
Abstract
Background:
The medial ulnar collateral ligament (UCL) of the elbow joint is the primary restraint to valgus stress during the throwing motion. The flexor pronator muscles (FPMs) also stabilize the elbow joint against valgus forces; however, assessment of FPM stiffness in baseball players has been limited.
Purpose:
To use ultrasound shear wave elastography (USWE) to evaluate the change in tissue elasticity of the FPMs due to pitching.
Study Designs:
Descriptive laboratory study.
Methods:
Included were 14 healthy male amateur baseball players (mean age, 28.0 ± 2.6 years) who had played intermediate-level high school or college baseball. The tissue elasticity of the flexor digitorum superficialis (FDS) in the superficial layer of the FPMs and the flexor digitorum profundus (FDP) in the deep layer of the FPMs were measured using USWE before, immediately after, and 24 hours after a throwing session of 100 pitches. The intra- and interrater reliability of the measurements were evaluated using the Pearson correlation coefficient and intraclass correlation coefficient (ICC). The elasticity of each muscle was analyzed using repeated-measures analysis of variance followed by post hoc analysis.
Results:
Reliability of the USWE measurements was good to excellent (intrarater ICCs, 0.78-0.94; interrater ICCs, 0.85-0.96). The mean tissue elasticity values before, immediately after, and 24 hours after pitching were 22.3 ± 4.4, 41.0 ± 13.8, and 38.3 ± 11.2 kPa, respectively, for the FDS and 27.1 ± 5.8, 48.0 ± 22.3, and 29.6 ± 11.5 kPa, respectively, for the FDP. For both the FDS and FDP, elasticity was significantly higher immediately after pitching than before pitching (P < .001 and P = .0027, respectively). While the elasticity of the FDS at 24 hours after pitching remained significantly higher compared with before pitching (P = .0011), the elasticity of the FDP at 24 hours decreased to the same level as before pitching (P = .91).
Conclusion:
Results using USWE indicated that the elasticity of the FDS did not decrease 24 hours after pitching and remained significantly higher than before pitching, suggesting that it may not be fully functioning as a dynamic stabilizer during this period.
Clinical Relevance:
Pitching in such a condition may result in greater stress on the UCL and increase the risk of UCL injury.
Keywords
The medial ulnar collateral ligament (UCL) of the elbow joint is the primary restraint for valgus stress. 27 During the throwing motion, the tensile load on the UCL is estimated to exceed its failure strength. 1 Repetitive valgus stress leads to UCL injuries; therefore, baseball players are at risk of medial elbow injury due to repetitive throwing. According to previous reports, dynamic contraction of the flexor pronator muscles (FPMs) plays a key role in stabilizing the elbow joint against valgus forces.18,28 Several anatomic, electromyographic, and cadaveric biomechanical studies have demonstrated that the FPMs protect the UCL by dynamically stabilizing it. ‡ As the elasticity of human tissue is an indicator of its quality or condition, measurement of elasticity could be useful in assessing skeletal muscle activity.
Heers et al 22 demonstrated that the elasticity of muscles determined using magnetic resonance elastography (MRE) was linearly correlated with muscle activity. However, MRE is affected by the measurement environment, such as location, space, and patient positioning. Ultrasound elastography appears to be more suitable than MRE for measuring muscle activity in clinical settings because it offers real-time in vivo measurements in less restricted postures and joint positions. Ultrasound elastography, which includes strain elastography and acoustic radiation force impulse imaging, has been developed to evaluate tissue stiffness.4,7,37 However, both strain elastography and acoustic radiation force impulse imaging are semiquantitative methods of measuring tissue elasticity. Additionally, strain elastography requires manual pressure; thus, it is operator dependent, and its reproducibility is questionable.
Recently, ultrasound shear wave elastography (USWE), which provides quantitative information on the elasticity of human tissue and is more operator independent, 3 has gained increasing attention for the evaluation of muscle stiffness.8,9 The principle is that the acoustic radiation force produced by a transducer creates shear waves, the velocity of the shear waves is measured as they travel through the tissue, and the elasticity (Young modulus) of the tissue can be calculated using this velocity. 5 Differences in elasticity are important for distinguishing pathological changes from normal conditions, and previous studies using shear wave elastography have reported significant differences in shear wave velocity between intact and torn Achilles tendons. 17 It has also been reported that an increase in muscle stiffness immediately after exercise results in muscle fatigue and microdamage.2,13,23,26 However, there is limited evidence on the quantitative assessment of FPM stiffness after throwing in baseball players.
The purpose of this study was to assess the change in tissue elasticity of FPMs due to throwing using USWE. We hypothesized that the elasticity value of FPM stiffness measured using USWE would increase owing to pitching stress.
Methods
Participants
The study included 14 healthy amateur male baseball players (mean age, 28.0 ± 2.6 years) who had played intermediate-level high school or college baseball and who volunteered to participate. The inclusion criterion was the ability to throw fastballs without pain or symptoms in the shoulder, elbow, hand, or other parts of the body, including the hip joint. Participants were excluded from the study if they had pain during throwing action; had a history of orthopaedic shoulder, elbow, or hand surgery; or had pitched in the 24 hours before the study measurements. Institutional review board approval was received for the study protocol, and all study participants provided written informed consent.
Setup and Protocol
We followed the throwing protocol described by Hattori et al. 21 Measurements commenced after the participants performed a preparation routine of full-body stretching and a warm-up of approximately 10 pitches. Pitching was performed on a standard pitching mound (ie, 18.44 m [60 feet 6 inches] away from the back point of home plate). The pitching protocol consisted of 100 fastballs (20 sets of 5 pitches at intervals of 15 seconds) with maximum effort from the set position toward the simulated strike zone.
Measurements
Measurements were obtained using a linear transducer (14L5 MHz) with an Aplio 500 Platinum ultrasound machine (Toshiba Medical Systems). Tissue elasticity values of the superficial and deep layers of the FPMs were measured before and after throwing using USWE. The superficial layer is mainly composed of the flexor digitorum superficialis (FDS) and flexor carpi ulnaris. The deep layer is mainly composed of the flexor digitorum profundus (FDP). In this study, the tissue elasticity of the FDS in the superficial layer of the FPMs and that of the FDP in the deep layer of the FPMs were measured at 3 time points: before, immediately after (0 hours), and 24 hours after pitching. The measurement location was 5 cm distal to the humeroulnar joint.
Both the superficial and deep layers were detected in the ultrasound brightness-mode (B-mode) image (Figure 1). All the muscles were located with the transducer oriented axially. The transducer was then turned perpendicular to the plane and oriented longitudinally to measure the stiffness. Using USWE, we measured tissue elasticity at 3 random points in each muscle. The circular region of interest was 5 mm in diameter and was placed parallel to the muscle fibers in the longitudinal view, such that it did not include vessels or surrounding structures of any of the muscles (Figure 2). Three valid measurements were recorded for each muscle layer, and the mean of the measurements was calculated. The USWE values were recorded in elasticity mode in kilopascals (0-80 kPa).

The superficial and deep layers of the flexor pronator muscles (FPMs) were detected 5 cm distal to the humeroulnar joint using ultrasound B-mode. (A) Short-axis view showing the flexor digitorum superficialis (FDS) and flexor carpi ulnaris (FCU), comprising the superficial layer of the FPMs, and the flexor digitorum profundus (FDP), comprising the deep layer of the FPMs. (B) Long-axis view. Measurements of the FDS in the superficial layer of the FPMs and the FDP in the deep layer of the FPMs were performed in this view.

Assessment of the stiffness of the flexor pronator muscles using shear wave elastography (SWE). Shown is an ultrasound image of the flexor digitorum superficialis. The blue rectangle indicates the region of interest (ROI). Measurements were performed at 3 random points (white rectangles) in each muscle.
Two experienced sonologists (Y.M. and A.I.) independently performed the ultrasound assessments. Intrarater reliability of the measurements was calculated from the difference of 3 valid measurements for each parameter, and interrater reliability was calculated from the difference of their mean of measurements.
Statistical Analysis
All data were analyzed using SPSS Statistics software (Version 22.0; IBM Corp) and are expressed as mean with standard deviation. The intra- and interrater reliabilities of the ultrasound measurements were evaluated using the Pearson correlation coefficient and intraclass correlation coefficient (ICC), respectively, and were interpreted as poor (<0.40), moderate (0.40-0.60), good (0.61-0.80), or excellent (>0.80). The sequential changes in the mean elasticity values of the respective muscles at the 3 time points (before, immediately after, and 24 hours after pitching) were analyzed using repeated-measures analysis of variance, followed by a post hoc analysis. Statistical significance was set at a P value <.05.
Results
Table 1 shows the ICCs for the intra- and interrater reliabilities for the elasticity measurements of each muscle tested. The intrarater ICCs ranged from 0.78 to 0.94, whereas the interrater ICCs ranged from 0.85 to 0.96.
Reliability of Ultrasound Measurements for Muscle Elasticity a

FDP, flexor digitorum profundus; FDS, flexor digitorum superficialis; ICC, intraclass correlation coefficient.
The tissue elasticity values of the FDS before, immediately after, and 24 hours after pitching were 22.3 ± 4.4, 41.0 ± 13.8, and 38.3 ± 11.2 kPa, respectively. FDS elasticity was significantly higher immediately after and 24 hours after pitching compared with before pitching (P < .001 and P = .0011, respectively). However, there was no significant difference in elasticity between immediately after and 24 hours after pitching (P = .80) (Figure 3A). The tissue elasticity values of the FDP before, immediately after, and 24 hours after pitching were 27.1 ± 5.8, 48.0 ± 22.3, and 29.6 ± 11.5 kPa, respectively. FDP elasticity immediately after pitching was significantly higher compared with before pitching (P = .0027) and 24 hours after pitching (P = .0085) (Figure 3B). Thus, while the elasticity of the FDS at 24 hours after pitching remained significantly higher compared with before pitching (P = .0011), the elasticity of the FDP at 24 hours decreased to the same level as before pitching (P = .91).
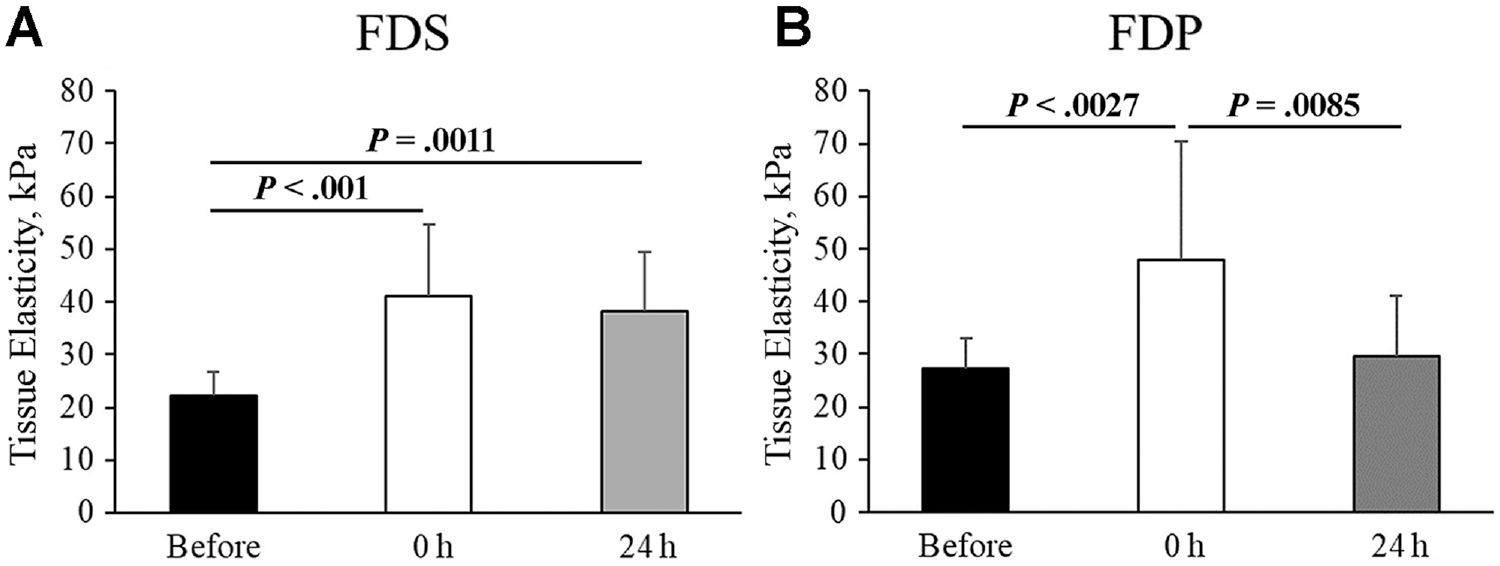
The elasticity of the (A) flexor digitorum superficialis (FDS) in the superficial layer of the FPMs and the (B) flexor digitorum profundus (FDP) in the deep layer of the FPMs before, immediately after (0 h), and 24 hours after throwing 100 pitches.
Discussion
In this study, in which sequential changes in the elasticity of FPMs due to pitching were measured using USWE, the elasticity values of the FDS and FDP were significantly higher immediately after pitching than before pitching (P < .001 and P = .0027, respectively). Although the elasticity of the FDP 24 hours after pitching decreased to the same level as before pitching (P = .91), the elasticity of the FDS remained significantly higher 24 hours after pitching (P = .0011). These results suggest that the FDS plays the most significant role among the FPMs against the valgus force applied to the elbow during pitching.
USWE is a novel noninvasive method for quantitatively assessing the elasticity or stiffness of tissues. Recent studies have used shear wave elastography to assess the stiffness of the Achilles tendon,6,10,16,30 patellar tendon, 34 rotator cuff,11,12,19,26,31,36 and UCL18,38 and have reported better reproducibility than conventional methods of assessment. In the present study, the ICCs for intra- and interrater reliability were considered good to perfect, 24 ranging from 0.78 to 0.94 and 0.85 to 0.96, respectively. These findings suggest that USWE is a highly reproducible mode of assessment.
The maximum valgus force is applied across the elbow during the cocking and acceleration phases of throwing, with the peak force generated immediately before ball release. 13 During the acceleration phase, the forearm is gradually pronated, and the wrist and finger flexors are in eccentric contraction. Therefore, forearm pronators, wrist flexors, and finger flexors might stabilize the elbow against valgus forces, especially during ball release. The role of the FPMs as dynamic stabilizers has been described in anatomic, electromyographic, and biomechanical studies. Frangiamore et al 15 showed in an anatomic study that tendon fibers of the FCU, pronator teres, and FDS merge in close proximity to the anterior bundle of the UCL, with the FDS tendon attached along 45.6% of the distal length of the anterior bundle and the FCU tendon overlapped with 20.9% of the distal footprint of the anterior bundle of the UCL. In another study, Frangiamore et al 14 reported that this anatomic feature may be a contributing factor to the higher failure rate of nonoperative management of distal UCL tears compared with proximal tears in professional pitchers. Davidson et al 11 also reported that the FCU and FDS were optimally oriented in line with the UCL to contribute to dynamic elbow valgus stability. Clinical electromyography studies aimed at defining the flexor contraction pattern during pitching motion have reported that pitchers with symptomatic valgus instability have decreased flexor pronator mass activity. 20 In a biomechanical study, Park and Ahmad 29 evaluated the role of the flexor pronator group using UCL-deficient elbow models and reported that contraction of the FCU and FDS resulted in the greatest stability of the UCL-deficient elbow compared with the other surrounding musculature.
To our knowledge, there are no reports on muscle activity of the FDP during throwing, but the FDP has the largest physiological cross-sectional area of forearm muscles and can output the highest muscle strength. The muscle activity of the FDP is thought to be similar to that of the FDS, and since the FDS demonstrates maximum muscle activity during the acceleration phase,12,17 the FDP should also demonstrate its greatest muscle activity during the same phase. In the current study, the tissue elasticity values of the FDS and FDP immediately after pitching were significantly higher than their values before pitching, suggesting that these muscles function as dynamic stabilizers for elbow valgus stability during throwing, as previously reported. 34
Udall et al 35 conducted a cadaveric biomechanical study and reported that the FDS was the largest contributor among the FPMs during throwing; other biomechanical studies have demonstrated that the FCU is the primary stabilizer for achieving elbow valgus stability.25,29 Our results showed that the elasticity value of FDS did not decrease 24 hours after pitching and remained significantly higher than before pitching, indicating that the FDS plays a particularly important role among the FPMs. Furthermore, the increased elasticity of the FDS suggests that the FDS was fatigued and may not be fully functioning as a dynamic stabilizer during this period. Pitching in such a condition may result in greater stress on the UCL and increase the risk of UCL injury. Therefore, it is important to measure the elasticity of the FDS over time after pitching to confirm improvement in elasticity and check for abnormalities in the elasticities of the FDS and FDP before pitching. To the best of our knowledge, this is the first report to assess the change in elasticity of the FPMs after throwing using USWE. This technology can measure muscle elasticity noninvasively with high reproducibility, suggesting that it may be a useful method to identify the potential risk of UCL injury by measuring changes in muscle elasticity over time before and after throwing.
Limitations
A limitation of this study was that the participants were amateur baseball players who had played at the intermediate level in high school or college. It is possible that the results would be different for professional pitchers with a higher level of competition. However, the findings of this study suggest that USWE can be used to measure the elasticity of throwing-related muscles around the elbow before and after pitching, regardless of the level of competition, and we would like to perform further studies on professional pitchers in the future.
Conclusion
Results using USWE indicated that the elasticity of the FDS did not decrease 24 hours after pitching and remained significantly higher than before pitching, suggesting that the FDS plays an important role among the FPMs against elbow valgus force during throwing.
Footnotes
Final revision submitted May 13, 2024; accepted May 20, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kobe University Graduate School of Medicine (ref No. B210009).