
Abstract

Introduction
Osteochondral defects (OCDs) of the talus comprise all lesions of the talar articular cartilage and its subchondral bone. Arthroscopic bone marrow stimulation is the preferred surgical treatment for primary OCDs up to 10 mm in diameter and 5 mm in depth. 2 Nevertheless, superiority over other treatments has not been proven. 1
Several attempts have been made to treat OCDs, such as osteochondral transplantation, 3 autologous chondrocyte implantation, 7 and metal surfacing. 8 However, these techniques are associated with donor site morbidity, poor bone grafting, implant failure, or involve 2-stage surgery.5,6 An individualized treatment, based on patient and defect characteristics, is advised. 6 Therefore, we present a case with a 2-year follow-up in which an os trigonum (OT) was harvested and used as an autograft to treat the OCD of the ipsilateral talus.
Case Report
A 66-year-old man was referred to the orthopaedic outpatient clinic because of continuous deep pain in the left ankle joint without instability. At physical examination, the leg alignment was neutral, there was no swelling, and the range of motion was normal and symmetric. There was a recognizable tenderness on palpation at the anteromedial side of the talus with the ankle in plantarflexion. The ankle was stable, and posterior impingement tests were negative.
Radiographs of the left ankle revealed a large cystic OCD of the medial talar dome. The additional computed tomography (CT) scan confirmed the OCD, measuring 15 × 15 × 13 mm (Figure 1). In addition, the CT scan showed the presence of a large OT of 15 × 12 × 20 mm (Figure 1). After informed consent, the patient was scheduled for a medial malleolus osteotomy with debridement of the OCD and transfer of the OT into the cystic defect.

(A) Coronal and (B) sagittal views of the preoperative CT scan showing the cystic osteochondral defect and the os trigonum.
Operative Technique
A curved incision was made somewhat posterior to the medial malleolus, since the OT had to be harvested. The posterior joint capsule was opened, and the OT was removed in 1 piece, with the flexor hallucis longus and neurovascular bundle kept to the medial side.
Next, 2 screw holes were predrilled in the medial malleolus, whereafter the medial malleolus osteotomy was performed. The OCD became visible and an oval incision of the cartilage was made to preserve as much healthy cartilage as possible and to prevent the cartilage from rupturing in the next steps. All cystic and necrotic bone was removed with a curette and chisel (Figure 2B) and the autograft recipient was (micro)drilled for bone marrow stimulation using a 2.0-mm drill. Parts of cancellous bone of the medial malleolus were used to fill the bottom of the cyst. The proximal cortical bone was removed of the OT and prepared for optimal fitting (Figure 2A). The graft should be 1 mm larger in all directions (anteroposterior, mediolateral diameter, and depth). Once the optimal fitting shape was reached, the OT was placed into the host site with the layer of cartilage on top. By means of an impactor, the inserted autograft was fitted approximately 1 to 2 mm underneath the level of the talar cartilage (Figure 2C). The osteotomy was reduced and fixated with 3.5-mm lag screws, and the wound was closed in layers.

(A) The os trigonum (OT) was removed, (B) the osteochondral defect of the talar dome became visible and the cystic lesion was debrided, and (C) the OT was press fitted into the defect.
Postoperative Management
The postoperative management consisted of cast immobilization until union of the malleolar osteotomy was confirmed on radiographs. Full weightbearing was built up in 2 weeks and physiotherapy was started.
Outcome
Overall, the recovery went well. Six months after surgery, the patient was able to walk 5 km and cycle 60 km without pain. From the 6-month follow-up onward, the range of motion was normal.
Questionnaires were administered before surgery as well as at the 6-month, 1-year, and 2-year follow-up. As shown in Tables 1 and 2, there was a reduction of pain and an improvement of the total Foot and Ankle Outcome Score (FAOS) during follow-up. Lastly, the American Orthopaedic Foot & Ankle Society ankle-hindfoot score (AOFAS) improved from 45 points before surgery to 85 points at the 1-year follow-up and 98 points at the 2-year follow-up.
Visual Analog Scale (VAS) Score Before Surgery and at 6 Months and 1 Year After Surgery.

Foot and Ankle Outcome Score (FAOS) in Total and on the 5 Subscales Before Surgery As Well As 6 Months, 1 Year, and 2 Years After Surgery.

Abbreviation: ADL, activities of daily living.
The osteotomy line was not fully consolidated at 6-week follow-up, resulting in 3 weeks’ extension of cast immobilization. At 9 weeks’ follow-up, the radiograph showed full consolidation, after which weightbearing was allowed. The imaging during follow-up showed a properly filled OCD (Figures 3 and 4).

(A) Coronal and (B) sagittal views of the postoperative computed tomographic scan showing a fully consolidated medial malleolus and a properly filled osteochondral defect.
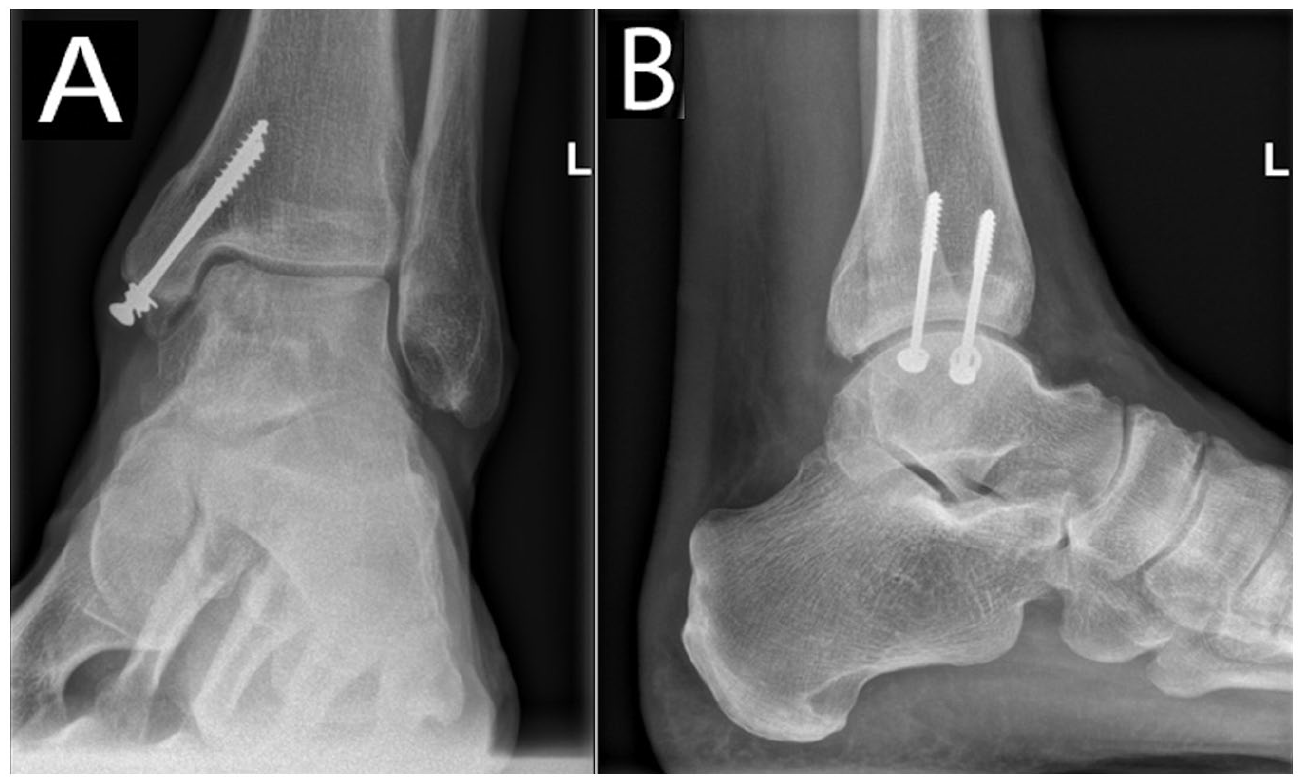
(A) Coronal and (B) sagittal views of the radiograph at 2-year follow-up.
Discussion
To our knowledge, this prospective case report is the first clinical report using an autologous OT as donor graft to treat a large cystic talar OCD. It provides insight into this specific surgical technique and its clinical follow-up.
Alternative treatments for large cystic talar OCDs include among others osteochondral transplantation, autologous chondrocyte implantation, and metal surfacing.3,7,8 However, autologous osteochondral transplantation is known for its donor site morbidity, and allograft osteochondral transplantation is associated with high failure and revision rates. 4 A considerable disadvantage of autologous chondrocyte implantation is the involvement of a 2-stage surgery. 7
The exact indications for the use of an OT as an autograft transplant are not yet known. However, it seems to have multiple advantages. First, it is thought to prevent donor site morbidity because the removal of an OT is a relatively safe procedure. 3 Second, harvesting the OT can be done in a single-stage surgery without an additional incision. Third, the OCD can be restored with the hyaline cartilage of the OT’s subtalar surface.
Grafting with an OT is a strongly individualized surgical technique, which is only possible in case of a coexisting large OT and a symptomatic OCD with matching characteristics. There is a minor complication risk when harvesting the OT and graft failure of the OT may occur. Although this technique has the advantage of using an autograft with hyaline cartilage, there is a mismatch in cartilage thickness and curvature of the transferred subtalar cartilage and the talus. Lastly, a nonunion or malunion of the medial osteotomy may occur.
Conclusion
In case of the presence of a large OT, a symptomatic cystic talar OCD can be treated with debridement and OT transfer. This individualized surgical technique showed excellent clinical and radiographic results.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241241324 – Supplemental material for Os Trigonum Transfer in a Large Cystic Osteochondral Talar Defect
Supplemental material, sj-pdf-1-fao-10.1177_24730114241241324 for Os Trigonum Transfer in a Large Cystic Osteochondral Talar Defect by Riff Ekelschot, Joost C. Peerbooms and Mikel L. Reilingh in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.