
Abstract
Purpose:
This study was designed to compare the clinical outcomes of meniscectomy versus repair and to study the effects of (1) duration of follow-up and (2) concomitant anterior cruciate ligament (ACL) reconstruction on clinical outcomes.
Methods:
A retrospective study was conducted, involving 112 knees of 106 patients who underwent meniscus surgery, either partial meniscectomy or meniscal repair between 2008 and 2016. There were 42 meniscectomies and 70 meniscal repairs. Patients were graded pre- and post-operatively using the International Knee Documentation Committee (IKDC) score and Tegner Activity Level Scale through case notes review. Statistical analysis was done using the paired Student’s t-test (two-tailed) or Wilcoxon signed-rank test for paired scores. The two-sample Student’s t-test (two-tailed) or Mann–Whitney U test was used for independent scores. Multiple variable linear regression analysis was used to assess the importance of the variables on outcomes. A statistical significance is taken as p < 0.05.
Results:
Meniscectomy and repair had good outcomes. IKDC scores improved from 46.6 to 81.7 after meniscectomy and from 45.9 to 84.4 after repair (p < 0.001). Meniscectomy fared worse in late follow-up (>18 months), decreasing from 88.2 in early follow-up (≤18 months) to 72.1 (p < 0.05). The post-operative scores in meniscal repair were maintained in the late follow-up group (82.9 compared to 87.1, p > 0.05). Concomitant ACL reconstruction improved the outcomes of meniscectomy (IKDC and Tegner: p < 0.05) and repair (IKDC and Tegner: p < 0.05).
Conclusion:
Both meniscectomy and meniscal repair are viable surgical techniques for meniscal injury and have good outcomes. Meniscal repair has a better prognosis in the long run.
Introduction
The meniscus plays a crucial role, functioning as a shock absorber, 1 a load distributer to minimize excessive contact pressure 2 and a secondary stabilizer of the knee, limiting excess motion 3 particularly in anterior cruciate ligament (ACL)-deficient knees. 4
Unfortunately, the meniscus is prone to injury and has poor healing rates as it is an intra-articular structure with relative avascularity. 5 The surgical management of meniscal tears has seen an increasing trend towards meniscal repair from partial meniscectomy 6 because of recognition of the role the meniscus plays in cartilage longevity.
Despite this, partial meniscectomy remains popular as an initial form of management, because it may provide better symptomatic resolution at least in the short term. 7 Other possible advantages of partial meniscectomy include being technically easier and requiring less operating time. Many studies thus far have looked at the radiologic outcomes of meniscectomy compared to repair, with a consistent reporting of increased osteoarthritic changes in the meniscectomy group compared to those who underwent meniscal repair. 8 –10 However, while there have been studies done comparing the clinical outcomes of meniscectomy and repair, 10 –14 the results so far have not been fully conclusive.
To provide a holistic view, factors which affect the comparative outcomes between the two surgical techniques should be explored. Since osteoarthritis develops over time, the duration post-operation is a critical factor which should be considered. Also, meniscal injuries are often accompanied by cruciate ligament injuries, especially the ACL. As a result, ACL reconstruction surgery is often done in the same setting as meniscal surgery. However, few studies have examined the effect of the aforementioned factors (period of follow-up and presence of concomitant ACL reconstruction) on the comparative clinical outcomes of meniscectomy versus repair thus far.
This study seeks to compare the clinical outcomes of partial meniscectomy and meniscal repair and elucidates the factors that may influence outcome. We hypothesize that the outcome of meniscus repair may be worse in the early stages of post-operation, but will eventually surpass that of meniscectomy in the long term.
Methodology
A retrospective review was conducted. Potential patients at a single large tertiary hospital in Singapore who underwent either partial meniscectomy or meniscal repair (with or without ACL injury and reconstruction) between 2008 and 2016 by a single surgeon were considered for inclusion in the study.
The following patient groups were excluded: (1) previous meniscal surgery done prior to current meniscal surgery, (2) concomitant ACL injury without undergoing simultaneous ACL reconstruction (patients with ACL-deficient knees), (3) posterior cruciate ligament injury and (4) underwent meniscal transplant.
The choice of surgery between meniscectomy and repair was not randomized and was based on the suitability of repair depending mainly on the blood supply and the state of the meniscus. Repair was done if the tear was in a zone with good vascularity (e.g. red-red zone) and if the edges of the meniscus were sufficiently intact to pass sutures through. Arthroscopy was done through standard arthroscopic portals (anteromedial and anterolateral). Meniscectomy was done by shaving the frayed portion of the meniscus (Figure 1). Meniscal repairs were performed using the outside-in technique for anterior horn tears and all-inside technique for body and posterior horn tears with the use of OMNISPANTM (DePuy Synthes, Singapore) or FasT-FixTM (Smith & Nephew, Singapore) suture anchors (Figure 2). Standard ACL reconstruction was carried out using semitendinous and gracilis grafts, with graft aperture fixation done with Milargo® interference screws. Post-operatively, patients were placed on non-weightbearing status for 2 weeks initially followed by partial weightbearing for 6–8 weeks.

Meniscectomy.

Meniscal repair.
Patient demographics such as age, gender, body mass index, duration between injury and operation, duration post-surgery (calculated from the time of operation to the time the post-operative scores were taken), location and type of meniscal tears, type of chondral lesions and chondral surgery performed were obtained from medical records.
To study the effect of length of duration post-surgery on the clinical outcomes of meniscectomy versus repair, patients were classified into two groups: early and late follow-up, depending on the time since surgery. Due to the relatively short duration of follow-up for patients undergoing meniscal surgery in this hospital, the early follow-up group comprised patients who underwent meniscal surgery from 2014 to 2016 (follow-up duration of 18 months or less from time of data collection), and the late follow-up group comprised patients who underwent meniscal surgery prior to 2014 (follow-up duration of more than 18 months).
Pre-operative and post-operative gradings were done retrospectively using the established subjective International Knee Documentation Committee (IKDC) knee evaluation form and Tegner Activity Level Scale (Tegner score). The IKDC is a scoring system that documents the patient’s symptoms and function 15 and is often used together with the Tegner score which is a reliable measure of outcomes of arthroscopic knee surgery, evaluating performance and activity levels before and after surgery. 16 The IKDC and Tegner scores were obtained based on the latest follow-up history from clinical case records in December 2016.
Data analysis was performed using R 3.3.2 (R Core Team 2016, R Foundation for Statistical Computing, Vienna, Austria). The two-sample Student’s t-test (two-tailed) and χ 2 test were used to compare the demographics and characteristics between the patients in the meniscectomy group and meniscal repair group. To compare the paired pre-operative versus post-operative scores for each surgical technique, the paired Student’s t-test (two-tailed) was used for the IKDC scores, while the Wilcoxon signed-rank test was used to analyse the Tegner score. The post-operative IKDC results of partial meniscectomy versus meniscal repair were compared using two-sample Student’s t-test (two-tailed) while that of the Tegner scores were compared using the Mann–Whitney U test. Finally, multiple variable linear regression analysis was done to determine the correlation between the variables (age, time from operation, severity of chondral injuries and concomitant ACL reconstruction) and the outcomes of meniscal repair and meniscectomy. A statistical significance is taken as p < 0.05.
The study had Institutional Ethics Review Board approval.
Results
In total, there were 42 meniscectomies and 70 meniscal repairs. Patient demographics and clinical characteristics were similar between the meniscal repair and meniscectomy groups (Table 1) including types of meniscal tears and chondral injuries, except that the meniscal repair group had a slightly higher proportion of isolated meniscus injury compared to the meniscectomy group. The mean age is 41.1 years old (range 19–72) for meniscectomy and 42.2 years old (range 17–76) for repair. For meniscectomy, the mean duration post-surgery is 27.6 months (range 1.0–91.0), while that of repair is 19.4 months (range 0.5–76.0).
Patient demographics and clinical characteristics.

IKDC: International Knee Documentation Committee; BMI: body mass index; ACL: anterior cruciate ligament.
a X 2 test.
Both meniscectomy and repair showed significant improvement in post-operative clinical outcomes compared to pre-operation (Figures 3 and 4). For meniscectomy, mean IKDC scores showed an increase from 46.6 to 81.7 (p < 0.001), while the mean Tegner scores improved from 3.0 to 5.0 (p < 0.001; Table 2). In patients who underwent meniscal repair, the mean IKDC score rose from 45.9 to 84.4 (p < 0.001) and the mean Tegner score improved from 2.6 to 4.8 (p < 0.001).

Average IKDC scores of meniscectomy and meniscal repair. IKDC: International Knee Documentation Committee.

Average Tegner scores of mesnicectomy and meniscal repair.
Overall results of meniscectomy and repair.a
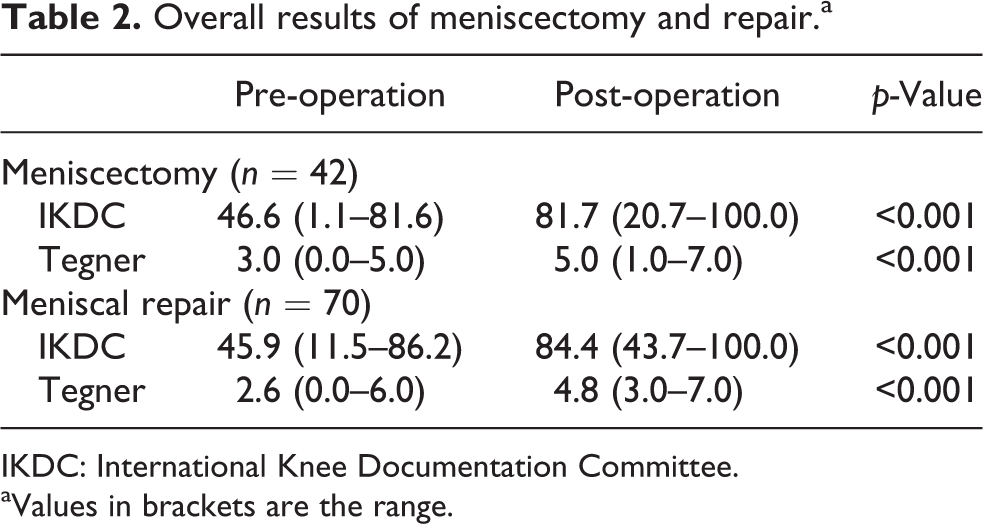
IKDC: International Knee Documentation Committee.
aValues in brackets are the range.
Comparing the early follow-up groups of meniscectomy and meniscal repair, we observed that meniscectomy performed slightly better than repair for both IKDC (88.2 vs. 82.9; p = 0.18) and Tegner scores (5.4 vs. 4.7; p < 0.05; Table 3). However, in the late follow-up groups, the IKDC score of meniscal repair was significantly better than those of meniscectomy (87.1 vs. 72.1, p < 0.05). Tegner scores also showed better outcomes with meniscal repair than meniscectomy (5.0 vs. 4.4, p = 0.23).
Effect of duration of follow-up on clinical outcomes of meniscectomy and repair.a

IKDC: International Knee Documentation Committee.
aValues in brackets are the range.
The changes in scores over time within each type of surgical management were also analysed. While the scores of meniscectomy were observed to decline between early and late follow-up (IKDC: 88.2 to 72.1, p < 0.05; Tegner: 5.4 to 4.4, p = 0.06; Table 3), the scores of meniscal repair tend to remain relatively stable, with no significant difference in the IKDC score (82.9 to 87.1, p = 0.25) and Tegner score (4.7 to 4.9, p = 0.17) between early and late follow-up groups.
We observed that within each surgical management, those who had concomitant ACL reconstruction consistently did better than those who had surgery for isolated meniscal injury for both the IKDC score (meniscectomy: p < 0.001; repair: p = 0.03) and Tegner score (meniscectomy: p < 0.001; repair: p < 0.001; Table 4). On the other hand, the presence or absence of concomitant ACL reconstruction did not seem to have a significant effect on the comparative clinical outcomes between the meniscectomy and meniscal repair groups.
Effect of concomitant ACL reconstruction on clinical outcomes of meniscectomy and repair.a

IKDC: International Knee Documentation Committee; ACL: anterior cruciate ligament.
aValues in brackets are the range.
Based on regression analysis for duration of follow-up, our data demonstrated that, in the meniscectomy group, for every month of follow-up, the IKDC score decreased by 0.3 points (p < 0.05) and the Tegner score fell by 0.02 points (p < 0.05). On the other hand, duration of follow-up was not significantly correlated with the clinical outcomes of meniscal repair. In fact, the Tegner score for meniscal repair increased by 0.01 for every month of follow-up (p < 0.05).
In contrast, the patient’s age had a significant negative correlation to the clinical outcomes of meniscal repair. The IKDC score reduced by 0.3 points for every year of age (p < 0.05) while Tegner scores declined by 0.04 points (p < 0.05). For the meniscectomy group, age of the patient had a significant negative correlation to the Tegner score, with a decrease of 0.04 points for every year of age (p < 0.05).
For both meniscal repair and meniscectomy, time from injury to surgery, concomitant ACL reconstruction and severity of initial chondral lesion did not have a significant correlation to the outcomes.
Discussion
Both types of surgical management, meniscectomy and repair, result in good outcomes compared to the pre-operative state both from the patient’s perspective (IKDC score) and in terms of the patient’s function (Tegner Activity Level Scale). This is consistent with the previous studies done on meniscectomy 17,18 and repair, 19,20 respectively. When the patients from each surgical management were divided into early (≤18 months) and late (>18 months) follow-up groups, we observed that meniscectomy had better symptom relief than meniscal repair in the early stages, which was also supported by the previous studies. 7 We hypothesize that this is because meniscectomy removes the pathology immediately by excision of the tear, whereas repair requires time for healing of the approximated torn meniscal edges, during which symptoms persist.
As mentioned earlier, studies which report differences in the clinical outcomes of meniscectomy versus repair have shown differing results. Shelbourne and colleagues reported no significant difference in outcomes (IKDC score) between meniscectomy and repair in the management of bucket-handle tears in both medial and lateral meniscus. 12,13 On the other hand, Xu and Zhao reported the converse – a meta-analysis of seven studies showed that meniscal repair did indeed have better outcomes (Lysholm, Tegner). 14
The key finding of this study is that the results of meniscal repair withstood the test of time, showing better long-term scores compared to meniscectomy. Patients who underwent meniscectomy had a decrease in subjective score and function when comparing the early and late follow-up groups. Conversely, no significant difference was found between the early and late follow-up groups in meniscal repair. This is supported by regression analysis which showed that among the variables being studied, the duration of follow-up was the most important negative correlator for the meniscectomy group, while such a relationship was not evident in the repair group, indicating that the outcomes remained stable over time.
These findings are in keeping with previous studies on the radiological outcomes of meniscectomy versus repair. 8 –10 Patients who underwent meniscectomy were reported to have greater osteoarthritic changes at long-term follow-up, due to the loss of the load distributing function of the meniscus. This resulted in focal chondral damage and propagation of existing chondral injury. 21 While the comparison between early and late follow-up groups for each surgical technique was not longitudinal, key variables affecting outcomes such as the patients’ demographics and surgical technique were kept similar. Therefore, the deterioration of outcomes between the early and late follow-up groups of meniscectomies is highly probable.
Another interesting finding of this study was that there was no significant difference in comparative outcomes between meniscectomy and meniscal repair regardless of the presence of concomitant ACL reconstruction. There are few studies thus far, if any, which look at whether having concomitant ACL reconstruction affects the comparative outcomes of meniscectomy and meniscal repair.
Conversely, we observed that for both meniscectomy and repair, the presence of ACL reconstruction was correlated with a better clinical outcome. Other authors have reported similar results – repairs done in knees with concomitant ACL reconstruction tend to heal better than those done in ACL-stable knees. 22,23 The theorized mechanism is the release of cytokines during drilling of bone tunnels and the fibrin clots, both of which aid in meniscal healing.
Overall, our results show that while both meniscectomy and repair are viable surgical management for meniscal injury, repair tends to outperform meniscectomy eventually. Unfortunately, not all meniscal injuries are amenable to repair. Therefore, in the interests of patients’ long-term function, we believe that meniscal repair should be the first-line management whenever possible since it preserves the original structure and function of the knee.
This is a retrospective study; therefore, there is the element of selection bias, as patients were not randomized to either arm of the study. This is mitigated to some extent as both groups (meniscectomy and meniscal repair) show minimal difference in demographics and characteristics of meniscal and chondral injuries. Another limitation is that the patients in this study were not randomized to either arm of treatment. Further studies may be conducted as blinded randomized controlled trials to better compare the clinical outcomes of meniscectomy versus repair.
Conclusion
In conclusion, while meniscectomy has been the mainstay of treating meniscal injury, the advent of meniscal repair has seen a decrease in use of meniscectomy due to recognition of long-term adverse effects on knee function. Our results show superior long-term clinical outcomes of repair versus meniscectomy, demonstrating the clinical value of treating meniscal injury with repair when possible. Therefore, save the meniscus!
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.