
Abstract
Background:
Nonprimary osteochondral lesions of the talus (OLT) pose a significant challenge in orthopaedics, with no definitive consensus on optimal surgical treatment.
Purpose:
To consolidate the most recent evidence on operative treatments for nonprimary OLT by assessing patient-reported outcomes (PROs), postoperative complications, and clinical failures.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
This review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 and PRISMA in Exercise, Rehabilitation, Sport medicine and Sports science guidelines. Searches were conducted in PubMed, Embase, and Cochrane Library databases through June 2023. Eligible studies evaluated operative outcomes in skeletally mature patients with nonprimary OLT after failed previous surgeries. Primary outcomes included clinical and functional PROs. Secondary outcomes included postoperative complications and clinical failures. Quantitative analyses involved weighted means, mean differences, minimal clinically important differences, success rates (95% binomial proportion confidence interval), and a pre-to-postoperative meta-analysis.
Results:
Out of 3992 identified records, 50 studies involving 806 ankles from 794 patients were included. All operative treatments significantly improved PROs (P < .05), except osteochondral allograft transplantation (OCA) for American Orthopaedic Foot and Ankle Society and pain (visual analog scale/numeric rating scale [VAS/NRS]) scores and HemiCAP for pain (VAS/NRS) scores. Autologous chondrocyte implantation (ACI) and osteochondral autologous transplantation (OAT) demonstrated the greatest PRO success rates, exceeding 80%. Postoperative complications occurred in 4% of cases, most frequently with HemiCAP. Clinical failures affected 22% of cases, particularly with autologous matrix-induced chondrogenesis, OAT, OCA, and HemiCAP.
Conclusion:
Our systematic review demonstrated that ACI and OAT are promising treatments for nonprimary OLT, with ACI showing fewer clinical failures than OAT. Conversely, OCA and HemiCAP exhibited lower effectiveness and higher clinical failure rates, suggesting a need for reassessment.
Keywords
Osteochondral lesions of the talus (OLTs) present considerable clinical challenges because of their complexity and the risk of severe morbidity. These lesions typically involve both the talar articular cartilage and subchondral bone, crucial for talar stability. 79 The limited regenerative capacity of articular cartilage often leads to inadequate self-repair, 12 potentially accelerating early stage osteoarthritis development and adversely affecting patients’ mobility and quality of life.13,66,68,75 Nonoperative treatments often result in high failure rates, with less than half of the lesions responding favorably.80,85
Bone marrow stimulation (BMS) has emerged as a primary surgical option for symptomatic OLT, demonstrating good to excellent outcomes in 72% to 90% of patients.17,50,53,74,80,82,93 However, less favorable results have been reported for larger and uncontained defects.16,17 Alternative interventions have been explored – such as autologous chondrocyte implantation (ACI), matrix-assisted autologous chondrocyte transplantation (MACT), bone marrow-derived cell transplantation (BMDCT), autologous matrix-induced chondrogenesis (AMIC), and osteochondral autologous/allograft transplantation (OAT/OCA). Each technique presents its challenges – including cost, technical complexity, potential donor site morbidity, and immunogenicity. a Metal resurfacing implants have recently gained attention for treating large lesions; nonetheless, their long-term efficacy is still under investigation.24,25,54,83,86
The current literature on BMS for failed primary OLT shows inconsistent improvements in patient-reported outcomes (PROs) and a high rate of clinical failures.6,19 Research on various surgical procedures for secondary OLT has not yet clearly distinguished between all the different treatment strategies available. 52
This systematic review aimed to consolidate recent evidence on operative interventions for nonprimary OLT, focusing on clinical and functional PROs as primary outcomes and postoperative complications and clinical failures as secondary outcomes. We hypothesized that there would be significant variability in outcomes among different operative treatments for nonprimary OLTs but comparable results between different operative treatments.
Methods
This systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) 2020 guidelines and PRISMA in Exercise, Rehabilitation, Sport medicine and Sports science guidelines.5,61 The protocol was preregistered at PROSPERO (CRD42023425676).
Eligibility Criteria
Eligibility criteria were based on the Population, Intervention, Comparator, Outcomes, and Study Design framework. Only full-text studies published in English were included, without publication date restrictions.
Population
We included studies involving skeletally mature patients with symptomatic OLT who had failed previous operative treatments. The exclusion criteria were patients with immature skeletons, OLT in joints other than the ankle, primary OLT, lesions not exclusively located on the talar dome, established ankle osteoarthritis or inflammatory arthritis, and previous ankle surgeries unrelated to cartilage procedures.
Intervention and Comparator
All operative cartilage procedures were considered. The exclusion criteria comprised nonoperative treatments and unspecified revision procedures. Comparator groups were compulsory for inclusion; however, studies comparing different operative methods were used for comparison between interventions.
Outcomes
Primary outcomes included preoperative and last recorded postoperative clinical and functional PRO measures, postoperative subjective satisfaction, return to work (RTW), and return to sports (RTS) to any and preinjury levels. Secondary outcomes encompassed postoperative complications and clinical failures. Trials were excluded if they did not report any primary or secondary outcomes and lacked quantitative data analysis.
Study Design
We included all published clinical studies, from randomized controlled trials to case designs. All other study designs were excluded. At least 5 patients per trial/group were required for inclusion.
Search Strategy
A comprehensive search was conducted on PubMed and EMBASE databases and the Cochrane Library until June 30, 2023 (Supplemental Table S1). Manual searches of reference lists from included studies and relevant reviews complemented database searches.
Study Selection
Database results were managed using EndNote (Clarivate Analytics, Version 20.5), with duplicate removal and independent review by 2 authors (R.C.C. and I.M.). Disagreements were resolved by a third author (C.M.). In cases of overlapping populations, the criteria prioritized studies with longer postoperative follow-up, larger patient samples, focus on nonprimary OLT, and publications reporting various methodological approaches, rather than spreading them across multiple papers. b To obtain specific data on nonprimary OLT, authors were contacted via email, when necessary. Failure to obtain this data resulted in study exclusion or data omission.
Data Extraction
Three authors (R.C.C., I.M., and C.M.) performed the data extraction and review using an Excel spreadsheet (Microsoft Corporation, Version 16.79.1) for study details, population, and lesion characterization; previous operative treatments; and outcome measures. The level of evidence (LoE) for each study was assessed according to the Oxford Centre for Evidence-based Medicine. 90 Operative success was defined as achieving a follow-up result with an American Orthopaedic Foot and Ankle Society (AOFAS) score of ≥80, visual analog scale (VAS) or numeric rating scale (NRS) for pain score of ≤2, or subjective patient satisfaction with patients reporting satisfaction or willingness to undergo the procedure again.
Postoperative complications included wound infection/delayed wound healing, thromboembolism, and nerve or tendon injury. Clinical failures were defined as any revision surgery, except symptomatic hardware removal on the malleolar osteotomy and second-look arthroscopy evaluation.
Data Management
Data were summarized using either proportions or weighted pooled means and standard deviations, employing imputation methods for missing standard deviations as described in the Cochrane Handbook. 18 When means and standard deviations were only available in figures, these were extracted using WebPlotDigitizer (Ankit Rohatgi, Version 5.2). 84
Risk of Bias
The risk of bias for each study was evaluated using the Risk of Bias Assessment tool for Non-randomized Studies 44 across 6 domains—including selection of participants, confounding variables, performance bias, detection bias, attrition bias, and reporting bias (Supplemental Table S2). The risk was judged as low, high, or unclear. Two authors (R.C.C. and I.M.) independently assessed both the LoE and the risk of bias, with discrepancies resolved through discussion.
Data Synthesis
Data were categorized into 4 groups as follows: cartilage repair, cartilage regeneration, cartilage substitution, and rescue procedures. The mean changes were calculated as the difference between the last recorded pre- and postoperative PRO values. The percentage of the mean change relative to the minimal clinically important difference (MCID) for each PRO was determined based on existing research: 2.7 for the VAS, 42 2 for the NRS, 71 and 8.9 for the AOFAS. 20 The 95% binomial proportion confidence interval for each study was calculated using the Wilson score interval (Confidence Interval Analysis for Windows, Version 2.2.0). Simple pooling methods were used to combine data from different studies with similar methodologies. Excel and SPSS (IBM SPSS Statistics, Version 22.0) were employed for further statistical analyses.
A pre-to-postoperative meta-analysis was performed to display the pooled effect sizes in a forest plot using a random-effects model to calculate the effect size (Cohen’s d). The effect size magnitude was interpreted as large (>0.8), moderate (0.5-0.79), or weak (0.2-0.49). The forest plot was segmented using the operative technique for each main outcome.
Because of a lack of homogeneous comparative studies, a traditional meta-analysis was not feasible. Subgroup analyses specific to age, sex, or lesion size were not possible because of unsegmented data in the included studies.
Results
Search Results
Database and manual searches yielded 3992 records. After screening titles and abstracts, 469 studies were selected for full-text analysis, with 50 meeting the eligibility criteria for inclusion (Figure 1). c

The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) flowchart of the search process and study selection. OLT, osteochondral lesions of the talus.
Study Characteristics
Most studies were published in the last 10 years (since 2013), with 36% (18/50) published within the last 5 years (since 2018). The majority employed a retrospective design (31/50 [62%]), and only 14% (7/50) included a comparison group. Regarding LoE, 86% (43/50) were classified as level 4 (Supplemental Table S3).
Risk of Bias
All studies exhibited a high risk of bias in at least 1 domain, with 64% (32/50) demonstrating a high risk across ≥4 domains (Figure 2). Studies were frequently judged to have a high risk of selection bias, attributed to the selection of participants (32/50 [64%]) and confounding variables (49/50 [98%]), as well as performance (42/50 [84%]) and detection (41/50 [82%]) bias. Fewer studies exhibited a high risk of attrition (11/50 [22%]) and reporting bias (14/50 [28%]).
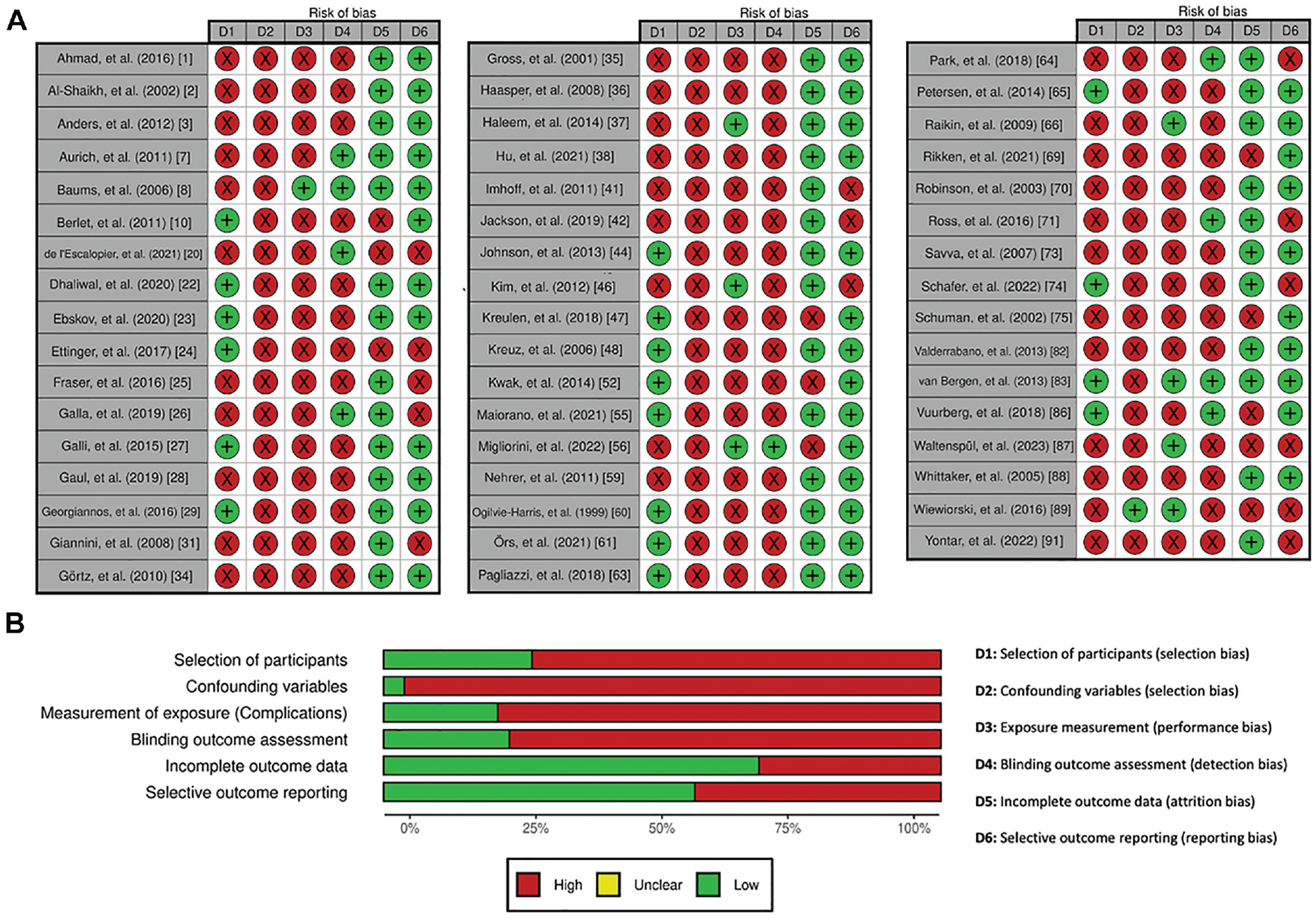
Risk of bias judgment: (A) study-level and (B) overall summary of all included studies.
Population Characteristics
The analysis included 806 ankles from 794 patients, with a weighted mean age of 36 ± 5 years. Among these patients, 57% (365/639) were men. Ankle laterality distribution was even (166/321 [52% right ankles]). The OLT location was predominantly medial (481/631 [76%]), followed by lateral (140/631 [22%]). The weighted mean lesion area and volume were 167 ± 90 mm2 and 1906 ± 2121 mm3, respectively. The weighted mean follow-up period was 53 ± 58 months (Supplemental Tables S3 and S4).
Characteristics of Operative Treatments
Cartilage substitution was the most common treatment (327/806 ankles [41%]) – including 30% OAT (238/806) and 11% OCA (89/806). Cartilage regeneration, comprising 37% (298/806 ankles), included 9% ACI (76/806), 8% MACT (65/806), 2% BMDCT (20/806), and 17% AMIC (137/806). Rescue procedures/HemiCAP and cartilage repair/BMS accounted for 14% (111/806 ankles) and 9% (70/806 ankles), respectively (Supplemental Table S3).
Clinical and Functional Outcomes
Clinical and functional PROs improved postoperatively across all treatments. The AOFAS, VAS/NRS for pain scores, and postoperative subjective satisfaction were reported in 54% (27/50), 48% (24/50), and 46% (23/50) of the studies, respectively (Supplemental Table S4).
Clinical Failures by Operative Treatment a

ACI, autologous chondrocyte implantation; AMIC, autologous matrix-induced chondrogenesis; BMS, bone marrow stimulation; MACT, matrix-assisted autologous chondrocyte transplantation; NR, not reported; OAT, osteochondral autologous transplantation; OCA, osteochondral allograft transplantation.
The AOFAS (k = 18 studies and n = 320 ankles) mean improvement ranged from 13 to 57.8 (MCID, 146% to 649%), with OAT (k = 5 studies and n = 100 ankles) showing the most and least pronounced mean change (Table 1). The pre-to-postoperative meta-analysis revealed significant improvements across all treatments (P < .05), except for OCA, which showed no significant improvement (Figure 3). The highest success rates were seen with ACI (k = 2 studies; 30/36 ankles [83%]) and OAT (k = 3 studies; 21/23 ankles [91%]), whereas HemiCAP (k = 1 study; 5/12 ankles) had the lowest (Table 2 and Supplemental Table S5).
Improvement in Outcome Measures by Operative Treatment a
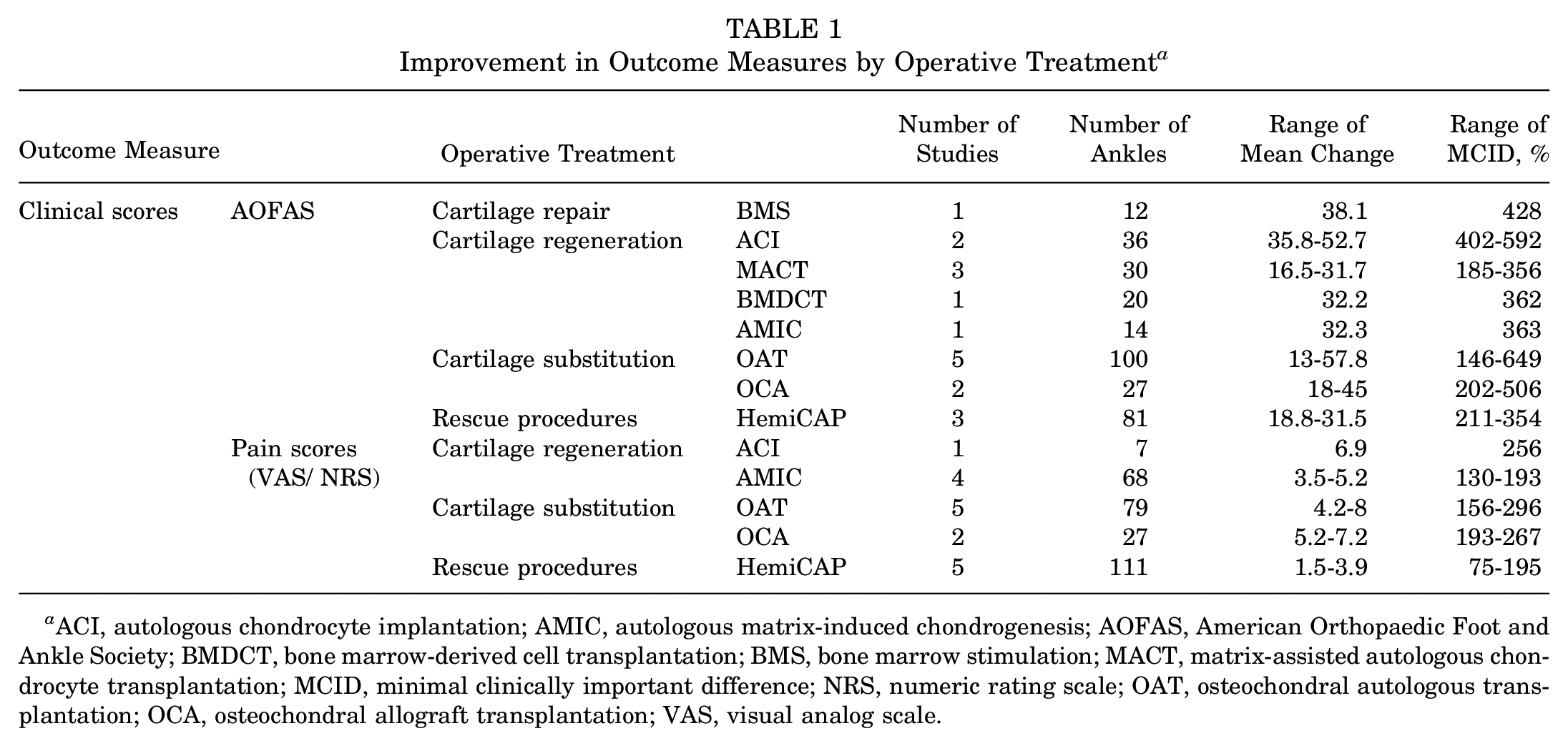
ACI, autologous chondrocyte implantation; AMIC, autologous matrix-induced chondrogenesis; AOFAS, American Orthopaedic Foot and Ankle Society; BMDCT, bone marrow-derived cell transplantation; BMS, bone marrow stimulation; MACT, matrix-assisted autologous chondrocyte transplantation; MCID, minimal clinically important difference; NRS, numeric rating scale; OAT, osteochondral autologous transplantation; OCA, osteochondral allograft transplantation; VAS, visual analog scale.
Success Rate in Outcome Measures by Operative Treatment a

ACI, autologous chondrocyte implantation; AMIC, autologous matrix-induced chondrogenesis; AOFAS, American Orthopaedic Foot and Ankle Society; BMS, bone marrow stimulation; MACT, matrix-assisted autologous chondrocyte transplantation; NRS, numeric rating scale; OAT, osteochondral autologous transplantation; OCA, osteochondral allograft transplantation; RTS, return to sports; RTW, return to work; VAS, visual analog scale.

The forest plot of pre-to-postoperative AOFAS score for each operative technique. ACI, autologous chondrocyte implantation; AMIC, autologous matrix-induced chondrogenesis; AOFAS, American Orthopaedic Foot and Ankle Society; BMDCT, bone marrow-derived cell transplantation; BMS, bone marrow stimulation; MACT, matrix-assisted autologous chondrocyte transplantation; OAT, osteochondral autologous transplantation; OCA, osteochondral allograft transplantation.
Pain scores (VAS/NRS) (k = 17 studies and n = 292 ankles) showed mean improvements ranging from 1.5 to 8 (MCID, 75% to 296%), with OAT (k = 5 studies and n = 79 ankles) displaying the most pronounced mean change and HemiCAP (k = 5 studies and n = 111 ankles) the lowest mean change (Table 1). The pre-to-postoperative meta-analysis revealed significant improvements across most treatments (P < .05), with ACI demonstrating a large effect size, while OCA and HemiCAP showed no significant improvements (Figure 4). The highest success rates were observed with ACI (k = 1 studies; 7/7 ankles) and OAT (k = 4 studies; 31/35 ankles [89%]), while HemiCAP (k = 2 studies; 4/22 ankles [18%]) had the lowest success rate (Table 2 and Supplemental Table S6).

The forest plot of pre-to-postoperative pain scores (VAS/NRS) for each operative technique. ACI, autologous chondrocyte implantation; AMIC, autologous matrix-induced chondrogenesis; BMS, bone marrow stimulation; NRS, numeric rating scale; OAT, osteochondral autologous transplantation; OCA, osteochondral allograft transplantation; VAS, visual analog scale.
There was a high success rate of postoperative subjective satisfaction (k = 23 studies and n = 346 ankles) across all operative treatments, with AMIC (k = 1 study; 11/18 ankles) and HemiCAP (k = 4 studies; 60/80 ankles [75%]) having the lowest rates (Table 2 and Supplemental Table S7). The RTW (k = 11 studies and n = 148 ankles) success rate was high across all operative treatments, with OCA (k = 2 studies; 8/13 ankles) having the lowest rate (Table 2 and Supplemental Table S7). The RTS at any level (k = 13 studies and n = 127 ankles) success rate was high across all operative treatments, except with MACT (k = 2 studies; 9/14 ankles) and OCA (k = 1 study; 2/5 ankles). The RTS at preinjury level (k = 11 studies and n = 103 ankles) success rate was low across all operative treatments, with MACT (k = 2 studies; 4/14 ankles) and OCA (k = 1 study; 0/5 ankles) having the lowest rates (Table 2 and Supplemental Table S7).
Postoperative Complications and Clinical Failures
Postoperative complications (k = 33 studies; 22/553 ankles [4%]) were not frequent across all operative treatments, except for HemiCAP, which had the highest incidence (k = 5 studies; 13/111 ankles [12%]) (Table 3 and Supplemental Table S8).
Postoperative Complications by Operative Treatment a

ACI, autologous chondrocyte implantation; AMIC, autologous matrix-induced chondrogenesis; BMDCT, bone marrow-derived cell transplantation; BMS, bone marrow stimulation; MACT, matrix-assisted autologous chondrocyte transplantation; OAT, osteochondral autologous transplantation; OCA, osteochondral allograft transplantation.
Clinical failures (k = 26 studies; 102/471 ankles [22%]) were more frequent with AMIC (k = 3 studies; 17/64 ankles [27%]), OAT (k = 5 studies; 32/144 ankles [22%]), OCA (k = 6 studies; 14/72 ankles [19%]), and HemiCAP (k = 5 studies; 31/111 ankles [28%]) (Table 4 and Supplemental Table S9).
Discussion
The primary findings of this systematic review highlight the superior efficacy of ACI and OAT in improving PROs, with ACI exhibiting fewer clinical failures than OAT. Conversely, HemiCAP and OCA demonstrated lower PROs and higher clinical failure rates, suggesting their limited effectiveness as revision procedures for nonprimary OLT. Despite the promising potential of ACI and OAT, the high risk of bias across the included studies warrants a cautious interpretation of these results.
This review offers a novel perspective, distinct from previous studies that focused on BMS6,19 and various operative treatments 52 for nonprimary OLT. By excluding patients with non-talar dome lesions, our review minimizes selection bias, which was overlooked in previous reviews.6,19 Our review emphasizes the importance of postoperative complications and clinical failures in assessing the safety and efficacy of these procedures. 52 Moreover, our established minimum threshold of 5 patients per study ensures external validity, 6 and the unique disaggregation of outcome scores reduces clinical heterogeneity, providing a more detailed understanding of treatment impact.19,52 Our review also highlights a notable increase in recent literature on this subject, with over a third of the included studies published in the last 5 years. d Notably, our review is the first to comprehensively evaluate the HemiCAP procedure, filling a gap in existing literature. Overall, this systematic review provides a broader and more current overview of the evidence, offering a deeper insight into the impact of each operative treatment on PROs, postoperative complications, and clinical failures.
Clinical and Functional Outcomes
PROs improved significantly across most treatments, demonstrating the general effectiveness of these techniques for nonprimary OLT. ACI and OAT showed substantial improvements and higher success rates compared with HemiCAP and OCA.
Regarding BMS procedures, this review observed significant improvements in AOFAS and VAS/NRS pain scores, exceeding the MCID, with a high rate of postoperative subjective satisfaction. These findings contrast with those of previous reviews reporting more modest improvements, with AOFAS and VAS pain scores similar to or below the MCID and an overall pooled success rate of 61%.6,19 RTW and RTS at any and preinjury levels showed comparable results. 19
A previous review 52 focused on various operative treatments reported overall pooled success rates of 90% for OAT, 73% for MACT, 65% for mosaicplasty, 59% for ACI, and 55% for OCA. These results contrast with the more favorable outcomes observed for ACI in our systematic review.
The newest findings pertain to the HemiCAP procedure, showing nonsignificant improvements in VAS/NRS pain scores and lower success rates in PROs. This suggests that the applicability of this technique in secondary OLT needs to be reconsidered before it is recommended for daily clinical practice.
Postoperative Complications and Clinical Failures
An overall low rate of postoperative complications was observed in this review, with the highest rates seen with HemiCAP. Previous reviews on BMS for nonprimary OLT reported a rate ranging between 0% 6 and 10%. 19 High clinical failure rates were seen with AMIC, OAT, OCA, and HemiCAP. Previous reviews on BMS for nonprimary OLT reported a much higher rate of clinical failure, ranging between 27% 19 and 33%. 6 Although both ACI and OAT are effective treatments, the higher rates of clinical failures associated with OAT suggest that ACI might be a more reliable option. However, it is important to note that the limited number of studies focusing on the ACI procedure may impact the generalizability of these results.
Future research should focus on adopting standardized and rigorous methodologies – particularly randomized controlled trials – to compare the effectiveness of operative interventions for treating nonprimary OLT. Studies should also explore the impact of lesion size, location, patient characteristics, and previous surgical histories on revision surgery outcomes. Standardizing validated outcome measures and conducting long-term follow-up studies are crucial for assessing these interventions’ durability and long-term effects.
Limitations
We acknowledge several limitations – including those related to the available studies – that have an inherent high risk of selection and detection bias because of the nonrandomization and lack of blinding in the included studies. The retrospective nature and the predominance of case series in the research also limit the strength of the conclusions. The variability in study designs and outcome measures poses challenges for direct comparisons between different treatments. The low proportion of studies with comparison groups precluded the possibility of conducting a traditional meta-analysis. Insufficient reporting of demographic variations and lesion characteristics restricted the scope of subgroup analyses. The use of nonvalidated outcome measures for treating OLT affects the internal validity of the results. Even though data were pooled for indirect comparisons, the clinical heterogeneity of included studies introduces confounding variables that could influence outcomes.
Conclusion
Our systematic review demonstrated that ACI and OAT are promising treatments for nonprimary OLT, with ACI showing fewer clinical failures than OAT. Conversely, OCA and HemiCAP exhibited lower effectiveness and higher clinical failure rates, suggesting a need for reassessment.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241296434 – Supplemental material for Operative Treatment of Nonprimary Osteochondral Lesions of the Talus: A Systematic Review
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241296434 for Operative Treatment of Nonprimary Osteochondral Lesions of the Talus: A Systematic Review by Rui Correia Cardoso, Renato Andrade, Inês Monteiro, Cátia Machado, Filipe Sá Malheiro, Pedro Serrano, Paulo Amado, João Espregueira Mendes and Bruno S. Pereira in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted July 23, 2024; accepted July 30, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.