
Abstract
Background:
The conversion rate of hip arthroscopy (HA) to total hip arthroplasty (THA) has been reported to be as high as 10%. Despite identifying factors that increase the risk of conversion, current studies do not stratify patients by type of arthroscopic procedure.
Purpose/Hypothesis:
To analyze the rate and predictors of conversion to THA within 2 years after HA. It was hypothesized that osteoarthritis (OA) and increased patient age would negatively affect the survivorship of HA.
Study Design:
Cohort study; Evidence level, 3.
Methods:
The IBM MarketScan database was utilized to identify patients who underwent HA and converted to THA within 2 years at inpatient and outpatient facilities between 2013 and 2017. Patients were split into 3 procedure cohorts as follows: (1) femoroacetabular osteoplasty (FAO), which included treatment for femoroacetabular impingement; (2) isolated debridement; and (3) isolated labral repair. Cohort characteristics were compared using standardized differences. Conversion rates between the 3 cohorts were compared using chi-square tests. The relationship between age and conversion was assessed using linear regression. Predictors of conversion were analyzed using multivariable logistic regression. The median time to conversion was estimated using Kaplan-Meier tests.
Results:
A total of 5048 patients were identified, and the rates of conversion to THA were 12.86% for isolated debridement, 8.67% for isolated labral repair, and 6.76% for FAO (standardized difference, 0.138). The isolated labral repair cohort had the shortest median time to conversion (isolated labral repair, 10.88 months; isolated debridement, 10.98 months; and FAO, 11.9 months [P = .034). For patients >50 years, isolated debridement had the highest rate of conversion at 18.8%. The conversion rate increased linearly with age. Factors that increased the odds of conversion to THA were OA, having an isolated debridement procedure, and older patient age (P < .05).
Conclusion:
Older patients and those with preexisting OA of the hip were at a significantly increased risk of failing HA and requiring a total hip replacement within 2 years of the index procedure. Younger patients were at low risk of requiring a conversion procedure no matter which arthroscopic procedure was performed.
The volume of hip arthroscopy (HA) has steadily grown throughout the past decade. In New York State alone, there was a 495% increase in HA surgeries from 29 2004 to 2016. Despite the growing popularity of HA, a subset of patients may experience failure of arthroscopic intervention, requiring revision HA or conversion to total hip arthroplasty (THA). Previous arthroscopy is a risk factor for periprosthetic dislocation and revision after THA, and conversion rates from HA to THA within 2 years after HA can range3,9,10,21 between 4% and 17%. Previous studies found that female sex, older age, obesity, smoking, osteoarthritis (OA), and lower preoperative modified Harris Hip Scores were risk factors that increase HA to THA conversion.3,6,10,11,13,14,24,26,30,31,33 Furthermore, the hospital operating costs for conversion to THA can be up to 26.4% higher than the costs for primary THA. 5 Thus, patients who experience HA failure and require conversion to THA can experience high total health care costs and increased risk exposure from a second anesthesia event. 27 Further exploration of risk factors that increase the rate of HA to THA conversion can help alleviate the patients’ financial health care burden and improve hospital resource utilization.
Although the nationwide incidence of HA has increased among all age groups, previous studies have found that patients >45 years performed worse than younger patients after HA.7,31 Patients >50 years had a 17% conversion to THA rate compared with <1% in patients <30 years. 31 Labral repair is more common in patients <30 years, and HA with isolated labral debridement is more common in older age groups.8,31 With respect to the specific HA procedure performed, patients who undergo debridement and partial resection of the labrum have relatively worse outcomes. 10 However, the risk factors for higher conversion rates to THA after specific HA procedures for FAI are insufficiently explored. Thus, the effects of age and procedure type on survivorship for HA require further investigation.
Current studies investigating risk factors for conversion to THA after HA utilize data from single institutions and are thus limited in sample size and diversity in their patient population. To assess the external validity of these smaller studies, we used a large national database to analyze the rate and predictors of conversion to THA within 2 years after 1 of the 3 HA procedures. 12 Specifically, we aimed to identify novel patient characteristics predictive of failure and quantify the independent effect of these characteristics on patient outcomes. We hypothesized that OA and increased patient age would negatively impact the survivorship of HA.
Methods
Data Source
In this retrospective cohort study, we utilized the IBM MarketScan Commercial Claims Encounter database. This large national insurance claims database includes >32 billion service records and contains data from active employees, early retirees, and dependents insured by employer-sponsored plans within the United States. The patient population of the database is composed of patients <65 years, which is the majority of the HA patient population. 28 Patients with Medicare, Tricare and Medicaid, as well as uninsured patients, were not included, as this database does not include these patients. A previous large-scale study of over 5000 patients found that 79.3% of patients who had HA had private insurance, while only 2.3% had Medicare. 18 Thus, our methodology aimed to cover the majority of patients who had HA.
Study Population and Inclusion/Exclusion Criteria
The study population—referred to as the full HA cohort—consisted of patients >18 years with the following HA Current Procedural Terminology (CPT) codes: 29860 (HA, diagnostic with or without biopsy), 29861 (HA, removal of loose body or foreign body), 29862 (HA, chondroplasty, abrasion arthroplasty and/or resection of the labrum, 29863 (HA, synovectomy), 29914 (HA, femoroplasty), 29915 (hip arthroscopy, osteoplasty acetabulum), and 29916 (HA, labral repair). Pediatric patients were excluded because of a higher risk of concomitant congenital hip pathologies. Patients with the above CPT codes and initial HA surgery dates between January 1, 2013, and December 31, 2015, with 2 years of continuous enrollment in the database were included. The full cohort was then split into 3 procedure cohorts: (1) femoroacetabular osteoplasty (FAO)—patients undergoing treatment for FAI with CPT codes 29914 or 29915, with labral repair or any of the debridement codes; (2) isolated debridement, with CPT codes 29860, 29861, 29862, 29863; and (3) isolated labral repair, with CPT code 29916, with any of the debridement codes but without 29914 or 29915. We excluded CPT code 29999 (unlisted procedure, arthroscopy) because this code does not allow the identification of the specific HA procedure. 32 Patient records were then reviewed for 2 years (through December 31, 2017) to identify patients who converted to THA, identified by CPT codes 27130 and 27132, in that period. Both inpatient and outpatient THAs were included.
Study Variables
The following variables were chosen for analysis: sex, age, geographical region, insurance plan type, Deyo-Charlson Comorbidity Index (DCCI), obesity status, tobacco use, OA, and year in which the procedure was performed. 23 Obesity status, tobacco use, and hip OA diagnoses were identified using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and ICD-10-CM diagnosis codes (Appendix Table A1).4,23 Age was reported as a continuous variable and as age groups ≤40, 41-50, and 51-60 years. The geographic region within the United States was categorized as Northeast, North Central, South, or West. The DCCI was categorized into 2 groups (0 and ≥1), as we found that >99% of patients who had HA fell within these groups.
The insurance plan type was grouped into the following 3 categories: (1) preferred provider organization and exclusive provider organization; (2) health maintenance organization, point of service (POS), and POS with capitation; and (3) high deductible health plan and consumer-driven health plan. The rationale for these groupings was as follows: The first category includes plans with higher premiums but provide more autonomy for patients in choosing their provider. Patient responsibility—including copays, deductibles, and coinsurance—is also lower than the plans in the third category. Category 2 plans have the least patient responsibility but provide the least out-of-network coverage. These plans also require referrals to see specialists but have the lowest deductibles and premiums. Category 3 plans have lower premiums than Category 1 but higher immediate patient out-of-pocket expenditures. Patients with insurance plan types defined by the database as “basic/major medical” and “comprehensive” were grouped in the “other” category, as the database did not specify how these plans were defined.
Statistical Analysis
Continuous variables were reported as medians with interquartile ranges (IQRs), and categorical variables were reported as numbers with percentages. Differences between cohorts (FAO, isolated debridement, and isolated labral repair) for study variables were analyzed using standardized differences (Std Diff) instead of P values to incorporate a degree of effect size analysis given the large sample size. 2 A Std Diff of ≥0.1 (or 10%) indicates a meaningful difference in covariate distribution between the 3 patient cohorts. Kaplan-Meier analysis was used to estimate the time (reported as median with IQR) to THA conversion after HA for each HA procedure cohort.
Logistic Regression Model
A multivariable logistic regression model was utilized to estimate the odds ratios (ORs) with corresponding 95% CIs for the outcome of conversion to THA when considering the aforementioned study variables as well as the HA procedure performed. Categorical age groups were utilized for the logistic regression analysis. For each age group, conversion rates were calculated for the full HA cohort and the FAO, isolated debridement, and isolated labral repair cohorts, and the chi-square test was used to compare rates of conversion between the 3 HA procedure cohorts within each age group. Univariable linear regression was utilized to examine the relationship between age as a continuous variable and the rate of conversion from HA to THA for each HA procedure cohort for patients 30 to 60 years old. Statistical significance was set at P < .05.
Subgroup Analysis Isolating Strongest Predictors of Conversion to THA
Multivariable logistic regression analysis found that OA and age >50 years were the greatest predictors of conversion to THA; thus, a subgroup analysis was performed to isolate these factors and determine the resulting rate of conversion, the median time to conversion, and the odds of conversion. Four groups were included: (1) patients ≤50 years without OA; (2) patients ≤50 years with OA; (3) patients >50 years without OA; and (4) patients >50 years with OA. The conversion rate was reported as numbers and percentages, and the groups were compared using Std Diff. The time to conversion was obtained using the Kaplan-Meier method. For odds of conversion, a multivariable logistic regression model isolated these 4 groups with an interaction term while controlling for the aforementioned study variables.
Results
Patient Population and Descriptive Statistics
A total of 5048 patients were identified, of whom 3580 (70.9%) underwent treatment for FAI (the FAO cohort), 972 (19.3%) underwent isolated debridement, and 496 (9.8%) underwent isolated labral repair. The majority of patients undergoing FAO and isolated labral repair were in the ≤40-year age group (FAO, 50.81%; isolated labral repair, 50.2%), whereas isolated debridement had a more balanced distribution with 35.6% of patients in the ≤40-year age group, 31.48% in the 41–50 year age group, and 32.92% in the 51–60 year age group (Std Diff, 0.260) (Table 1). The isolated labral repair cohort had the highest proportion of women, while the FAO group had the lowest proportion of women (Std Diff, 0.270), but most patients in the full HA cohort were women (65%). Patients were overwhelmingly healthy, with most patients in the full cohort having a DCCI score of 0. Moreover, 13.8% of all patients had a diagnosis of OA with no differences between the 3 procedure cohorts (Std Diff, 0.088). The isolated debridement cohort had the highest rate of conversion to THA (isolated debridement, 12.86%; isolated labral repair, 8.67%; FAO, 6.76% [Std Diff, 0.138]), but the isolated labral repair cohort had the shortest time to conversion (isolated labral repair, 10.88 months; isolated debridement, 10.98 months; FAO, 11.90 months [P = .034]) (Table 1). However, the statistically significant difference between 10.88 months and 11.90 months was likely not clinically significant.
Characteristics of the Patient Population According to FAO, Isolated Debridement, and Isolated Labral Repair Procedure Cohorts (N = 5048) a
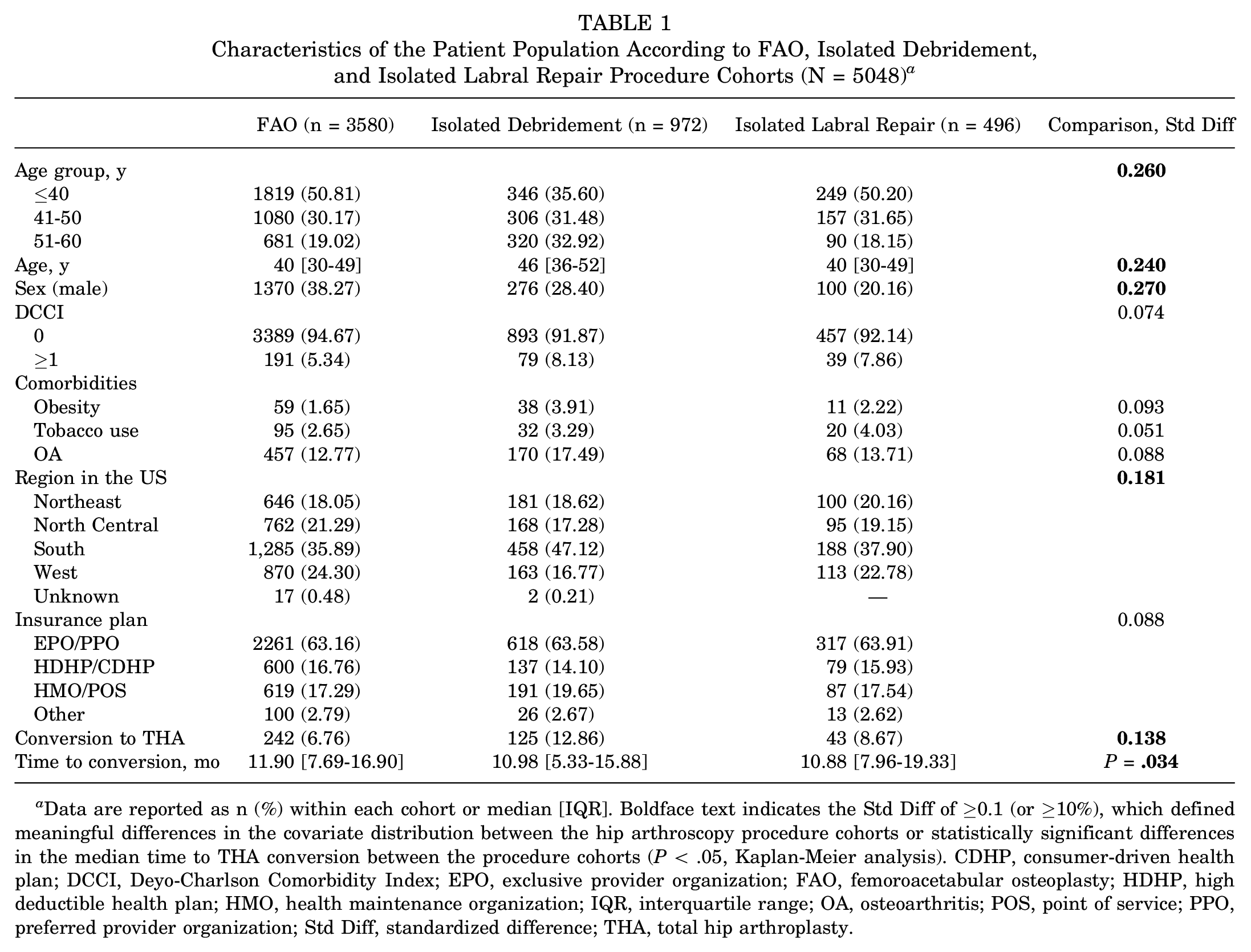
Data are reported as n (%) within each cohort or median [IQR]. Boldface text indicates the Std Diff of ≥0.1 (or ≥10%), which defined meaningful differences in the covariate distribution between the hip arthroscopy procedure cohorts or statistically significant differences in the median time to THA conversion between the procedure cohorts (P < .05, Kaplan-Meier analysis). CDHP, consumer-driven health plan; DCCI, Deyo-Charlson Comorbidity Index; EPO, exclusive provider organization; FAO, femoroacetabular osteoplasty; HDHP, high deductible health plan; HMO, health maintenance organization; IQR, interquartile range; OA, osteoarthritis; POS, point of service; PPO, preferred provider organization; Std Diff, standardized difference; THA, total hip arthroplasty.
Logistic Regression Model
In the multivariable logistic regression model, the factors associated with the highest risk of conversion to THA included older age and OA. When compared with patients ≤40 years, patients in the 41–50 year age group were >3 times as likely to convert to THA (OR, 3.23 [95% CI, 2.39-4.37]; P < .001), and patients in the 51–60 year age group were >6 times as likely to convert (OR, 6.50 [95% CI, 4.83-8.75]; P < .001). OA also increased the odds of conversion by >3 (OR, 3.35 [95% CI, 2.66-4.23]; P < .001). Obesity significantly increases the odds of conversion (OR, 1.76 [95% CI, 1.01-3.09]; P = .048), and the isolated debridement procedure type increased the odds of THA conversion when compared with FAO (OR, 1.46 [95% CI, 1.14-1.87]; P = .003). In contrast, the isolated labral repair procedure type did not increase the odds of conversion compared with FAO. In addition, the procedure performed in the Southern region of the United States decreased the odds of conversion to THA compared with the West (OR, 0.74 [95% CI, 0.47-1.18]; P = .037). Sex, increased DCCI, tobacco use, the year the procedure was performed, and the insurance plan type had no effect on conversion to THA (Table 2).
Multivariable Logistic Regression Model Assessing Predictors to THA (N = 5174) a
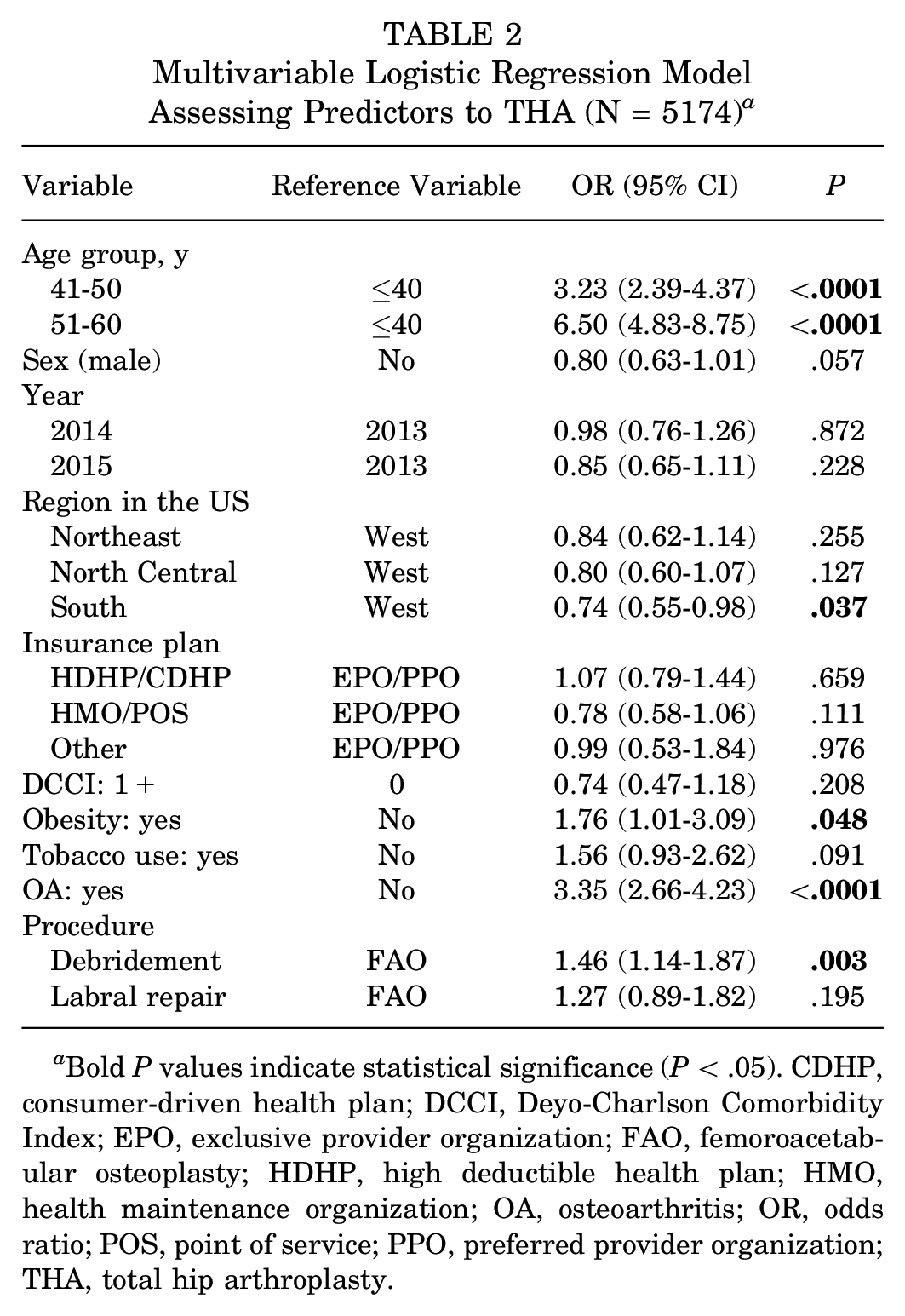
Bold P values indicate statistical significance (P < .05). CDHP, consumer-driven health plan; DCCI, Deyo-Charlson Comorbidity Index; EPO, exclusive provider organization; FAO, femoroacetabular osteoplasty; HDHP, high deductible health plan; HMO, health maintenance organization; OA, osteoarthritis; OR, odds ratio; POS, point of service; PPO, preferred provider organization; THA, total hip arthroplasty.
Relationship Between Age and Conversion Rate
In patients ≤40 years, the conversion rate for the full cohort was low at 2.7%, and there were no differences in the conversion rate between the 3 HA procedure cohorts on chi-square analysis. In patients aged 41 to 50 years, the overall conversion rate increased to 9.5%, and we found a significant difference in conversion rates between the 3 procedure cohorts (P = .043). Isolated labral repair had the highest conversion rate at 11.3%, followed by isolated debridement at 10.8% and FAO at 7.6%. Patients 51 to 60 years old had the highest conversion rate at 18.2%, and a significant difference between the 3 cohorts was also observed (P = .021). In this age group, isolated debridement had the highest conversion rate at 18.8%, followed by isolated labral repair at 15.1%, and FAO again had the lowest conversion rate at 13.7% (Figure 1). When age was treated as a continuous variable on linear regression, we found that conversion rates for the full cohort and all 3 subcohorts significantly increased with age in a relatively linear fashion. The full cohort and the FAO subcohort had the highest R2 values (full cohort, R2 = 0.817 [P < .0001]; FAO, R2 = 0.789 [P < .001) (Figure 2).

The conversion rate to THA by age group and procedure cohort.

The relationship between age and the conversion rate to THA for the (A) full hip arthroscopy cohort and the procedure cohorts: (B) femoroacetabular osteoplasty, (C) isolated debridement, and (D) isolated labral repair. R2 correlation coefficients represent the strength of the relationship.
Subgroup Analysis Isolating Strongest Predictors of Conversion to THA
Logistic regression analysis revealed that the strongest predictors of conversion to THA were OA and age >50 years. Subgroup analysis of patients showed that 33.8% of patients in this subgroup converted to THA within 2 years. This was significantly higher than patients >50 years without OA (14.2%), patients ≤50 years with OA (14.7%), and patients ≤50 years without OA (4.1%) (Std Diff, 0.415). However, no difference was observed in the median time to conversion between the 4 groups (P = .096). Multivariable logistic regression analysis showed that patients >50 years with OA were 11.24 times more likely to convert to THA than patients ≤50 years without OA (95% CI, [8.05-15.70]; P < .001), while patients >50 years without OA were 3.72 times more likely to convert (95% CI, [2.90- 4.86]; P < .001) and patients <50 years with OA were 4.14 times more likely to convert (95% CI, 3.04-5.63; P < .001) (Table 3).
Results of Subgroup Analysis Isolating Strongest Predictors of Conversion to THA a

Data are presented as n (%), median [IQR], OR (95 CI%). Boldface text indicates statistical significance (Std Diff of ≥0.1 [or ≥10%]). IQR, interquartile range; OA, osteoarthritis; OR, odds ratio; Std Diff, standardized difference; THA, total hip arthroplasty.
Discussion
The main findings of this study were that older age, OA, and isolated debridement increased the risk of conversion to THA within 2 years. When managing patients with these risk factors, the patient must be fully informed of the risk of procedure failure and presented with alternative treatment approaches. To minimize risk and optimize outcomes for any unique patient, the ultimate treatment plan must be established through informed, shared decision-making. Furthermore, the surgeon must consider whether an arthroscopic procedure is in the best interest of the patient in certain circumstances. The surgeon should understand the limits of HA and that certain patients would achieve a better, longer-lasting outcome from THA. Perhaps most importantly, the surgeon should be able to identify these patients and, if they do not perform THA themselves, be willing to refer them to an appropriate surgeon.
The descriptive data trends presented in this study closely approximate those of the current body of the literature. In their study of more than 8000 patients, Sing et al 31 found that nearly half of the patients undergoing HA were <40 years. Similarly, Rosinsky et al, 26 in their analysis of HA procedures at a single institution, found that the mean patient age was 37 years. In comparison, we found that patients <40 years comprised 47.8% of the study population. The similarity in the reported values between these 3 studies, paired with the differences in dataset size and scope, suggests that the data reported are precise and accurate.
Investigating procedural trends of HA, we found that the most common surgery in all 3 age cohorts was for FAI, which accounted for over 70% of HA cases; isolated debridement and isolated labral repair comprised 19.3% and 9.8% of cases, respectively (Std Diff, 0.260). Any patient who underwent treatment for FAI was included in the FAO cohort and only the FAO cohort. However, comparison with the findings of Sing et al 31 is not possible, as data on procedures for FAI treatment were only reported for 1 of the 5 years investigated in their study. On a smaller scale, a study of 2545 patients from a single Canadian city who underwent HA found that 58% of patients underwent treatment for FAI either with or without a labral procedure, while 16.58% and 16.70% of patients underwent isolated labral repair and isolated labral debridement, respectively (remainder of methods not specified). 10 Independent of the performance of procedures for FAI, labral repairs occurred in 48.36% of patients in this Canadian study. A European study of >50000 patients from the Danish Hip Arthroscopy Registry reported that a labral repair procedure was performed in 82% of HA patients, while a debridement or labral resection was completed 20 in only 17%. Interestingly, treatment for FAI was addressed in 93% of surgeries. The difference in rates of specific surgical procedures performed during HA between these 3 studies is substantial. Osteoplasty was performed in 71% of patients in this study, while it was performed in only 58% of Canadian patients and 93% of Danish patients. The reasons underlying this discrepancy have not yet been investigated. Also of note is the finding that a labral repair was performed in 82% of patients in the Danish registry. However, the Canadian study does not report data on labral procedures in patients who also underwent osteoplasty. Similarly, our study fails to delineate between patients who underwent labral debridement with osteoplasty and those who underwent labral repair with osteoplasty. This is a limitation of our study, and future literature should explore international and regional differences in performance rates of specific arthroscopic procedures.
Subsequently, the 2-year THA conversion rate of matched cohorts of patients with a difference of opinion on appropriate surgical management should be compared. Hip preservation surgery aims to delay or eliminate the need for future THA conversion. This is most important in young patients whose lifetime risk of revision THA is elevated. In the cohort of youngest patients, this study revealed a low rate of conversion surgery. Overall, only 2.7% of patients aged ≤40 years underwent THA within 24 months of HA. A subgroup of patients who underwent procedures to address FAI accounted for over 3 quarters of this cohort. It demonstrated a conversion rate of 2.4%—the lowest rate of any subgroup investigated. This low conversion rate in young patients is an encouraging finding, suggesting that the vast majority of young patients avoid an undesirable outcome for at least the first 2 years after surgery. That being said, the 2-year follow-up data may not have been long enough for OA, a chronic disease, to progress to the point of THA conversion in younger patients, as their joints were relatively healthier at baseline. Longer-term follow-ups at 10 or 20 years postoperatively may reveal different results and will aid our understanding of the effects of various arthroscopic interventions.
The findings of this study support the current body of evidence that older patients are at higher risk of undergoing THA conversion after HA.11,31 We found the odds of requiring conversion surgery to be 3.23 times higher (P < .001) for patients 41 to 50 years old and 6.50 times higher (P < .001) for patients >50 years old compared with the youngest patients. Examining the >50-year-old cohort in isolation, the specific HA procedure performed does have a significant association with subsequent THA conversion. The oldest patients who underwent isolated debridement during HA had a significantly higher conversion rate (18.8%; P = .021) than those who underwent isolated labral repair (15.1%) or an FAI procedure (13.7%). When possible, repair of the labrum is preferable to debridement and resection, as it more closely restores the natural biomechanics of the hip and slows the development of degenerative disease.14,15,19 It is possible that those older patients who underwent isolated debridement had complex, harder-to-repair or irreparable labral tears and thus poorer joint health preoperatively. Obesity was also found to be an independent risk factor for elevated risk of HA failure and THA conversion (OR, 1.762 [95% CI, 1.005-3.090]; P = .048). This supports the similar findings of Kester et al 13 in their analysis of New York State patients undergoing HA and those of Horner et al 11 in their systematic review. A likely explanation for this increased risk in obese patients is the simple relationship between increased body weight and increased loading forces experienced by the hip, which could also lead to more rapid development of OA. 25 Nonetheless, obesity has not been established as a contraindication to HA, as previous studies have shown that obese patients can still derive improvements in pain and functionality from well-indicated arthroscopic interventions. 22
Perhaps unsurprisingly, when evaluating the study population as a whole, the variable most predictive of early THA conversion was the presence of a concomitant diagnosis of OA (OR, 3.35 [95% CI, 2.66-4.23]; P < .001). Even though many procedures performed utilizing HA may be referred to as hip preservation procedures, it is now understood that preservation techniques are only reliably successful in patients with minimal preexisting arthritis. 6 The current body of evidence suggests that the severity of arthritis is inversely related to the likelihood of the procedure providing symptomatic relief.6,33 As discussed above, increasing age displayed a similar inverse relationship with the success of the HA procedure. The regression analysis presented in this study demonstrates that both age and the presence of preexisting arthritis in the ipsilateral hip are independently predictive of increased risk of requiring early conversion THA. Given that advanced age and increasing severity of OA tend to go hand-in-hand, a subgroup analysis of these highest-risk patients was performed.16,17 Compared with patients ≤50 years without arthritis, patients >50 years with concomitant arthritis of the operative hip were >11 times as likely to require THA conversion within 2 years of the index procedure (OR, 11.24 [95% CI, 8.05-15.70]; P < .001).
Clinically, the findings presented in this study highlight the importance of carefully evaluating the surgical candidacy of each patient. In addition to age, the patient’s degree of arthritic change, as well as the severity of their labral pathology, should also be considered. In those patients who are subsequently determined to be at high risk of conversion THA, physician-patient communication and the preoperative establishment of postoperative expectations are critical. Older patients must understand that they may have a >1 in 7 chance of undergoing hip replacement surgery in the first 24 months after HA, and those with concomitant arthritis must be informed that their risk is significantly higher. Further investigation will identify additional demographic, imaging, preoperative, and intraoperative characteristics that place a patient at increased risk for a poor outcome after HA surgery and may be used to optimize indications, outcome, and, ultimately, patient care.
Limitations
There are several limitations to this study. First, as with any database study, the reliability of the results produced depend on the accuracy and reliability with which data are entered. MarketScan, the dataset used in this study, has been externally validated and is widely accepted and utilized throughout the surgical research community. 1 However, classification based on coding can also compromise the accuracy of our procedure cohorts because surgeons may prefer certain CPT codes more than others, or there may be arthroscopic procedures performed that can be difficult to document with CPT codes because of bundling accurately. For example, the MarketScan database does not provide granular data regarding microfracture procedures and capsular closures that may affect the survivorship of the arthroscopic procedure. We did not include patients with Medicaid or uninsured patients because of limitations of the MarketScan database, and the database did not have data available on the severity of OA in the hip, patient outcome measures, or the effect of nonoperative treatment.
Moreover, this study did not include information on hip dysplasia, although we attempted to exclude patients with hip dysplasia by only including patients >18 years. As mentioned before, another limitation of this study was the lack of delineation between patients who underwent a labral procedure alone and those who experienced a labral procedure and concomitant osteoplasty. In addition, with only 2 years of postoperative data, it is possible that significant differences between age cohorts and procedural cohorts were not recognized. Significant differences that take longer to declare will be recognized by subsequent studies with longer-term follow-up data and will be valuable to our understanding of the benefits of HA and patients’ postoperative progression. The study was also limited by the lack of data on the surgeon performing the procedure, including surgeon procedural volume. There is a learning curve when performing the specific procedures investigated in this study, as with any surgical procedure. In most cases, surgeons who are more experienced with the procedure will perform a higher quality procedure than less experienced surgeons, and it is reasonable to assume that such a difference would ultimately affect the outcome of the patient. Finally, the study was limited to the upper age limit of the inclusion criteria. Many people in the United States switch their insurance to Medicare upon turning 65 years old. When this happens, their data are no longer included in MarketScan, resulting in patients in the cohort >60 years who are lost to follow-up. Future studies should investigate the outcomes and utility of HA procedures in older adults.
Conclusion
This retrospective cohort study utilized a large commercial claims database to analyze trends and risk factors for conversion to THA within 2 years of undergoing an HA procedure. Younger patients were found to be at very low risk for conversion no matter which of the 3 HA procedures they underwent. On the contrary, the risk of conversion was significantly higher in older patients, particularly those who underwent an isolated debridement. Finally, preexisting arthritis of the ipsilateral hip increases a patient’s risk of conversion independent of their age. To minimize patient risk exposure and maximize overall quality of surgical care, it is important to discuss a patient’s risk of requiring conversion THA after an HA procedure and to establish a treatment plan through shared decision-making.
Footnotes
Appendix
Diagnosis Codes Used to Identify Patients With Obesity, Tobacco Use History, and Hip Osteoarthritis a

| Classification System | Diagnosis Code |
|---|---|
| Obesity | |
| ICD-9-CM | 278.0, Obesity |
| ICD-10-CM | E66.X (where X is any number), Obesity |
| Tobacco use | |
| ICD-9-CM | 305.1, Tobacco use disorder |
| V15.82, History of tobacco use | |
| 64900, Tobacco use disorder-unspecified | |
| 98984, Toxic effect of tobacco | |
| ICD-10-CM | F17.200, Nicotine dependence, unspecified, uncomplicated |
| F17.201, Nicotine dependence, unspecified, in remission | |
| F17.210, Nicotine dependence, cigarettes, uncomplicated | |
| F17.211, Nicotine dependence cigarettes, in remission | |
| F17.220, Nicotine dependence, chewing tobacco, uncomplicated | |
| F17.221, Nicotine dependence, chewing tobacco, in remission | |
| F17.290, Nicotine dependence, other tobacco products, uncomplicated | |
| F17.291, Nicotine dependence, other tobacco products, in remission | |
| Z87.891, Personal history of nicotine dependence | |
| Hip osteoarthritis | |
| ICD-9-CM | 715.15, Osteoarthrosis, localized, primary, pelvic region, and thigh |
| 715.25, Osteoarthrosis, localized, secondary, pelvic region, and thigh | |
| 715.35, Osteoarthrosis, localized, not specified whether primary or secondary, pelvic region, and thigh | |
| 715.95, Osteoarthrosis, unspecified whether generalized or localized, pelvic region, and thigh | |
| ICD-10-CM | M16.XX (where XX is any number), Osteoarthritis of the hip |
CM, clinical modification; ICD, International Classification of Diseases.
Final revision submitted July 6, 2023; accepted July 31, 2023.
One or more of the authors has declared the following potential conflicts of interest or sources of funding: S.G.A. has received education payments from Gotham Surgical Solutions & Devices; consulting fees from Smith & Nephew; and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.