during this period of time were recurrent patellar instability (≥2 documented patellar dislocations) and high-grade trochlear dysplasia (Dejour type B or D with a supratrochlear spur >5 mm). The contraindications were patellofemoral arthritis grade 2 to 4 of the Iwano classification 12 or skeletal immaturity. The final cohort consisted of 10 patients (10 knees) (Figure 1).

Flowchart of the selection process for the final study cohort.
Surgical Technique
The surgical technique has been previously published. 10 The patient was placed in a supine position with the knee at 90° of flexion, supported laterally and distally. A midline skin incision was made, and a transquadricipital tendon approach was used.
The trochlea was prepared by marking the native groove, the medial and lateral facets, and the newly planned groove. The trochlear prominence was reduced by removing a strip of cortex around the femorotrochlear osteochondral junction. The surface under the trochlea was prepared by drilling multiple convergent tunnels through the trochlear undersurface cancellous bone and by removing the bone bridges between the tunnels. An osteotomy of the trochlear surface was performed by a cartilage incision with a surgical scalpel blade along the marked lines. A thin osteotome was used for the osteochondral cuts, and the facets were rotated slightly to increase the sulcus angle. The facets were then fixed with staples. The new trochlear groove was aligned with the femoral anatomic axis, establishing proximal realignment.
According to the preoperative measurements, a tibial tubercle osteotomy was performed in cases of excessive tibial tuberosity–trochlear groove (TT-TG) distance or patella alta. 4 Finally, the lateral retinaculum was released, and the medial patellofemoral ligament (MPFL) was reconstructed using a hamstring autograft.
Postoperative Rehabilitation
Patients were allowed full weight bearing without limitation of range of motion immediately after surgery, while for patients who underwent adjuvant tibial tubercle osteotomy, an extension brace was used, limiting flexion up to 100° for 30 days. At 45 days postoperatively, patients started performing aquatic and cycling activities, muscle reinforcement in a closed kinetic chain, and proprioceptive and postural exercises. At 3 months postoperatively, the patient was prepared to return to sport by focusing on running and plyometrics, enabling a full return to sport by 8 months.
Postoperative Assessment
All patients were evaluated at a minimum follow-up of 10 years by an independent clinician (D.H.D.). Patient history of any patellar redislocation or reoperations in the operated knee, level of satisfaction with their surgery (1 [not satisfied] to 10 [very satisfied]), return to sports, apprehension, and the International Knee Documentation Committee (IKDC) 11 and Kujala 14 scores were collected.
Imaging
Sagittal view radiographs and computed tomography scans were used to classify the trochlear dysplasia and assess the patellar height using the Caton-Deschamps index. 1 Axial view radiographs at 20° of flexion were used to evaluate the presence of patellofemoral arthritis using the Iwano classification. 12 The patellar articular surface angle (PA) and the trochlear articular surface angle (TA) were measured on axial view radiographs (Figure 2).

The articular surface angles are demonstrated on an axial view radiograph of a right knee. The patellar articular surface angle is based on the most posterior part of the patella and 2 lines along the lateral and medial facets (a), and the trochlear articular surface angle is based on the deepest point of the trochlear groove and the most prominent aspects of the medial and lateral condyles (b).
Statistical Analysis
Descriptive statistics are used to summarize the demographic data, clinical scores, and radiographic measurements. Continuous variables are expressed as mean ± standard deviation where appropriate, while dichotomous variables are expressed as the number and percentage of patients. The Shapiro-Wilk normality test was used to assess the normality of distributions.
Pearson correlation analysis was used to evaluate the relationship between the PA, the TA, and the difference between these 2 angles with OA. Spearman rank correlation analysis was used to assess correlations between categorical and ordinal variables. A 2-tailed Student t test for independent samples was used to compare the mean values of the Kujala, IKDC, and satisfaction scores between the OA group and the non-OA group. These statistical analyses were performed using SPSS (Version 25; IBM Corp). Significance was set at an alpha of P < .05.
Results
The characteristics and surgical details of the 10 study patients are presented in Table 1. The mean age at surgery was 20.4 ± 5.44 years.
Patient Characteristics and Surgical Details (N = 10 Patients) a

Data are presented as mean ± SD or n (%). MPFLR, medial patellofemoral ligament reconstruction TTO, tibial tubercle osteotomy; VM, vastus medialis.
The final flexion range was 135°± 5.2°, and none of the patients had an extension deficit. The satisfaction, Kujala, and IKDC scores were 8.2 ± 1.75, 82.5 ± 10.09, and 84.4 ± 9.79, respectively. Only 1 patient (10%) reported a traumatic patellar dislocation at 1 year postoperatively; this was managed by nonoperative treatment and did not recur over the following 11 years. None of the patients required reoperations at the end of the follow-up period. Eight of 10 patients (80%) returned to sports postoperatively, and all patients (100%) indicated they would undergo surgery again. None of the patients were evaluated with OA preoperatively. The final follow-up results are shown in Table 2.
Final Follow-up Results a

Data are presented as mean ± SD (range) or n (%). IKDC, International Knee Documentation Committee; OA, osteoarthritis; ΔPT angle, patellar angle - trochlear angle (as an absolute value).
Difference between both postoperative measurements (patellar angle and trochlear angle)
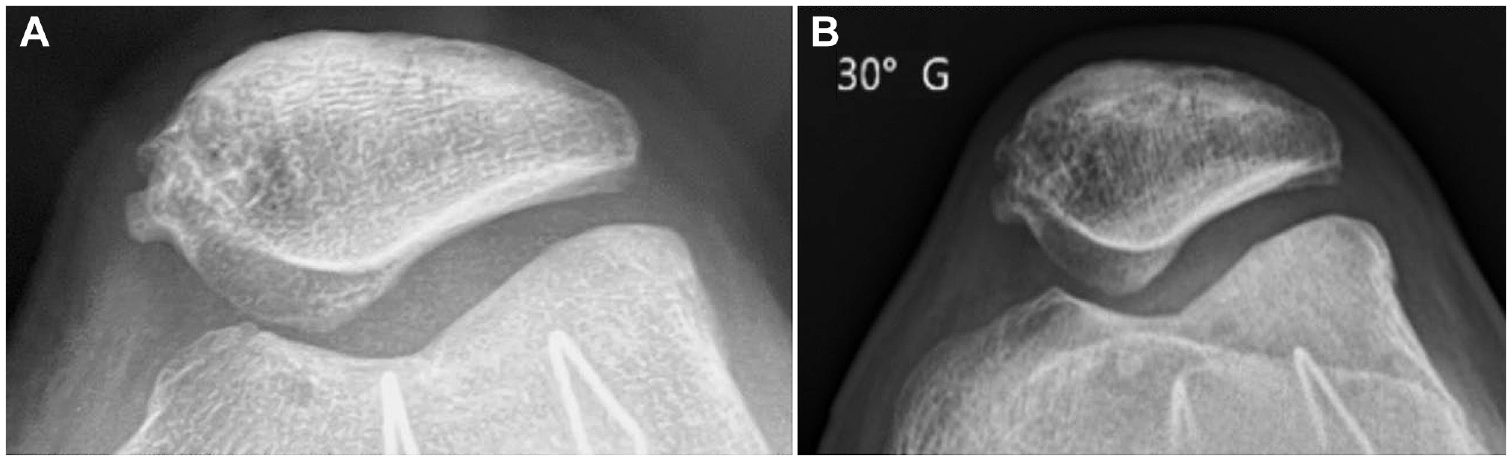
At a mean follow-up of 15.4 ± 3.93 years (range 10.4-22.9 years), 4 patients (40%) were evaluated with OA: 2 patients (20%) had Iwano grade 1 OA and 2 patients (20%) had Iwano grade 2 OA (Figure 3). The remaining patients did not show any OA (Figure 4).

Incongruent patellofemoral joint example. (A) Immediate postoperative axial view radiograph obtained in a trochleoplasty patient. (B) Axial view radiograph obtained at the 17-year follow-up after fixation device removal.
Congruent patellofemoral joint example. (A) Immediate postoperative axial view radiograph obtained in a trochleoplasty patient. (B) Axial view radiograph obtained at the 15-year follow-up.
A higher patellofemoral incongruence between patellar and trochlear angles correlated with patellofemoral OA (P = .017). When analyzed independently, no correlation was observed between the TA and OA (P = .553) or between the PA and OA (P = .884). A trend was found between the duration of follow-up and OA (P = .060) but was not statistically significant. To further investigate this finding, patients were grouped by follow-up duration (<15 vs >15 years); however, no significant difference between groups was observed (P = .363).
When we analyzed the results between patients with OA versus those without, we did not observe statistically significant differences in terms of Kujala score (P = .725), IKDC score (P = .751), or patient satisfaction (P = .494).
Discussion
The most important finding of this study was that postoperative incongruence between the articular angles of the patella and trochlea correlated with the development of OA at mid- to long-term follow-up in patients undergoing trochleoplasty, without a relationship between OA and a flat trochlea or flat patella separately. The clinical relevance of these long-term findings is that sulcus-deepening trochleoplasty with high congruence between the patella and trochlea suggests prevention of the development of OA.
Previous studies have assessed factors contributing to OA progression in patients who did not undergo trochleoplasty. Erard et al 8 investigated the effect of femoral tunnel positioning on long-term OA progression in patients with isolated MPFL reconstruction, finding no influence from tunnel malposition. Similarly, Shatrov et al 17 evaluated the impact of various factors such as preoperative body mass index, patellar height, and TT-TG distance on the progression of OA in patients who underwent isolated MPFL reconstruction, with a mean follow-up of 12.3 years (range, 10-14 years), and found no significant correlation. However, long-term evidence in series involving trochleoplasty remains limited.
A systematic review by Leclerc et al, 15 which included 1000 trochleoplasties, found that only 3 studies had a minimum follow-up of 10 years. Their study revealed that patellofemoral OA was common after trochleoplasty (117/431 knees; 27%). In a clinical study by Rouanet et al, 16 the outcomes of thick-flap trochleoplasty were evaluated at a minimum follow-up of 12 years, revealing that 65% of patients had Iwano grade ≥2 OA. In contrast, in the present study, the incidence was much lower, with only 40% having Iwano grade ≤2, and none with Iwano grade ≥3 OA.
In a recent study, Dejour et al 5 reported a 62% rate of mild patellofemoral OA (Iwano grade ≤2) without observing any cases of severe OA (Iwano grade ≥3) after a mean follow-up of 14.8 years. Similarly, in a series of patients with a mean follow-up of 24.4 years, Dejour et al 2 observed mild OA in 77% and severe OA in 22% of patients. However, none of the aforementioned studies analyzed predisposing factors for patellofemoral OA after trochleoplasty.
A recent finite element study by Kaiser et al 13 evaluated patellofemoral joint pressures of knees undergoing trochleoplasty. The study revealed that trochleoplasty knees exhibited a significant decrease in contact surface and a notable increase in contact pressures. Similarly, a dynamic simulation study by Elias et al 7 observed that while trochleoplasty effectively reduced lateral patellar maltracking, it also increased patellofemoral contact pressures. These observations support our hypothesis that reduced congruence after trochleoplasty may be a key factor in the development of OA, providing a plausible explanation for our findings and highlighting the role of evaluating the patellar morphology when planning a trochleoplasty. 9
Finally, our study did not show any differences in functional outcomes between patients with mild OA and those without OA, which is consistent with the findings of Shatrov et al 17 in patients with isolated MPFL reconstruction. This finding suggests that mild patellofemoral OA in patients with a history of patellofemoral surgery does not significantly impact functionality. However, our study was underpowered to detect such differences. Based on the distribution of OA in our cohort and the standard deviation in our data set, 43 patients would have been required to detect a mean difference of 9 points (suggested as the minimal clinically important difference) with 80% power and an alpha value of .05.
Limitations
We acknowledge some limitations that must be considered when interpreting our results. First, this was a retrospective study, and as such, it is subject to the inherent limitations and biases of the study design. Second, the small number of patients included in our study, because of the challenge of obtaining immediate postoperative radiographs to assess joint congruence, limits the generalizability of our findings. Third, cartilage damage was not systematically documented during intraoperative assessment at the time of surgery, and finally, there was potential variability in the degrees of knee flexion when obtaining the radiographs.
Conclusion
Our study demonstrated that patellofemoral incongruence after trochleoplasty is associated with the development of long-term OA without an independent correlation with a flat trochlea or a flat patella. These findings are relevant for preoperative trochleoplasty planning, especially in cases with high-grade trochlear or patellar dysplasia, permitting the optimization of patellofemoral congruency and potentially improving patient outcomes by minimizing the risk of long-term OA.
Footnotes
Final revision submitted September 30, 2024; accepted October 15, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Conseil d’Orientation Scientifique Ramsay Sante (reference No. COS-RGDS-2023-08-001-DEJOUR-D).