
Abstract
Background:
Hip arthroscopy (HA) procedures have continued to increase worldwide. However, no data are currently available regarding the increasing HA case volume and trends in Turkey.
Purpose:
To identify trends in postoperative care habits and incidence of HA in Turkey using data from the national Health Coding Reference Server (SKRS) database.
Study Design:
Cross-sectional study.
Methods:
Patients who underwent HA and were recorded in the SKRS database between 2016 and 2023 were identified and retrospectively analyzed. Age, sex, institution type, geographic zone, and number of procedures were determined. The incidence of HA, overall annual case volume, chemoprophylaxis prescriptions, and postoperative care habits were also evaluated. The International Classification of Diseases, 10th Revision codes for femoral neck fracture after the index procedure and total hip arthroplasty conversion rate were analyzed. The authors utilized Poisson regression to determine the ratios of before and after periods in comparison with the same periods. Statistical analysis was performed using the statistical package SPSS software.
Results:
In total, 1580 HA procedures were identified. The mean age of the included patients was 39.2 ± 11.0 years (range, 18-65 years). Throughout the research period, an 833% increase in the number of surgeries was observed, whereas the incidence increased from 0.37 to 2.86 per 100,000 cases (P = .001). A significant annual increase in incidence was noted from 2017, 2018 and 2021 compared with the respective prior year. Moreover, 56.1% of all HA cases were performed in the Marmara region, whereas 47.7% of the cases were treated in private hospitals. Femoral neck fractures were encountered in 2 (0.1%) cases throughout the study duration. Enoxaparin sodium was the most preferred chemoprophylactic drug (99.4%). The 2-year total hip arthroplasty conversion rate was 3.5%.
Conclusion:
This study describes the current trends in HA across Turkey and provides a perspective on physician preferences. Notably, HA procedure counts, the ratio between HA and other orthopaedic procedures, and the incidence of HA demonstrated an increasing trend, with enormous potential for further advancement. These findings highlight the need for the creation of a national registry capable of obtaining more specific and accurate data.
Keywords
Femoroacetabular impingement (FAI) was first introduced in 1999 by Ganz, who described the pathology as an “abundance of bone on the head or head-neck junction of the femur which causes pain and limits flexion.” 42 Since then, the management of FAI has shifted toward arthroscopic surgery after the development of sophisticated surgical equipment and techniques. The concept of precise bony overgrowth removal via minimal invasive techniques has attracted the attention of physicians and has facilitated the rapid development of hip arthroscopy (HA). Moreover, increasing awareness of the arthroscopic treatment of FAI has promoted the use of HA for other pathologies, such as septic arthritis, 49 loose bodies, 41 ligamentum teres injuries, 14 iliopsoas bursitis, labrum repair, and snapping hip syndrome. 27
Mounting evidence has suggested that FAI is a precursor to osteoarthritis (OA).11,13,33,45,46 Resection of FAI aims to alleviate pain and relieve undesired premature contact during movement. Moreover, several studies have shown that the minimally invasive surgical approach offers increased functional scores and high rates of return to previous activity levels with low complication rates in young athletes33,34,38 and decreases the conversion to total hip arthroplasty (THA) in the mid-to-long term. 29 Furthermore, evidence has shown that HA promotes superior functional outcomes compared with nonoperative treatment.15,17,19,39 Additionally, HA is a cost-effective approach to preventing substantial and indirect economic burden caused by FAI while also increasing quality of life scores. 36 However, postoperative care protocols after HA have yet to be established, and heterotopic ossification (HO) and venous thromboembolism (VTE) prophylaxis having been reported as concerns, with complication rates reaching up to 6.94% and 44%, respectively.1,3,4,20,28
Consistent with the burgeoning interest, recent studies have demonstrated an increasing trend in HA numbers by up to 25-fold across the globe.12,13,15 For instance, research has shown a 365% increase in the incidence of HA across the United States,8,35,40 with similar surges having been reported in England, Korea, Finland, and Sweden during the early stages after the adoption of HA in each country.26,32,43,52 To obtain precise insights into future device supply projections and national surgical volume expectations, the accurate collection of nationwide data is crucial. Additionally, evaluating these data provides a comprehensive understanding of the long-term clinical outcomes of the HA, which can further guide clinical decision-making and improve patient care. With the increasing demand for minimally invasive hip preservation techniques in Turkey and the challenging health care economic climate within the country, hospital systems need to adequately prepare the necessary tools and strategies for the safe performance of HA in the Turkish populus. To the best of our knowledge, this is the first study to present national trends in HA on a yearly basis for the Republic of Turkey.
As such, the current study aimed to reveal trends in the incidence and perioperative care habits after HA in Turkey using data from the national Health Coding Reference Server (SKRS) database. We hypothesized that (1) the number of HA procedures in the country has been trending upward and (2) the incidence rates of HA among other orthopaedic surgeries have been increasing.
Methods
This retrospective study was authorized by the Turkish Ministry of Health and was conducted in accordance with the ethical principles stated in the Declaration of Helsinki. Ethics committee approval was obtained from the Turkish Ministry of Health, which waived the need for informed consent given the retrospective nature of this study and the health information privacy law (ID: 95741342-020/27112019). In Turkey, all citizens are covered by the Social Security Institution (SSI). All health-related information regardless of insurance company and type is stored in the Turkish Ministry of Health Database (MHD), a national database containing medical information pooled from every individual from both public and private insurance companies. 6 Personal health records (PHRs) for individuals who were admitted to any health care service providers nationwide were retrieved from the Turkish MHD. All personal information was anonymized, with each individual being assigned a unique identification number. All data were encrypted and stored in a secure computer, and no personal information was disclosed.
This retrospective study evaluated HA data cataloged based on PHRs stored at the Turkish MHD between January 2016 and January 2023. The SKRS is a subunit of the MHD database in which all electronic surgical information is stored (https://skrs.saglik.gov.tr/). All surgical procedure instrument codes and diagnostic codes based on the International Classification of Diseases, 10th Revision (ICD-10) were recorded in this system with a unique identification number. The SKRS system works synchronously with the MHD to prevent data duplication. Intervention and surgical instrument package codes were also run simultaneously to confirm whether all patients undergoing HA were encoded in the database. Particular intervention codes were extracted from the database (612750, interventional HA; 612751, arthroscopic labrum repair (hip); and 612700, arthroscopic debridement of the labrum). Given that code 612700 has been used for both hip and shoulder arthroscopy and discrimination of the cases was impossible, cases using this code were excluded from this study. Instrument codes specific to HA were also searched. The corresponding codes were accepted as inclusion criteria (Figure 1).

Flow diagram of the study participants.
A binding database containing the related ICD codes was created and then sorted according to the information required. Individual ICD codes were extracted to determine the number of postoperative femoral neck fractures, postoperative anticoagulant preference, and HO prophylaxis. Thereafter, variables were classified according to sex (male/female), age (numeric), institution type (university/second- or third-stage state hospital/private), geographic zones (7 geographic zones), surgery date (HA and THA), presence of femoral neck fracture (yes/no, within 6 months), indomethacin prescription (yes/no, within 12 months), anticoagulant prescription at discharge (acetylsalicylic acid [ASA], enoxaparin sodium [LMWH], and rivaroxaban, within 10 days). All data were then categorized according to year.
The term “incidence” represents the number of HA procedures performed in every 100,000 patients admitted to the orthopaedic outpatient clinic in a particular year. 53
Statistical Analysis
Statistical analysis was performed using the statistical package SPSS software (Version 25.0; IBM Corp). Normally distributed continuous variables are presented as mean ± standard deviation (P > .05 using the Kolmogorov-Smirnov test or Shapiro-Wilk test [n < 30]), whereas nonnormally distributed continuous variables are presented as median. To calculate the incidence rate, data commands were used. Groups were compared using the Mann-Whitney U test or Kruskal-Wallis test for nonnormally distributed data. Categorical variables between the groups were analyzed using the chi-square test or Fisher exact test. We estimated the ratios for before and after periods with respect to the same period in 2022 using Poisson regression, including the period, year, and period-year interaction as fixed effects. In all analyses, a P value <.05 indicated statistical significance.
Results
More than 112 million PHRs were searched in the database from >60 million patients treated between 2016 and 2023. In total, 1580 HA procedures were identified. The most frequently entered code was 612750 (interventional HA; 1004 [63.5%] cases), followed by 612751 (arthroscopic labrum repair of the hip; 373 [23.6%] cases) and the miscellaneous surgical instrument codes (203 [12.8%] cases) (Figure 2).

The frequency of Health Coding Reference Server codes (612750, interventional hip arthroscopy; 612751, arthroscopic labrum repair; and miscellaneous instrument codes).
Among the included patients, 57.5% and 42.5% were male and female, respectively, with a male-to-female ratio of 3:2. The mean age of the patients upon surgery was 39.2 ± 11.0 years (range, 18-65 years). The mean age of female patients was higher than that of male patients upon surgery (41.1 ± 11.2 years vs 37.8 ± 10.6 years; P < .0001). Furthermore, 59.9% of the patients were aged between 30 and 50 years (Figure 3). All institutions providing health services in Turkey are connected to the SSI. Hospitals are mainly divided into public, private, and university hospitals. Although the facilities and capabilities of hospitals are determined according to the level system, hospitals differ in terms of surgical competence given the heterogeneous sociological and economic makeup of the country. Data distribution according to institution revealed that most surgeries were performed at private hospitals (n = 754; 47.7%), followed by state hospitals (n = 519; 32.8%) and then university hospitals (n = 307; 19.4%) (Table 1). A significant annual increase was observed in the preference for private hospitals (P = .001) (Figure 4).

Age of the patients at the time of hip arthroscopy surgery. The vertical axis demonstrates the cumulative number of procedures performed, whereas the horizontal axis corresponds to the age of the patients at the time of surgery.
Geographical and Institutional Distribution of Cases


Distribution of cases between 2016 and 2023 according to institution. Each color represents the number of procedures performed in different types of institutions.
An 833.3% increase in the number of HA procedures was found from 2016 to 2022 (P = .001). Analysis according to year demonstrated a significant increase in procedure counts from 2016 to 2018 and 2020 (P = .001). From 2019 to 2020, an 18.8% decrease in the number of surgeries was noted. Although the number of surgeries consistently increased in 2020, no significant increase was observed in 2021 and 2022 (Figure 5).
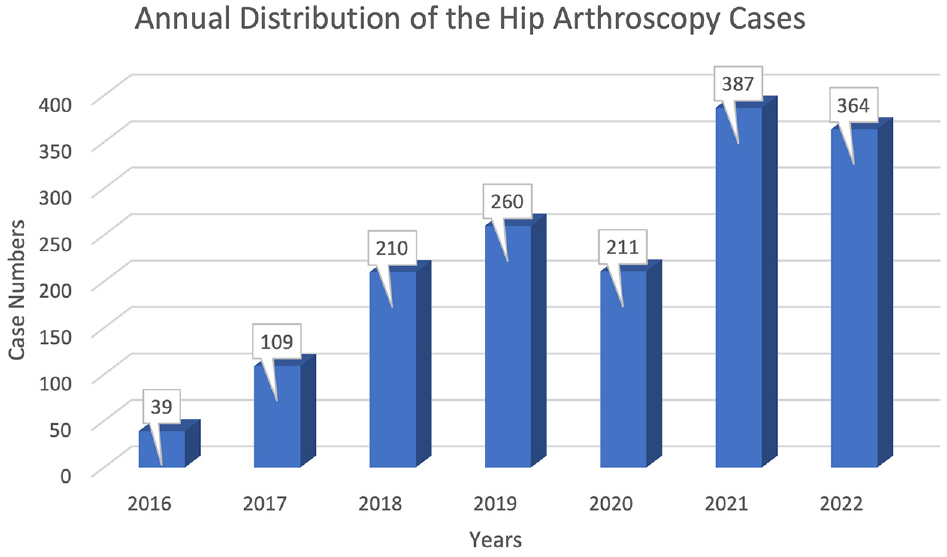
Annual number of hip arthroscopy procedures performed between 2016 and 2023.
The incidence of HA was 0.37 and 2.86 cases per 100,000 patients in 2016 and 2022, respectively. The ratio of HA to general orthopaedic surgeries also significantly increased from 0.003% in 2016 to 0.038% in 2022 (P = .001). The ratio of HA to all orthopaedic surgeries significantly increased from 2016 to 2018 and 2020 (P < .05) (Table 2).
Incidence of Hip Arthroscopy Between 2016 and 2022

Indicates a statistically significant increase.
Most of the cases occurred in the Marmara region (56.1%; P = .001), followed by central Turkey (Central Anatolia) (32.9%) and western Turkey (Aegean) (7.1%) (Figure 6).

Heat map for the geographical distribution of hip arthroscopy procedures per year and overall total. Darker colors correspond to higher values, whereas lighter colors represent lower values.
Among the 1580 patients analyzed, 1446 (91.5%) discharge prescriptions were identified. LMWH (n = 1437; 99.4%) was the most prescribed anticoagulant, followed by ASA (n = 8; 0.6%) and rivaroxaban (n = 1; 0.1%). Postoperative indomethacin prescriptions were used to evaluate trends in HO prophylaxis. A total of 223 HO prophylaxis prescriptions were found, with a significant annual increase observed (P = .001).
According to the obtained data, 76 THA procedures were performed throughout the study duration. Cases in which the duration until THA exceeded 2 years after HA were classified as irrelevant. As such, 20 cases were excluded. Therefore, 56 (3.5%) THA conversions were encountered from 2016 to 2022. Additionally, among cases requiring THA conversion, female patients significantly outnumbered male patients (P = .0001). There was no annual significant difference in THA conversion numbers over the course of study (P = .172). Within 2 years after HA, 2 (0.1%) cases of femoral neck fractures were identified.
Discussion
The current study primarily showed trends in (1) the number of HA procedures and ratio of HA procedures to other orthopaedic procedures, (2) yearly incidence rates, (3) annual geographical distribution of the cases, (4) postoperative VTE prophylaxis preference, (5) THA conversion rates, (6) femoral neck fracture rates, and (7) HO prophylaxis prescription preference and rates.
Specially, our data showed an 833.3% increase in the number of procedures from 2016 to 2022 (P = .001). The number of HA procedures, ratio of HA to all orthopaedic procedures, and incidence of the HA significantly increased in 2016, 2017, 2018, and 2020. HA had an overall incidence of 1.9 per 100,000 between 2016 and 2022. LMWH was the most preferred agent (99.4%) for VTE prophylaxis, with only 0.6% of the physicians initially prescribing ASA. Conversion to THA was found in 3.5% of the cases. Femoral neck fractures as a devastating complication were encountered in only 0.1% of the patients throughout the study duration.
Recent demographic studies have demonstrated up to a 3-fold increase in the number and incidence of HA among the other orthopaedic interventions.8,16,55 This increase was attributed to the increased demand for minimally invasive surgery, faster recovery times, broader indications for surgery, and increased awareness of the topic through social media. 22 In 2020, elective orthopaedic interventions were canceled or postponed for some time, with the total number of such interventions decreasing by almost half. 51 Elective hip preservation surgeries were even more affected, with a decrease of up to 64%. 5 In the current study, both the number of HA procedures and the ratio of HA to other orthopaedic interventions significantly increased between 2016 and 2018. Furthermore, the current findings clearly depict the impact of coronavirus 2020, which presented as an 18.8% decrease in the number of interventions during the outbreak. In 2021, a significant increase in the number of surgical procedures was observed (P = .001); however, no substantial increases were observed in 2022.
HA as a treatment for cam deformities in FAI aims to restore the decreased femoral head–neck offset by resecting abnormal bulkiness. 44 However, the optimal amount of resection remains unclear, and overresection may cause fractures by weakening the femoral neck. Femoral neck fractures are a rare yet devastating complication of HA. 2 Our study demonstrated a femoral neck fracture incidence of 0.1%, which was similar to those reported by Merz et al (0.07%), 37 Gedouin et al (0.09%), 18 and Horner et al (0.1%). 25 However, our findings were not consistent with that reported by Zingg et al, 54 who found an incidence rate of 1.9%, which was markedly higher than that reported in the literature, although all such fractures were insufficiency fractures detected through magnetic resonance imaging. These variations between studies could be attributed to differences in postoperative weightbearing protocols, patient selection, and surgical competency as experience is accumulated.
The current study found an initial anticoagulant prescription rate of 91.5%, with LMWH (99.3%) being the most preferred medication for chemoprophylaxis, followed by ASA and rivaroxaban with usage rates of 0.6% and 0.1%, respectively. Unlike our findings, a systematic review revealed that only 48.3% of patients received chemoprophylaxis for VTE. 20 A study by Holler et al 24 revealed that only 2.1% of the patients received chemoprophylaxis, with preference rates for LMWH, aspirin, and rivaroxaban being 52.3%, 42.8%, and 4.9%, respectively. Moreover, a systematic review by Haldane et al 20 found that aspirin and LMWH were used in 1095 (75.8%) and 166 (11.5%) hips, respectively. Consequently, the necessity of routine thromboembolic prophylaxis for HA remains controversial but recommended for patients with risk factors. Nonetheless, studies have emphasized the importance of staying in the safe zone.1,7,24 In the current study, the most used perioperative prophylaxis was LMWH, with our preference rates being greater than that reported in the literature.
In the current study, the incidence of HA was 2.86 per 100,000 patients in 2022. Montgomery et al 40 stated a 365% increase in the incidence of HA (from 12 to 55.8 per 100,000 from 2004 and 2009), whereas Bonazza et al 8 and Maradit Kremers et al 35 reported similar increases continuing between 2008 and 2013 in the United States. Evidence suggests that newly qualified surgeons tend to perform an increasing number of procedures every year given their heightened enthusiasm triggered by the surgical education received during residency. 9 Zusmanovich et al 55 also reported an 85% increase in the incidence of HA (ie, from 73.1 to 135.4 per 100,000) between 2011 and 2018. Overall, the incidence rates obtained in the current study were prominently lower than those reported in the literature. However, such increases project an eventual rise in the number of HA procedures in the near future. Although HA has been introduced early, the increase in the number of procedures seems to be delayed, probably because of the steep learning curve and high device dependence as stated by Lee et al. 31 In our study, a significant increase in the ratio of HA to other orthopaedic procedures was observed from 2016 to 2018 and 2020 (P = .001). In Turkey, HA is still in its infancy and possesses a huge potential for further growth in the future.
The current study found that the number of HA procedures performed nationally showed an increasing trend, consistent with reports documenting early increases in arthroscopy adoption globally. In particular, studies have shown a 110% increase in Korea and a 770% increase in the United Kingdom.32,43 Studies conducted in the United States between the 2000s and early 2010s have also reported a 1.8- to 3.65-fold increase in HA surgery volume.8,35,40,50,55 Finally, recent studies conducted in Sweden and Finland reported a rapid decrease (up to 47%) in the number of procedures after a rapid peak in the early 2010s.26,52 Consistent with the typical life cycle of surgical procedures, sharp increases in case volumes are expected at the early stages of development, followed by a plateau and potential decrease as the procedure becomes more established. Our findings suggest that Turkey is in the early phase of the HA life cycle. Close monitoring of the development is required to estimate future trends and potential shift toward the utilization of HA as a surgical treatment option.
THA is the most common reoperation procedure after HA. 21 Our study demonstrated that 3.5% of the cases required conversion to THA within 2 years after the index surgery, with women being significantly more likely to require conversion to THA compared with men (P = .0001). Aside from type of arthroscopic surgery performed, age and OA severity have been identified as major predictors of future conversion to THA. 30 Indeed, studies have shown that older patients and those with preoperative arthritis are more likely to require conversion to THA.10,21,48 Sardana et al, 47 who reported a THA conversion rate of 5.6%, emphasized that THA conversion mostly occurs within 2 years after the index surgery and that underresection is the most probable cause. To be compatible with the literature, the same time frame was scanned in current study. In another study, Schairer et al 48 reported a THA conversion rate of 11.7%, with older patients, those with obesity, and low-volume centers showing increased rates. Similarly, Hoit et al 23 reported a THA conversion rate of 9.3% in a recent study involving 2545 patients and determined that older age and labral resection rather than repair were risk factors for THA conversion. In contrast, another systematic review by Harris et al 21 reported a conversion rate of 2.9%; however, this study included only HA procedures without any exclusions, with most studies being level 4 studies and case reports. Consequently, available evidence suggests that patient-related factors are the main determinants of THA conversion. We believe that this conversion rate will likely decrease as more suitable surgical candidates are identified. However, the current study demonstrated no significant difference in conversion rates throughout the study duration (P = .172).
The current study found that 14.1% of the cases were prescribed postoperative indomethacin. Bedi et al 4 stated that combining naproxen with indomethacin reduced the rate of HO from 8.3% to 1.8% compared with naproxen alone. Conversely, the effects of routine nonsteroidal anti-inflammatory drug use remain uncertain, and further studies are needed to determine whether the advantages of routine nonsteroidal anti-inflammatory drug use outweigh the disadvantages. Our findings indicate that physicians have some degree of knowledge regarding HO prevention, but routine prescription is not widely preferred.
Limitations
The current retrospective study is not without limitations. First, data were extracted from a large data pool after a mining process, which may have resulted in the inclusion of incorrect, incomplete, or missing data. Access to more detailed follow-up and perioperative data, such as rehabilitation protocol, postoperative medications, functional scores, and complication rates, could be possible with the implementation of indication-specific registries on the electronic surveillance system. Second, the SKRS code 612750 corresponds to interventional HA but does not truly specify the procedure performed. Therefore, we could not establish cohorts according to the specific treatment techniques received, such as labrum debridement and labrum repair. Considering that HA is still a relatively new surgical method, the intervention codes have yet to completely cover the surgery performed. Therefore, the complexity of the surgeries may have varied widely, and more detailed analysis was currently impossible. Third, the rate of THA conversion secondary to HA was determined based on the number of THAs performed within 2 years after index HA. Given that the codes do not specify the laterality, we could not determine whether additional surgeries were performed on the same side as the index surgery. Last, the current study did not include HA procedures performed in small clinics that are not covered by either private or public health insurance. Hence, only a negligible number of patients might have been missed. Despite these limitations, our findings still provide valuable insights on the trends of HA nationwide.
Conclusion
This study described the current trends in HA across Turkey and provided a perspective on physician preferences. Notably, HA procedure counts, the ratio between HA and other orthopaedic procedures, and the incidence of HA demonstrated an increasing trend, with enormous potential for further advancement. Our findings highlight the need for the creation of a national registry capable of obtaining more specific and accurate data.
Footnotes
Acknowledgements
The authors express sincere gratitude to the Turkish Society of Preventive Hip Surgery (KEKCD) and Sports Traumatology, Arthroscopy, Knee Surgery Association (TUSYAD) Hip Joint Branch and TUSYAD Istanbul Scientific Workshop Study Group for their invaluable support that significantly contributed to the development of HA in Turkey. Additionally, the authors thank all HA enthusiasts and contributors for their collective efforts and insights that have significantly enriched the research.
Final revision submitted April 14, 2024; accepted May 3, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Turkish Ministry of Health (95741342-020/27112019).