
Abstract
Background:
Recent literature has identified that patient resilience may affect outcomes after meniscectomy. Research into psychological risk factors for poor surgical outcomes has been a focus in orthopaedic surgery.
Purpose/Hypothesis:
The purpose of this study was to examine the relationship between preoperative patient resilience and 2-year postoperative outcomes after arthroscopic meniscectomy. It was hypothesized that there would be no relationship between resilience and patient-reported outcomes after meniscectomy.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Patients who underwent meniscectomy between January and June 2020 at a single multicenter institution were identified, and those aged ≥18 years without evidence of significant osteoarthritis who completed the brief resilience scale (BRS) preoperatively were considered for inclusion. Included patients completed the International Knee Documentation Committee (IKDC), Knee injury and Osteoarthritis Outcome Score for Joint Replacement (KOOS-JR), Single Assessment Numeric Evaluation (SANE), and visual analog scale (VAS) for pain at a minimum of 2 years postoperatively. Based on BRS scores, patients were stratified into low resilience (LR), normal resilience (NR), and high resilience (HR) groups, and differences and changes in outcomes were compared among the groups using the analysis of variance or the Kruskal-Wallis test for continuous data and the chi-square test for categorical data.
Results:
Overall, 100 patients were included (LR group, n = 17; NR group, n = 65; HR group, n = 18). Patients with higher preoperative resilience had higher preoperative IKDC (P = .004) and KOOS-JR (P = .003) scores. However, resilience was not a fixed construct: The median BRS increased in the LR group and decreased in the HR group from pre- to postoperatively (+0.17 and –0.58, respectively; P = .001). At the 2-year follow-up, there was no difference in patient-reported outcome scores across resilience groups, nor was there a difference in the change in IKDC or KOOS-JR scores. Although a positive correlation was observed between preoperative resilience and preoperative IKDC (rS = 0.331) and KOOS-JR (rS = 0.334) scores, preoperative resilience did not correlate with postoperative or 2-year improvements in IKDC or KOOS-JR scores. A weak positive correlation was observed between postoperative resilience and postoperative IKDC (rS = 0.229) and SANE (rS = 0.202) scores, and a weak negative correlation was observed between postoperative resilience and VAS pain scores (rS = ∓0.256).
Conclusion:
Our study indicated that preoperative patient resilience was not predictive of functional outcome scores at a 2-year follow-up after arthroscopic meniscectomy.
Research into psychological risk factors for poor surgical outcomes has been a focus of recent literature. Previous studies have found that anxiety and stress negatively impact recovery by portending a slower and more painful convalescence with inferior long-term outcomes.2,7,11 Another psychological factor that has been the focus of extensive research across various surgical fields is resilience or a person's ability to bounce back from and recover from stress.9,11 Although there is no universally accepted method of assessing resilience, the brief resilience scale (BRS) has been used in the setting of orthopaedic procedures such as total shoulder arthroplasty, total knee arthroplasty (TKA), spinal fusion, and anterior cruciate ligament reconstruction (ACLR).4-6,11,12-14
Many of these studies have demonstrated significant relationships between patient resilience and patient-reported outcomes (PROs) during the postoperative period. However, Chavez et al 3 examined the relationship between resilience and ultrashort-term follow-ups after meniscectomy and found no significant differences in the visual analog scale (VAS) for pain, Knee injury and Osteoarthritis Outcome Score (KOOS), single assessment numeric evaluation (SANE), satisfaction, or opioid use at 3- and 6-month postoperatively between patients stratified into low resilience (LR), normal resilience (NR), and high resilience (HR) groups.
This study aimed to study the relationship between preoperative patient resilience and 2-year postoperative outcomes after arthroscopic meniscectomy. We hypothesized that there would be no relationship between resilience and postoperative PRO scores.
Methods
Inclusion/Exclusion Criteria
This prospective cohort study was approved by our institutional review board before the onset of data collection. All patients who underwent meniscectomy (Current Procedural Terminology codes 29880 and 29881) at a single multicenter institution between January and June 2020 were identified. Patients ≥18 years who completed the BRS through our standard-of-care PRO system were considered for inclusion. Additionally, patients were included in the final analysis only if they also completed the BRS at the 2-year follow-up. Patients were excluded if they (1) were <18 years old at the time of surgery, (2) had undergone revision meniscectomy surgery, (3) had undergone meniscal repair surgery, (4) had undergone concomitant procedures at the time of surgery, and (5) had significant arthritis as defined by a Kellgren-Lawrence (K-L) grade of 3 or 4 at the time of surgery.
We conducted a prior power analysis using a medium effect size of 0.30, an alpha of .05, and a beta of 80% and determined that a sample size of 81 patients would be sufficient to achieve adequate power. This study was able to achieve power by including 100 patients in the final analysis. The included patients were stratified into 3 groups according to their preoperative BRS scores: those with resilience scores of <1 standard deviation from the mean were considered as having LR (n = 17), those with scores within 1 standard deviation of the mean were considered as having NR (n = 65), and those with scores >1 standard deviation from the mean were considered as having HR (n = 18). 14 Figure 1 shows the patient-inclusion process.
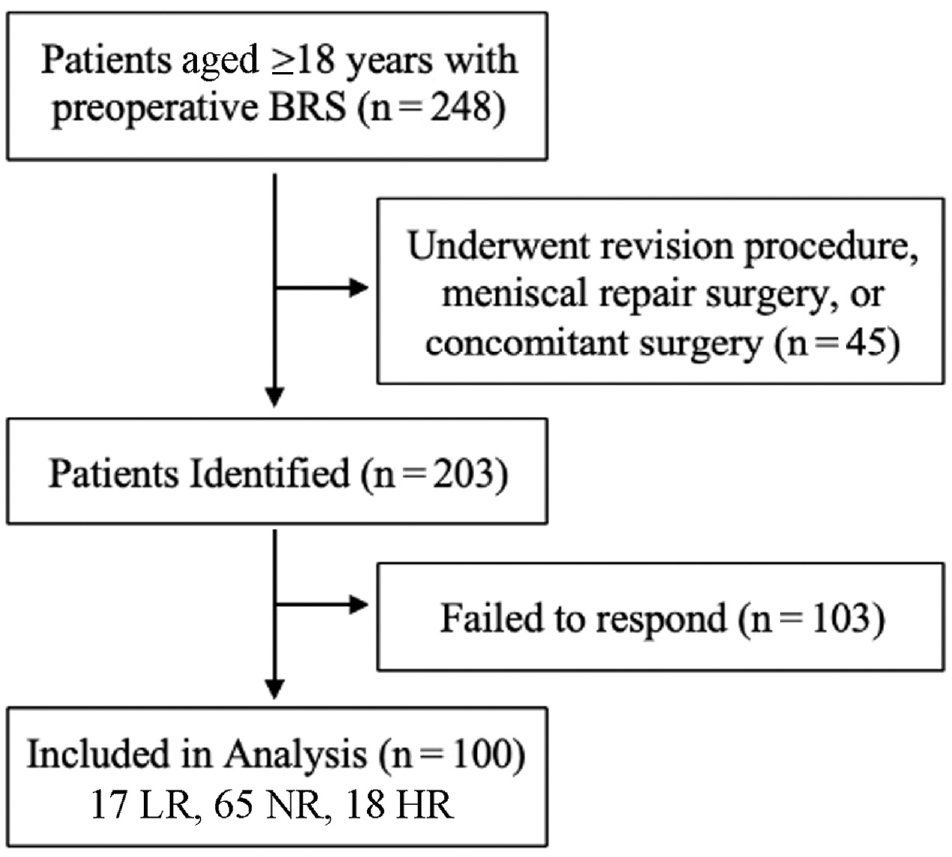
Flowchart of patient inclusion. BRS, brief resilience scale; LR, low resilience; NR, normal resilience; HR, high resilience.
Data Collection
The Outcome Based Electronic Research Database was screened for identified meniscectomy patients to further identify those who completed the BRS before surgery. Preoperative IKDC and KOOS for Joint Replacement (KOOS-JR) survey responses collected through standard-of-care surveys were also queried. A chart review for included and eligible patients was conducted to confirm the level of osteoarthritis (K-L grade) as well as to collect demographic information (sex, race, preinjury level of competition, site of the tear, and alcohol/tobacco/recreational drug use) and medical history. During data collection, self-reported mental health conditions—including anxiety and depression—were recorded from patient electronic medical records to exclude these patients as part of a subanalysis. Two-year follow-up scores—including BRS, IKDC, KOOS-JR, VAS pain, and SANE—for the operative and contralateral knee were collected via REDCap (Vanderbilt University). Preoperative IKDC scores were available for 99 patients (99%) and preoperative KOOS-JR scores were available for 98 patients (98%).
Using previously published cutoff values, 1 we calculated the rates that patients achieved the minimal clinically important difference (MCID), substantial clinical benefit (SCB), and Patient Acceptable Symptom State (PASS) for the IKDC (MCID: 10.6 points, SCB: 25.3 points, PASS: 57.9) and the KOOS-JR (MCID: 10.7 points, SCB: 13.2 points, PASS: 68.3).
Statistical Analysis
Descriptive statistics were reported as means with standard deviations for normal distributions, medians with interquartile ranges for non-normal distributions, or frequencies with percentages. Comparisons of continuous data were performed using the analysis of variance or Kruskal-Wallis tests depending on normality, and comparisons of categorical data were performed using chi-square tests. PRO scores were compared between the LR, NR, and HR groups using the Kruskal-Wallis test. Correlation analysis (Spearman r) was performed to understand the relationship between preoperative resilience and postoperative PRO scores as well as between postoperative resilience (based on 2-year follow-up BRS scores) and postoperative PRO scores. A similar subgroup analysis was also performed after excluding patients who self-reported experiencing anxiety or depression. For all analyses, P < .05 was deemed significant. All statistical analyses were performed using R studio Version 3.6.3.
Results
All Meniscectomy Patients
Patients in the LR, NR, and HR groups did not differ significantly in age, body mass index (BMI), race, K-L grade of osteoarthritis, smoking habits, alcohol use, recreational drug use, or history of psychiatric comorbidity (defined as a history of anxiety or depression). The groups differed significantly in the proportion of female patients (41.2%, 44.6%, and 5.56% for LR, NR, and HR groups, respectively; P = .009) and the side affected (right side: 76.5%, 47.7%, 22.2% for LR, NR, and HR groups, respectively, P = .006) (Table 1).
Comparison of Demographic Characteristics According to Preoperative Resilience Group a

Data are presented as mean ± SD or n (%). Bold P values indicate statistically significant differences between groups (P < .05). BMI, body mass index; HR, high resilience; K-L, Kellgren Lawrence; LR, low resilience; NR, normal resilience; OA, osteoarthritis.
Resilience was found to be fluid—median BRS scores significantly changed from the preoperative to the 2-year follow-up in the LR, NR, and HR groups (+0.17 vs 0 vs −0.58, respectively; P = .001) (Table 2).
Changes in Resilience According to the Preoperative Resilience Group a
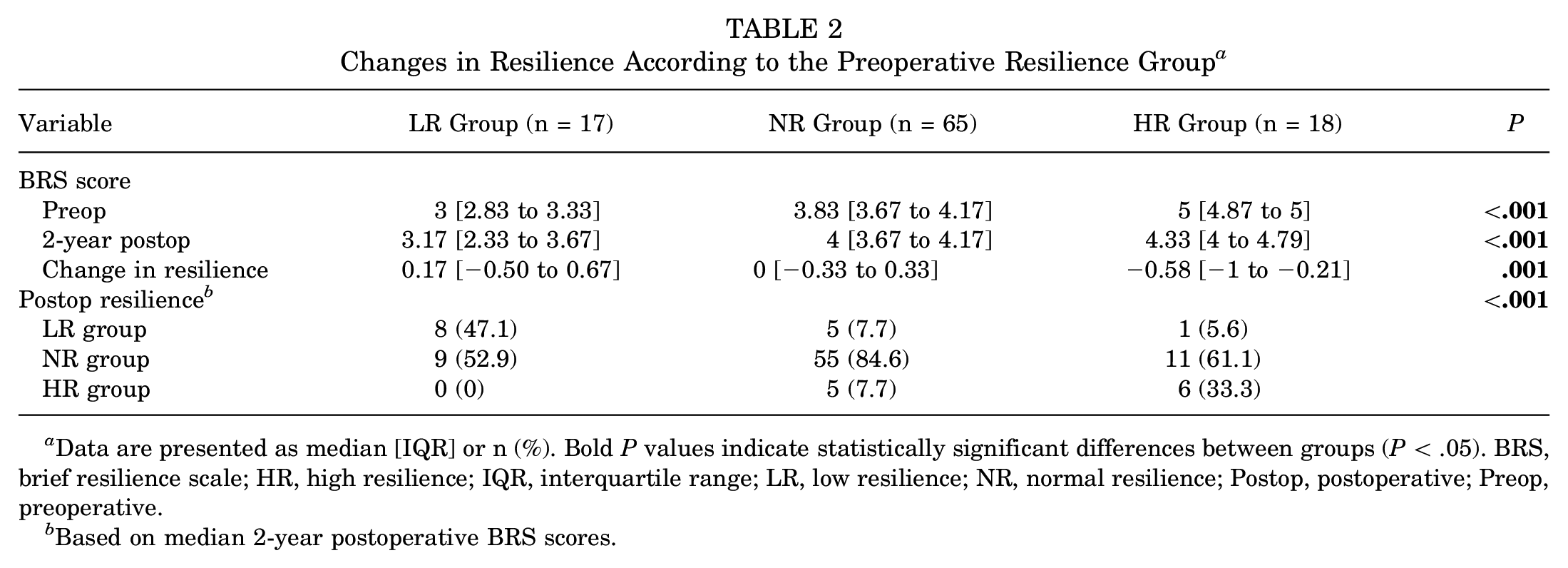
Data are presented as median [IQR] or n (%). Bold P values indicate statistically significant differences between groups (P < .05). BRS, brief resilience scale; HR, high resilience; IQR, interquartile range; LR, low resilience; NR, normal resilience; Postop, postoperative; Preop, preoperative.
Based on median 2-year postoperative BRS scores.
Median preoperative IKDC (LR: 30.8 vs NR: 41.4 vs HR: 54.3; P = .004) and KOOS-JR scores (LR: 44.9 vs NR: 54.8 vs HR: 62.7; P = .003) were significantly different between the resilience groups (Table 3). However, no differences were observed in the median postoperative IKDC, KOOS-JR, VAS pain, or SANE scores at the 2-year follow-up.
Pre- and Postoperative PRO Scores According to the Preoperative Resilience Group a
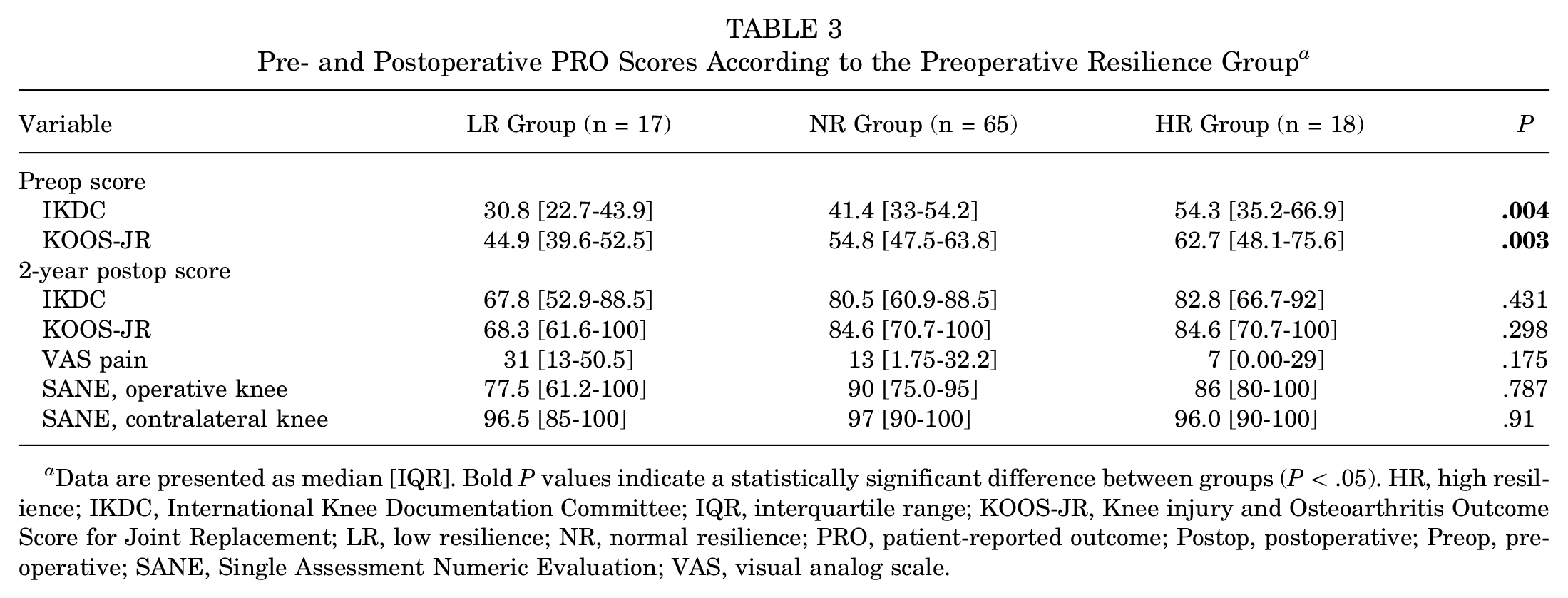
Data are presented as median [IQR]. Bold P values indicate a statistically significant difference between groups (P < .05). HR, high resilience; IKDC, International Knee Documentation Committee; IQR, interquartile range; KOOS-JR, Knee injury and Osteoarthritis Outcome Score for Joint Replacement; LR, low resilience; NR, normal resilience; PRO, patient-reported outcome; Postop, postoperative; Preop, preoperative; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
Although there was no difference in the proportion of patients who met the MCID or SCB for the KOOS-JR, the LR group met the KOOS-JR PASS less frequently versus the NR and HR groups (38.5% vs 75.4% and 76.5%, respectively; P = .036) (Table 4). No difference was found in the proportion of patients who met the MCID, SCB, or PASS for the IKDC.
Patients Who Met the MCID, SCB, and PASS for the IKDC and KOOS-JR According to the Preoperative Resilience Group a
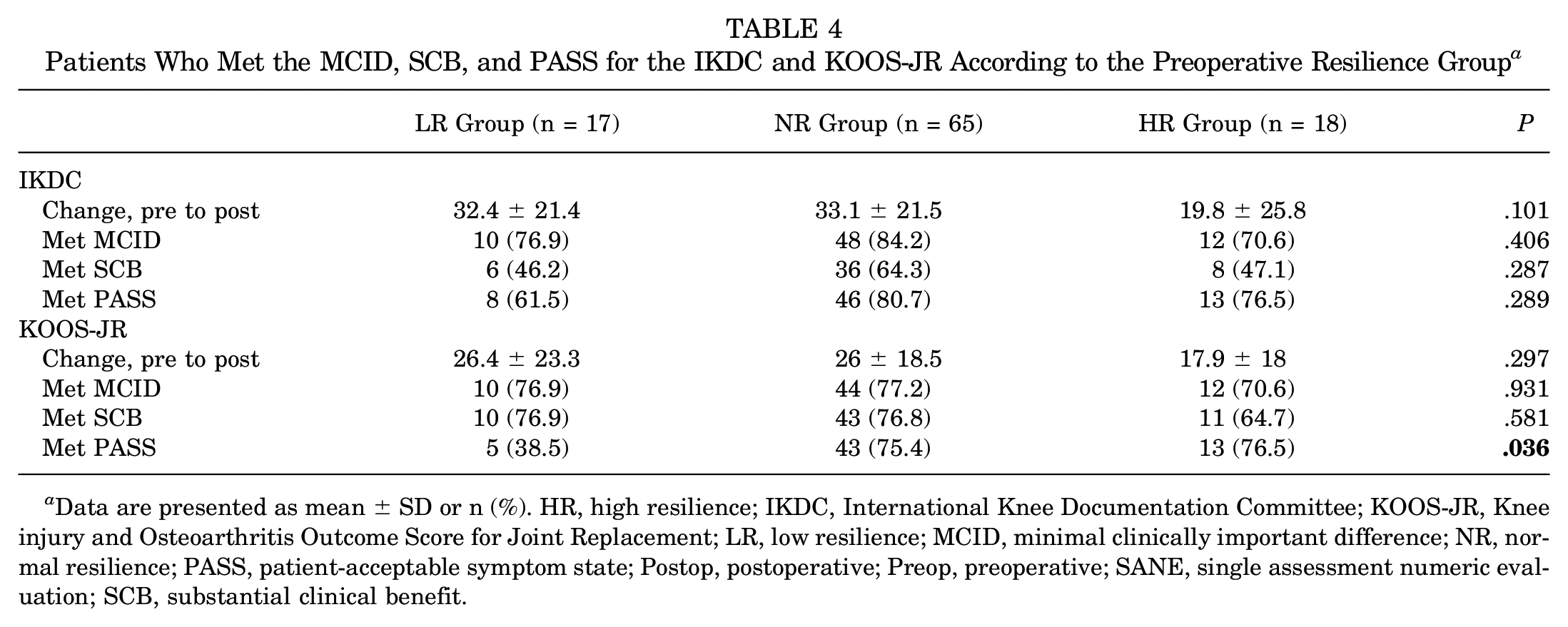
Data are presented as mean ± SD or n (%). HR, high resilience; IKDC, International Knee Documentation Committee; KOOS-JR, Knee injury and Osteoarthritis Outcome Score for Joint Replacement; LR, low resilience; MCID, minimal clinically important difference; NR, normal resilience; PASS, patient-acceptable symptom state; Postop, postoperative; Preop, preoperative; SANE, single assessment numeric evaluation; SCB, substantial clinical benefit.
Correlation analysis was also performed. Although there was a weak positive correlation between preoperative resilience and preoperative IKDC (rS = 0.331) and KOOS-JR scores (rS = 0.334), preoperative resilience did not correlate with any postoperative PRO. Similarly, it did not correlate with the changes in IKDC or KOOS-JR scores over time. However, resilience did change over time, and there was a weak positive correlation between postoperative resilience and postoperative IKDC (rS = 0.229) and SANE (rS = 0.202) scores, and there was a weak negative correlation with postoperative VAS pain scores (rS = −0.256). No relationship was observed between postoperative resilience and postoperative KOOS-JR scores, changes in IKDC scores, or changes in KOOS-JR scores.
Subanalysis of Patients Without History of Anxiety or Depression
In the subgroup analysis of patients with no medical history of anxiety and/or depression, no significant differences were found in sex, age, race; BMI; K-L grade; or site of tears between groups. Preoperative KOOS-JR scores improved postoperatively across groups (LR: 47.5 vs NR: 58.1 vs HR: 63.1; P = .016). However, the NR and HR groups met the KOOS-JR PASS at higher rates than the LR group (P = .009) (Table 5).
Resilience and PROs for Patients When Excluding Those With a Medical History of Anxiety and/or Depression a

Data are presented as median [IQR], n (%), or mean ± SD. Bold P values indicate a statistically significant difference between groups (P < .05). BRS, brief resilience scale; HR, high resilience; IKDC, International Knee Documentation Committee; IQR, interquartile range; KOOS-JR, Knee injury and Osteoarthritis Outcome Score for Joint Replacement; LR, low resilience; MCID, minimal clinically important difference; NR, normal resilience; PASS, Patient Acceptable Symptom State; Postop, postoperative; PROs, patient-reported outcomes; Preop, preoperative; SCB, substantial clinical benefit.
Based on median 2-year postoperative BRS scores.
Additional Procedures
Overall, 3 patients (2 in the LR cohort and 1 in the NR cohort) underwent subsequent procedures. One patient in the LR group and 1 patient in the NR group underwent TKA procedures; the patient in the LR group had a TKA within 6 months of the initial meniscectomy for continued pain and progressive osteoarthritis from an osteochondral defect, while the patient in the NR group had a TKA 15 months after the initial surgery. An additional member of the LR group underwent an arthroscopic synovectomy within 5 months of the initial procedure for continued pain and discomfort.
Discussion
The primary finding of this study was that preoperative resilience as measured by the BRS was not predictive of patient outcomes at 2 years after meniscectomy. Although lower preoperative BRS scores were associated with lower preoperative IKDC and KOOS-JR scores (difference between LR, NR, and HR groups, P = .004 and P = .003, respectively), no significant difference was found between the groups in postoperative IKDC or KOOS-JR scores (P = .431 and P = .298, respectively). Similarly, preoperative resilience did not significantly correlate with pre- to postoperative changes in IKDC or KOOS-JR scores (P = .101 and P = .297, respectively).
The current literature on the relationship between preoperative BRS scores and outcome scores is mixed. Magaldi et al 6 studied a cohort of 153 patients with TKA (mean age, 68.2 years; 52% women): At 3- and 12-month follow-ups, they found that high preoperative resilience was associated with greater physical and mental health outcomes as measured by the Patient-Reported Outcomes Measurement Information System but not with the KOOS-JR. However, Nwankwo et al 8 studied a similar cohort of 117 patients with TKA (mean age, 67 years; 53% women) and found that higher preoperative BRS scores were associated with better postoperative knee function and general physical health, but not general mental health, at a 3-month follow-up. Similar to our study, Chavez et al 3 examined 132 patients who underwent meniscectomy (mean age 48 years, 59% women) and found no correlation between preoperative resilience and postoperative PROs at 3 and 6 months postoperatively. Our study evaluated 100 patients (mean age 52.5 years; 37% women) and found no significant correlations between preoperative resilience and PROs 2 years after surgery.
There are several possible reasons for the heterogeneity of these results. First, the studies of TKA patients by Magaldi et al 6 and Nwankwo et al, 8 which both found an association between resilience and outcomes, followed older, lower-demand patient populations (mean age 68.2 and 67 years, respectively), compared with the cohorts of the study by Chavez et al 3 and our study (48 and 52.5 years, respectively), which found no correlation. This may indicate some associations between the impact of resilience and age or physiologic demand or may be secondary to the disparate nature of the surgeries themselves (TKA vs meniscectomy). Magaldi et al 6 and Nwankwo et al 8 also had a notable difference in their findings, with the former indicating an association between resilience and general health (mental and physical) but not knee-specific outcomes, while the latter study found an association between resilience and general physical health and knee outcomes but not general mental health. This suggests that there are varying degrees to which specific PRO measures may be sensitive to resilience as measured by the BRS. 3
In assessing BRS scores both preoperatively and at a 2-year follow-up, we were able to establish that resilience is dynamic and changes over time. Howerver, there is a paucity of information on the fluidity of BRS scores over time, and it is difficult to elucidate the timeline by which these changes occur. This, along with the heterogeneous associations with different PRO measures in the literature, suggests that the BRS may be an imperfect tool for assessing resilience. However, we did find that when assessed concurrently, BRS scores did significantly correlate with IKDC and KOOS-JR scores—preoperative BRS scores were associated with preoperative IKDC and KOOS-JR scores, and 2-year BRS scores were associated with 2-year IKDC and KOOS-JR scores. This suggests that although resilience measured in the preoperative period may not be a clinically useful predictive measurement, assessing resilience in real time may be useful in determining concurrent functional status.
Although demographic differences may also contribute to differences in resilience, specific demographic risk factors remain poorly defined. In the present study, a significant difference was found in the ratio of female patients across groups, and the HR group had the lowest composition of female patients (HR group: 5.56%; NR group: 44.6%; LR group: 41.2%). However, Chavez et al 3 did not find a significant difference in the sex distribution across study groups. Furthermore, Zhang et al 14 evaluated patients after ACLR and found that the low resilience group had the smallest percentage of women (HR group: 41.7%; NR group: 54.3%; LR group: 22.2%). Further research is necessary to elucidate the relationship between resilience, sex, and patient outcomes.
Finally, we found that patients in all 3 study groups met the MCID, SCB, and PASS thresholds for IKDC scores and the MCID and SCB thresholds for KOOS-JR scores at similar rates. However, patients in the LR group met the KOOS-JR PASS significantly less frequently than the NR and HR groups. The reason and clinical significance for this are unclear, especially since there was no difference in postoperative KOOS-JR scores or 2-year perioperative KOOS-JR improvements across groups.
Limitations
This study is not without its limitations. First, the response rate for this study was 49.3% (100/203), introducing nonresponse bias to the study. Although our study had a 2-year minimum of patient follow-up data, the coronavirus 2019 pandemic was concurrent with this period. This may have deterred patients from responding to our study, introduced selection bias by including patients willing to have surgery during this time, and in a similar manner may have skewed resilience scores by including this patient population. It would be interesting to assess the same variables in a different period and compare the findings to the present analysis. Confounding factors—such as patient socioeconomic status—could not be accounted for, introducing another source of potential bias. This, however, is difficult to ascertain and control for in any study. A subanalysis of patients without a medical history of anxiety and/or depression was included to examine the cohort without some of the potential influencing factors other studies have explored. Although the study is properly powered, the demographic characteristics of included patients are not accurately representative of the US population (37% female cohort in this study vs 50%, 82% White vs 75% across the United States), which may limit the generalizability of the study. 10 Finally, despite typically being used to evaluate patients who underwent TKA, the 7-question KOOS-JR was used for this study, as it was more convenient for patients to complete. Future iterations of this study should attempt to take these limitations into account through their design. Additionally, exploration or development of varying other means for evaluating resilience beyond the BRS can benefit our overall understanding of the subject.
Conclusion
Preoperative patient resilience was not predictive of functional outcome scores at a 2-year follow-up after arthroscopic meniscectomy.
Footnotes
Final revision submitted April 9, 2024; accepted May 2, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.W.C. has received education payments from Smith+Nephew, Paladin Technology Solutions, and Gotham Surgical. F.P.T. has received consulting fees from DePuy/Medical Device Business Services; royalties from Tigon Medical; hospitality payments from MicroVention and Stryker; and has stock/stock options in Trice Medical. K.B.F. has received grant support from Vericel; education payments from Liberty Surgical; consulting fees from DePuy/Medical Device Business Services, Vericel, and Innocoll; nonconsulting fees from Vericel; and honoraria from Vericel. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Philadelphia University/Thomas Jefferson University (ref No. 19E.940).