
Abstract
Background:
Achilles tendinopathy is a common condition without a reproducible and timely treatment modality. Platelet-rich plasma (PRP) injection has been proposed as an enticing treatment option, but there is no consensus regarding its effectiveness.
Purpose:
To pool the available data and evaluate the evidence of the effect of PRP injections on Achilles tendinopathy.
Study Design:
Systematic review; Level of evidence, 1.
Methods:
This review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. CINAHL via EBSCOhost, Cochrane Library, and PubMed databases were searched for randomized controlled trials comparing PRP injection with nonoperative treatment, with the Victorian Institute of Sport Assessment–Achilles (VISA-A) questionnaire score or maximal Achilles tendon (AT) thickness on ultrasound as outcome measures. Risk-of-bias assessment was performed of the included studies, and meta-analyses compared differences in outcome measures between PRP injection and control at the short-term (3-month), intermediate-term (6-month), and long-term (12-month) follow-ups.
Results:
Of 409 publications, 6 publications (N = 422 patients with chronic midportion Achilles tendinopathy) were identified from the literature search. Risk-of-bias assessment revealed 2 studies were low risk, 1 was of some concern, and 3 were high risk of bias. Meta-analysis revealed no significant differences between PRP injection and control at any time point for both VISA-A score (short term: P = .29; intermediate term: P = .42; long term: P = .57) and maximal AT thickness (short term: P = .60; intermediate term: P = .20; long term: P = .55).
Conclusion:
Our review demonstrated that although recent trends have shown an increasing popularity of PRP injection, no solid evidence has been established. The heterogenicity of the tendinopathy pathology and the PRP injection content and methodology should be controlled by better-designed clinical trials. Further research is needed before it should be recommended as a standard treatment.
Achilles tendinopathy is a common pathology with a prevalence of 5.6% among the general population.9,32 In elite endurance athletes, lifetime incidence can reach 50%,22,23 with a mean time loss from training or games of 18.4 days. 19 The Achilles tendon (AT) plays a major role in force transmission during walking, running, and jumping, 5 making it especially susceptible to overload. Unfortunately, poor vascularization and other factors potentially limit its repair capability. 26 Treatment of Achilles tendinopathy should be timely to avoid complications, including “degenerative” AT rupture. 30
Several therapies, including shockwave therapy, eccentric training, pulsed electromagnetic field therapy, and orthopaedic insoles, have been demonstrated to have beneficial effects on Achilles tendinopathy.1,20,24 However, each has limitations, including poor patient adherence to prolonged and intensive treatment protocols and intolerance to discomfort, such as shockwave therapy.
Platelet-rich plasma (PRP) injection is a relatively common injection therapy under the umbrella of regeneration medicine. PRP is a platelet-concentrated part of autologous blood consisting of growth factors and cytokines that are hypothesized to promote tissue healing when injected. 10 Positive effects have been shown in laboratory settings, but conflicting results have been reported in various clinical trials.3,4,7,12,15
In this study, we aimed to systematically analyze the evidence of the effect of PRP injection for the treatment of Achilles tendinopathy. The Victorian Institute of Sport Assessment–Achilles (VISA-A) questionnaire score and maximal AT thickness were examined as indices of functional outcomes and impairment level, respectively. We hypothesized that PRP injection would improve AT function and reduce maximal AT thickness.
Methods
This review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 guidelines. Covidence was used for bibliographic management. Two reviewers (C.T.-K.M. and J.P.-Y.L.) worked independently on the eligibility of studies and risk-of-bias assessment. In case of disagreements, consensus was achieved through discussion, and a third reviewer (S.K.-K.L.) was called in to make the decision.
Literature Search
The CINAHL via EBSCOhost, Cochrane Library, and PubMed databases were searched. Keywords used were (Achilles) AND ((platelet-rich plasma) OR (PRP)) in all databases. No filter was adopted in any search engines. The last search was on May 2, 2022.
Inclusion/Exclusion Criteria
All articles obtained were screened for eligibility, first by title and abstract then by full text retrieved. The inclusion criteria followed the PICOS (Population, Intervention, Comparison, Outcomes, and Study design) principles, as follows: (1) population: clinical or ultrasonographic diagnosis of Achilles tendinopathy; (2) intervention: PRP injection; (3) comparison: sham injection (saline injection or no injection) or other forms of nonsurgical intervention; (4) outcomes: VISA-A score or maximal AT thickness; and (5) study design: randomized controlled trials (RCTs). We excluded studies with (1) nonadult population; (2) nonhuman population; (3) surgical interventions involved; (4) non-English language; and (5) full text unavailable.
Risk-of-Bias Assessment
The risk of bias of the included studies was assessed with the Cochrane risk-of-bias tool for randomized trials (Version 2). Each study's overall risk of bias was judged based on 5 domains: randomization process, deviation from intended intervention, missing outcome data, measurement of the outcome, and selection of the reported result. The risk of bias was classified into low, some concerns, or high.
Data Extraction and Analysis
Data extraction was based on the following areas: (1) study protocols (study design and settings); (2) participant characteristics (demographics, disease severity, and disease duration); (3) treatment regimens of the treatment group and comparison group (injection type, injection method, dosage, and cointerventions); and (4) outcomes (reported results, mean difference [MD] with 95% CI).
The primary outcomes of interest were VISA-A scores and maximal AT thickness on ultrasound. Secondary outcomes were satisfaction (at the latest follow-up) and any adverse event reported. The VISA-A is a self-administered questionnaire on the severity of Achilles tendinopathy. 27 It covers 3 domains (pain, function, and participation) in 8 questions. A total score of 0 indicates the highest severity, and 100 indicates the lowest severity. There is no diagnostic cutoff for VISA-A. Maximal AT thickness measures AT thickening in the anteroposterior aspect. It is a sign of Achilles tendinopathy and can be measured clinically with ultrasound imaging. It is widely accepted that a thickness >8 mm is regarded as thickening. 29
Three postintervention time points were considered: short term (3 months), intermediate term (6 months) and long term (12 months). When there were multiple assessments at a similar time point, the measurement nearest to that time point was extracted. If postintervention and change-from-baseline values were available, the former was extracted. If only graphical presentations of outcomes were available, Plot Digitizer 2.6.9 (Joseph A. Huwaldt) was used for data extraction, and they were excluded from the quantitative analysis. In case of missing data, the estimates of the effect of intervention were considered in the following order: (1) intention-to-treat analysis; (2) modified intention-to-treat analysis (examining the effect of random assignment to group but excluding the participants responsible for missing data); and (3) per-protocol analysis. Unadjusted MDs were obtained instead of adjusted MDs when both were presented. All continuous data were reported as mean ± standard deviation unless otherwise specified. Differences between groups were reported as MD with 95% CIs.
Statistical Analysis
A meta-analysis was conducted on all primary outcomes. Review Manager (Revman) 5.3 was used for all data entry and analysis. As all studies shared the same scales on the outcome variables, the MDs were pooled. Statistical heterogeneity was identified with the chi-square test, and the I2 statistic was calculated. The greater the I2, the greater the inconsistency among studies. Random-effects models were adopted for all comparisons. The level of significance was set at P < .05.
Results
Study Selection
Overall, 409 records were identified from the 3 databases after our initial search. Of these publications, 7 reports6,8,13,17,18,21,31 from 6 studies6,13,17,18,21,31 were included in this study (Figure 1). The 1-year follow-up of the study by de Vos et al 13 was published by de Jonge et al 8 ; in the current review, the results from de Vos et al 13 (short term and intermediate term) and de Jonge et al 8 (long term) were considered a single entity and were referred to as de Vos et al. 13

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 flowchart indicating research article inclusion for final analysis.
Summary of the Included Studies
In total, there were 422 participants in the 6 included studies. They were all patients with chronic Achilles tendinopathy; no studies involved patients with insertional Achilles tendinopathy. The study protocol and baseline participant characteristics of each study can be found in Tables 1 and 2, respectively.
Study Protocols of the Included Studies a

MRI, magnetic resonance imaging; PRP, platelet-rich plasma; RCT, randomized controlled trial; SVF, stromal vascular fraction.
Sample sizes correspond to (1) Victorian Institute of Sport Assessment–Achilles questionnaire and (2) maximal Achilles tendon thickness.
Only the placebo group was considered the comparison group in this review.
Sample size analyzed for maximal Achilles tendon thickness.
Sample size analyzed for the short-term outcomes.
Baseline Participant Characteristics of the Included Studies a

Data are presented as mean ± SD, mean (range), or median [interquartile range] unless otherwise indicated. AT, Achilles tendon; NA, not applicable; PRP, platelet-rich plasma; VISA-A, Victorian Institute of Sport Assessment–Achilles.
Table 3 shows the interventions used in each study. Volumes of 3 to 6 mL of PRP were used in the included studies. During the preparation of PRP, the centrifugation time ranged from 5 to 15 minutes, and the centrifugation speed ranged from 1500 to 3200 RPM. The centrifugation speed was not specified by de Vos et al, 13 and Kearney et al 17 reported relative centrifugal force instead of centrifugation speed. This was also the only study that adopted a 2-staged centrifugation. 17
Treatment Regimens of Included Studies a

Dashes indicate areas not applicable. PRP, platelet-rich plasma; RCF, relative centrifugal force; RPM, revolutions per minute; SVF, stromal vascular fraction.
Additional injection at 2 months for participants with pain visual analog scale >3 and American Orthopaedic Foot & Ankle Society score <70.
Two weeks between each injection.
Two studies17,31 specified the use of leukocyte-rich PRP. Four studies specified the use of ultrasound-guided injection,6,13,21,31 and the remaining studies did not. PRP was injected into both intratendon and peritendon space in 2 studies6,31 and only to the intratendon space in the other 4 studies.13,17,18,21 PRP was injected once only in 4 studies.13,17,18,21 Usuelli et al 31 did not report the number of participants who received a second injection. Both groups in the study by Boesen et al 6 received corresponding injections 4 times with a 2-week interval between injections.
Regarding the comparison groups, saline was used in 3 studies,6,13,21 dry insertion in 1 study, 17 stromal vascular fraction injection in 1 study, 31 and eccentric exercise in 1 study. 18 Eccentric exercise was part of the cointervention in 3 other studies.6,13,21 Apart from Krogh et al, 21 who did not report these data, the eccentric training consisted of 180 repetitions of eccentric heel-drop exercise daily for 12 weeks, as suggested in the protocol of Alfredson et al. 2
Risk of Bias of the Studies
The risk-of-bias assessment indicated that 2 studies13,17 had a low risk of bias, 1 study 6 had some concerns, and 3 studies18,21,31 had a high risk of bias (Figure 2). All studies demonstrated low risk of bias in terms of randomization process and deviations from intended interventions. The injecting physicians were unable to be blinded in 3 studies6,17,18 due to the study design, but there was no evidence that deviation from the protocols occurred; hence, they were classified as having low risk of bias according to the algorithm. Massive dropout leading to a high risk of bias in missing outcome data was observed in the study by Krogh et al. 21 Their study also had some concerns regarding the selection of reported results, as the original statistical analysis plan focused on long-term results. 21

Summary of risk of bias according to (A) bias domains and (B) included studies.
Two studies13,17 had low risk of bias in terms of measurement of the outcome. The other studies did not have outcome assessors blinded. Regarding VISA-A scores, participants (ie, the outcome assessors) were not blinded in 2 studies,18,21 and Usuelli et al 31 did not report whether participants were blinded in their study. Regarding maximal AT thickness, 2 studies6,21 did not have the assessing physicians blinded.
Outcomes
All studies reported short-term and intermediate-term results (only graphical presentation was available in the study by Usuelli et al 31 ), and 3 studies6,13,21 reported long-term results.
Primary Outcomes
All studies reported VISA-A scores. Although there were trends favoring PRP injection over control, no significant difference was found at any time point (short term: MD, 2.28 [95% CI, –1.95 to 6.51], P = .29; intermediate term: MD, 1.83 [95% CI, –2.66 to 6.32], P = .42; long term: MD, 3.46 [95% CI, –8.62 to 15.55], P = .57) (Table 4 and Figure 3).
Summary of VISA-A Scores a

Data in brackets represent 95% CIs. Dashes indicate areas not applicable. MD, mean difference; PRP, platelet-rich plasma; VISA-A, Victorian Institute of Sport Assessment–Achilles.
Data extracted from the figures.
Only adjusted means available.

Forest plot of VISA-A scores between PRP injection and control groups at (A) short-term (3-month), (B) intermediate-term (6-month), and (C) long-term (12-month) follow-up after intervention. The long-term outcomes for de Vos et al 13 were published by de Jonge et al. 8 IV, inverse variance; PRP, platelet-rich plasma; VISA-A, Victorian Institute of Sport Assessment–Achilles.
Four studies reported max AT thickness. One study reported the results at all time-points, 6 and the other 3 studies reported results at short-, 21 intermediate-, 31 and long-term 11 follow-up time points, respectively. Trends favoring PRP injection over control were shown at intermediate- and long-term follow-up. Nonetheless, no statistically significant difference was identified at all time points (short term: MD, 0.26 [95% CI, –0.71 to 1.24], P = .60; intermediate term: MD, –0.84 [95% CI, –2.12 to 0.43], P = .20; long term: MD, –0.28 [95% CI, –1.19 to 0.64], P = .55) (Table 5 and Figure 4).
Summary of Studies Reporting Maximal AT Thickness a
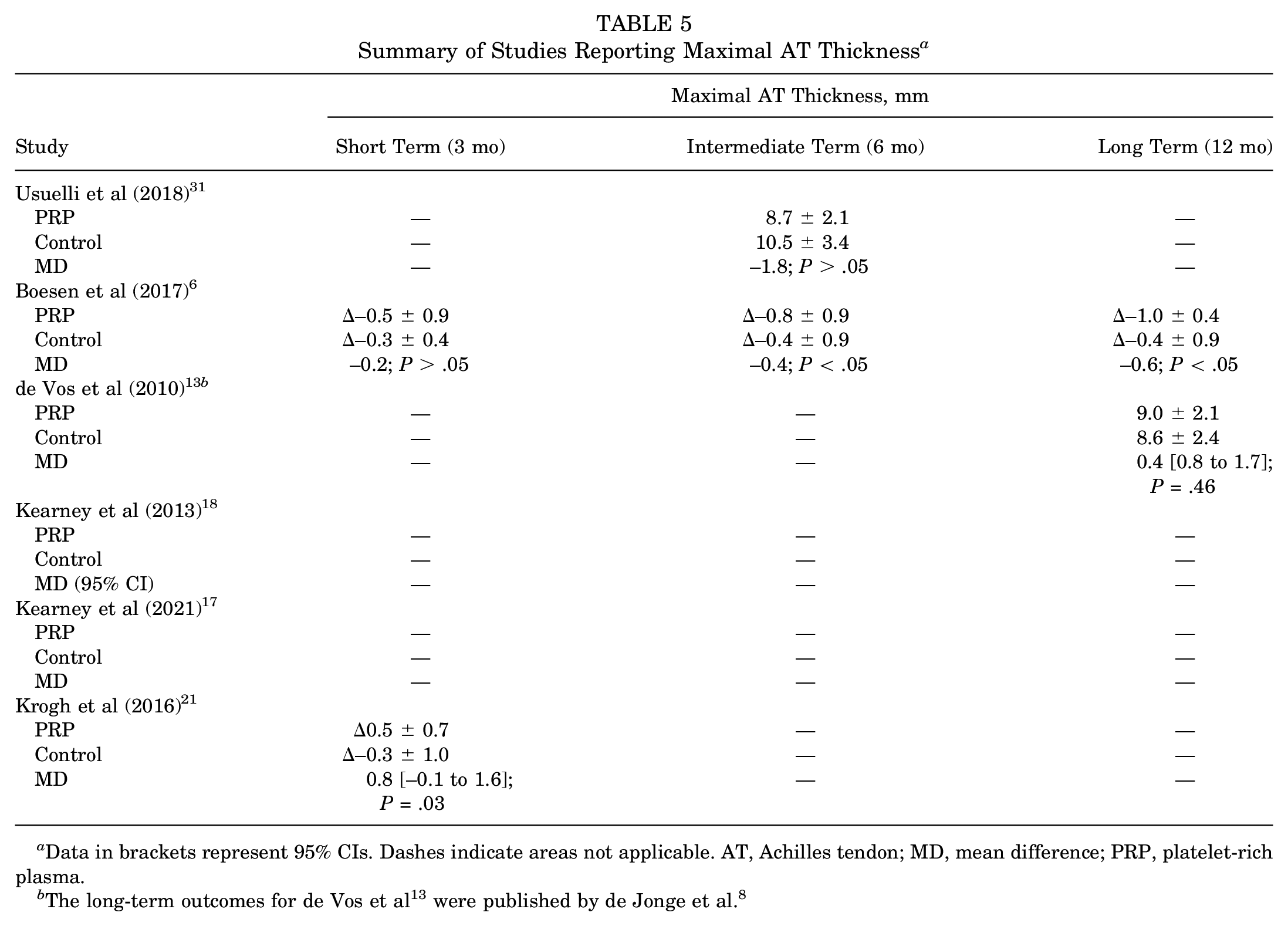
Data in brackets represent 95% CIs. Dashes indicate areas not applicable. AT, Achilles tendon; MD, mean difference; PRP, platelet-rich plasma.

Forest plot of maximal Achilles tendon thickness between PRP injection and control groups at (A) short-term (3-month), (B) intermediate-term (6-month), and (C) long-term (12-month) follow-up. The long-term outcomes for de Vos et al 13 were published by de Jonge et al. 8 IV, inverse variance; PRP, platelet-rich plasma.
Secondary Outcomes
Only 2 studies assessed participants’ satisfaction with the treatment. Boesen et al 6 reported that 58% and 42% of participants in PRP group and control group, respectively, were satisfied with the allocated injection. However, de Vos et al 13 reported that 56% and 63% of participants in the PRP group and the control group, respectively, were satisfied with the allocated injections. 8 No conclusions on whether PRP injection was more satisfying than control could be drawn.
No infections, hematomas, or ruptures were reported in the studies, with 1 exception. One participant experienced severe pain and required surgical intervention in the pilot study of Kearney et al 18 in 2013. One participant experienced severe pain and required surgical interventions in Kearney et al.’s RCT in 2021. 17 The incidence of mild side effects including bleeding, bruising, swelling, and mild discomfort at the injection site was also reported as common side effects, but few lasted for 6 months. 17
Discussion
This systematic review with meta-analysis analyzed 6 publications with a total of 422 participants having chronic midportion Achilles tendinopathy. There was no significant evidence to support the hypotheses that, compared with control, PRP injection improves VISA-A scores (short term: P = .29; intermediate term: P = .42; long term: P = .57) and that PRP injection reduces maximal AT thickness (short term: P = .60; intermediate term: P = .20; long term: P = .55). These findings are consistent with results from other published articles.4,11,12,15
As illustrated by the risk-of-bias assessment, the 6 included studies contributed to a broad coverage of methodological qualities. The 2 studies with low risk of bias provided nonsignificant results.13,17 The majority of flaws in the quality of studies can be accounted for by a lack of blinding. Only de Vos et al 13 achieved a triple-blinded trial (blinding of those delivering the interventions, the patients, and the outcome assessors). 8
While the studies by Boesen et al 6 showed the best results of PRP injection, there are some concerns over its risk of bias, as the physician assessing tendon thickness was not blinded. Nevertheless, a better baseline condition in the study of Boesen et al 6 may imply some ideal circumstances in which PRP injection excelled: younger patients, less severe symptoms, and early intervention during disease onset. The superior results in the Boesen et al 6 study can also be explained by the multiple injections, which may have allowed prolonged exposure to growth factors to complete the tissue repair process. 3
One major source of inconsistency in results leading to the inconclusive effectiveness of PRP injection in treating Achilles tendinopathy is proposed to be the variability of PRP injection protocols and techniques employed in the different studies. Different injection methods in the studies may have led to inconsistent results. The use of ultrasound-guided injections can improve the accuracy in injecting PRP to the desired location, 7 but it was only reported in 4 studies.6,13,21,31 In addition, the difference in the exact site of injection may give rise to the distinction of results. In the studies by Boesen et al 6 and Usuelli et al, 31 where results were more favorable toward PRP injection, PRP was injected to both the tendon body and the surrounding tissue. Kearney et al suggested that needling to the tendon body itself potentially poses a therapeutic effect. 18 However, whether the effect is beneficial or detrimental remains unclear.
Another factor influencing the outcomes is the content injected. Depending on the centrifugation speed and time, the concentration of different components in PRP would be different; the composition of PRP in the included studies was likely different, contributing to variable therapeutic effects. For instance, the concentration of platelets may be directly related to the amount of growth factors produced. Leukocyte-rich or leukocyte-poor PRP preparation has been debated, with different pathologies responding differently. A high concentration of leukocytes has been suggested to trigger inflammatory responses that may not benefit tendon regeneration.16,33,34 Of the studies on Achilles tendinopathy, none has declared the use of leukocyte-poor PRP. Notwithstanding, the exact level of different components in PRP that can produce the best results remains unclear. Composition analysis of the PRP is suggested before injection to better clarify the mechanisms behind this treatment. 25
Future studies are expected to involve large double-blind RCTs with appropriate randomization and blinding processes to produce high-quality, more reliable evidence guiding the clinical use of PRP to elicit statistically significant improvement in terms of functional outcomes and impairment levels in patients with Achilles tendinopathy. Standardization and categorization in the collection of existing PRP classification systems, such as those summarized by Rossi et al, 28 in monitoring PRP preparation and administration methods may be hugely beneficial.
Limitations
The main limitation of this review remains the high degree of heterogeneity among the included RCTs for quantitative analysis. Heterogeneity may stem from the etiologies of and risk factors for Achilles tendinopathy, the stage of tendinopathy, the method of PRP preparation, the cellular composition of PRP, the technique of injection, the dose and frequency of injection, and the control group design. Because of the lack of standardization and categorization in PRP preparation and administration methods, we were unable to reach a consensus on PRP biologics based on the current review.
Moreover, we were unable to analyze PRP in different subgroups, such as age and sex, as data were not reported in such detail in previous literature. As interest grows and analysis of larger patient cohorts becomes feasible, subgroup analyses should evaluate the potential differential effect of PRP treatment in patients with different baseline characteristics so that the utilization of PRP in treating Achilles tendinopathy can be further characterized and optimized.
It should be noted that the results cannot be generalized to insertional Achilles tendinopathy, in which pathology occurs at the bone-tendon junction rather than the tendon body. The 2 conditions also differ regarding the occurrence of calcification and the level of vascularity. A systematic review showed promising results of PRP injections on insertional Achilles tendinopathy in a retrospective study, but no prospective RCT wasavailable to cobboratethe results. 14
Conclusion
Our review demonstrated that although recent trends show an increasing popularity of PRP injection, no solid evidence has been established. The heterogenicity of the tendinopathic pathology and the PRP injection content and methodology should be controlled by better-designed clinical trials. While regenerative medicine and biologics are hoped to be a “holy grail” for many challenging pathologies such as Achilles tendinopathy, further research is needed before PRP injection should be recommended as a standard treatment. Patients should be educated on the available evidence regarding PRP injections in Achilles tendinopathy prior to considering this treatment option.
Footnotes
Acknowledgements
The authors appreciate the staff in the Department of Orthopaedics and Traumatology at The Chinese University of Hong Kong for their support throughout this study.
Final revision submitted April 16, 2024; accepted May 2, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.