
Abstract
Background:
The Kerlan-Jobe Orthopaedic Clinic shoulder and elbow score (KJOC) is sensitive enough to detect subtle changes in the functional level of the shoulder or elbow in overhead athletes. However, a Japanese version of the KJOC is not yet available. Moreover, the original KJOC uses a visual analog scale (VAS) assessment format that requires a print version so that users can add a check mark along a horizontal line. The KJOC can be completed using online tools such as Google Forms if a 10-point scale format can be used with comparable results.
Purposes:
To (1) translate and cross-culturally adapt the KJOC into Japanese (KJOC-J) and assess its validity and (2) evaluate the correlation between a standard VAS format and a 10-point scale format (KJOC-J10).
Study Design:
Cohort study (Diagnosis); Level of evidence, 3.
Methods:
In total, 318 athletes participated in the validation study, 255 in the test-retest reliability study for the KJOC-J, and 273 in the validation study for the KJOC-J10. Internal consistency was evaluated using the Cronbach alpha. Validity was evaluated by calculating the correlation between the KJOC-J and the Disability of the Arm, Shoulder and Hand (DASH). Test-retest reliability was assessed using the intraclass correlation coefficient (ICC). The validity of the KJOC-J10 was evaluated by calculating the correlation between the KJOC-J10 and KJOC-J.
Results:
The Cronbach alpha was 0.914, indicating good internal consistency. The KJOC-J was moderately correlated with the DASH (r = −0.581; P < .001) and had good test-retest reliability (ICC, 0.874). A strong correlation was found between the KJOC-J and KJOC-J10 (r = 0.846; P < .001).
Conclusion:
The study results demonstrated good internal consistency, validity, and reliability for the KJOC-J, indicating that it is a valid assessment tool for shoulder and elbow functions in Japanese overhead athletes. Moreover, a strong correlation was found between the VAS and 10-point formats of the KJOC-J.
Self-reported outcome measures can decrease the discrepancy between physical examination outcomes and subjective patient assessments, determine treatment outcomes, and screen for the risk of injuries. The Kerlan-Jobe Orthopaedic Clinic shoulder and elbow score (KJOC) was developed in 2010 to evaluate function in overhead athletes. 1 The KJOC consists of 10 items, and the mean of these items is calculated and used to evaluate the subjective functional status of the shoulder or elbow in overhead athletes. Since the KJOC was introduced, several studies have used this measure for overhead athletes participating in baseball, tennis, softball, and swimming.5,7,9,15,16,21,23 Furthermore, the KJOC is sufficiently sensitive to detect slight changes in the functional level of the shoulder or elbow in overhead athletes5,7,16 and is associated with in-season injury risk in female softball players. 9 Because these previous studies support the efficacy of the KJOC,5,7,9,16 the original English version has been translated and validated in several languages, such as German, Italian, Korean, Norwegian, Turkish, Persian, and Dutch.8,12-14,17,19,22 However, a Japanese version of the KJOC is not yet available.
Translation and cross-cultural adaptation procedures are necessary to utilize questionnaires with speakers of other languages. Since Beaton et al 3 introduced the guidelines for the cross-cultural adaptation of self-reported outcome measures, several researchers have followed these guidelines and translated various questionnaires into other languages.10,11 These guidelines have also been used when translating the KJOC into other languages.8,13,14,17,19,22 Moreover, the validity of the KJOC has been demonstrated by comparing it with the Disability of the Arm, Shoulder and Hand score (DASH), both in the original English version 1 and in several translations of the KJOC.8,12,13,17,19,22 A Japanese version of the DASH is available. 10
The original KJOC uses a visual analog scale (VAS) to assess shoulder and elbow function. 1 However, using the VAS assessment format may limit the widespread use of various questionnaires, as this type of assessment requires a printed version for the user to write a check mark along the horizontal line. If an interval scale format is used instead, the KJOC could be completed through online tools such as Google Forms (Google Inc.).
In the present study, we aimed to translate and cross-culturally adapt the KJOC into Japanese (KJOC-J) and assess its validity. In addition, we aimed to evaluate the correlation of the KJOC-J between a standard VAS format and a 10-point interval scale format (KJOC-J10).
Methods
Translation and Cross-cultural Adaptation
The protocol for this study was approved by our ethics committee. Before obtaining the data, the purpose and procedures were carefully explained to the participants, and informed consent was obtained. According to the guidelines of Beaton et al, 3 the process of translation and cross-cultural adaptation was separated into 5 stages as follows: (1) forward translation; (2) synthesis of the translations; (3) back translation; (4) expert committee meeting; and (5) testing of the prefinal version.
Forward Translation
Two Japanese-English bilingual individuals from different backgrounds translated the original English version of the KJOC into Japanese. The informed translator (first translator: H.Y.) was a physical therapist who had studied abroad for 3 years in the United States, whereas the uninformed translator (second translator) was an economics specialist. The first and second translators provided translations T1 and T2, respectively.
Synthesis of the Translations
T1 and T2 were compared and reviewed in a group meeting to resolve all inconsistencies between the 2 versions, providing a synthesized KJOC-J (KJOC-J T-1-2). The synthesizing group consisted of 3 Japanese-English bilingual physical therapists (T.I., H.Y., and H.A.) with >10 years of experience in orthopaedic and sports rehabilitation.
Back-Translation
Two native English speakers without medical backgrounds who could read Japanese translated the KJOC-J T-1-2 into English. The first and second back-translators were not informed of the original KJOC and provided back-translations BT1 and BT2, respectively.
Expert Committee Meeting
The expert committee comprised a professional linguist (A.T.) and bilingual sports medicine researchers (T.I., H.Y., H.A., and M.E.). The committee members reviewed and synthesized all translations (T1, T2, T-1-2, BT1, and BT2), as well as the original version of the KJOC, to reach a consensus on any discrepancy and obtain conceptual equivalence between the original and Japanese versions of the KJOCs. Consequently, the expert committee obtained a prefinal version of the KJOC-J.
Testing of the Prefinal Version of the KJOC-J
In the pretest, 22 college tennis players completed the prefinal version of the KJOC-J. Subsequently, the athletes were interviewed regarding their thoughts and the reason for selecting their response for every item. The expert committee members reviewed the pretest results and acquired comments to achieve the final adaptation of the questionnaire. After addressing any discrepancies and achieving agreement among the committee members, the final version of the KJOC-J was approved by the expert committee. This version is available separately (see Supplemental Material).
Participant Recruitment
The participants were recruited from several college sports clubs and an orthopaedic hospital. Our participants were both amateur and professional athletes. The inclusion criteria were as follows: (1) native Japanese speakers; (2) age >18 years; and (3) belonging to sports clubs, such as baseball, basketball, tennis, softball, swimming, volleyball, and throwing events (ie, javelin, discus, and shot put). With regard to the nonscored question in the KJOC about the current status of athletes, we categorized athletes who were playing without any arm trouble as asymptomatic and athletes who were playing with arm trouble or not playing due to arm trouble as symptomatic.
Procedures
The participants completed the KJOC-J and the DASH on the same day as the first test session to evaluate internal consistency and validity. In line with studies that translated and validated the KJOC into other languages,8,12-14,17,19,22 the participants were instructed to complete the KJOC-J again approximately 2 weeks after the first session to evaluate the test-retest reliability. In the second session, the participants simultaneously completed the KJOC-J10 using Google Forms.
Internal Consistency
Internal consistency was evaluated by calculating the Cronbach alpha to measure the degree of homogeneity of the 10 items of the KJOC-J, with an alpha value between 0.70 and 0.90 indicating good internal consistency. 20
Validity
The validity of the KJOC-J was evaluated by calculating the correlation coefficient between the KJOC-Js and the DASH (0-100: 0 indicating no disability, and 100 indicating the worst disability). The validity of the KJOC-J10 was evaluated by calculating the correlation coefficients between the KJOC-J10 and KJOC-Js obtained in the second session. According to previous studies,13,18 the correlation coefficients were categorized as follows: very strong, 0.90-1.00; strong, 0.70-0.89; moderate, 0.40-0.69; weak, 0.10-0.39; and negligible, 0.00-0.10.
Test-Retest Reliability
To evaluate the test-retest reliability, the intraclass correlation coefficient (ICC), with corresponding 95% CI for the mean score and the score of each item, was calculated using the data obtained in the first and second sessions. According to a previous study, 19 ICC values were categorized as follows: excellent, >0.90; good, 0.75-0.90; moderate, 0.50-0.75; and poor, <0.50. Furthermore, the standard error of measurement (SEM) and the minimum detectable change (MDC) were calculated using the following formulas:


A Bland-Altman plot (95% limits of agreement) was constructed by plotting the mean difference between the test and retest KJOC-Js against the mean of the 2 measures. 2
Statistical Analyses
Descriptive data were reported as mean ± standard deviation. All statistical analyses were performed using SPSS Statistics Version 29 (IBM Corp). The normality of all measures was evaluated using the Shapiro-Wilk test. The validity of the KJOC-J and KJOC-J10 was assessed using either the Pearson correlation coefficient or the Spearman rank correlation coefficient depending on normality. Statistical significance was set at P < .05.
Results
Internal Consistency and Validity of the KJOC-J
To examine internal consistency and validity, 318 athletes were asked to complete the KJOC-J and DASH in the first session. The characteristics of these participants are presented in Table 1. The KJOC-J showed good internal consistency, with a Cronbach alpha of 0.914.
Participant Characteristics for the Validation Study of the KJOC-J a

Data are presented as No. of athletes or mean ± standard deviation. DASH, Disabilities of the Arm, Shoulder and Hand; F, female; KJOC-J, Kerlan-Jobe Orthopaedic Clinic-Japanese; M, male.
Javelin, discus, and shot put.
As normality was not confirmed using the Shapiro-Wilk test, the correlation between the KJOC-J and the DASH was evaluated using the Spearman rank correlation test. The KJOC-J was found to be moderately correlated with the DASH (r = −0.581 [95% CI, –0.652 to −0.501]; P < .001).
Test-Retest Reliability
The demographic data for the study of test-retest reliability are shown in Table 2. Of all the athletes who completed the KJOC-J in the first session, 63 did not complete the retest questionnaire because of scheduling conflicts and changes in their upper extremity status. The test-retest reliability was investigated using the mean score and each scoring item of the KJOC-J (Table 3). The reliability of the mean KJOC-J was categorized as good. In addition, each item showed good to moderate reliability, except for items 1 and 5. The Bland-Altman plot (Figure 1) indicated no correlation between the difference and the mean of the test-retest measurements. The mean difference of the KJOC-J was −1.8 ± 6.5 (95% CI, –14.6 to 11.0).
Participant Characteristics for the Test-Retest Reliability Analysis of the KJOC-J a

Data are presented as No. of athletes or mean ± standard deviation. F, female; KJOC-J, Kerlan-Jobe Orthopaedic Clinic-Japanese; M, male.
Javelin, discus, and shot put.
Results of the Test-Retest Reliability Analysis of the KJOC-J a

Data are presented as mean ± standard deviation unless otherwise indicated. ICC, intraclass correlation coefficient; KJOC-J, Kerlan-Jobe Orthopaedic Clinic-Japanese; MDC, minimum detectable change.

Bland-Altman plot showing the test-retest outcomes of the KJOC-J. Dashed lines indicate 95% limits of agreement. KJOC-J, Kerlan-Jobe Orthopaedic Clinic-Japanese.
Validity of the KJOC-J10
The demographic data for the validation of the KJOC-J10 are shown in Table 4. In the second session, 18 additional athletes simultaneously completed the KJOC-J and KJOC-J10. The correlation between the KJOC-J and KJOC-J10 was evaluated using the Spearman rank correlation, and the results are shown in Table 5. The results demonstrated that the mean score and most individual score items showed a strong correlation between the VAS and the 10-point scale format of the KJOC-J. Only item 5 showed a moderate correlation between the different questionnaire formats.
Participant Characteristics for the Validation Study of the KJOC-J10 a
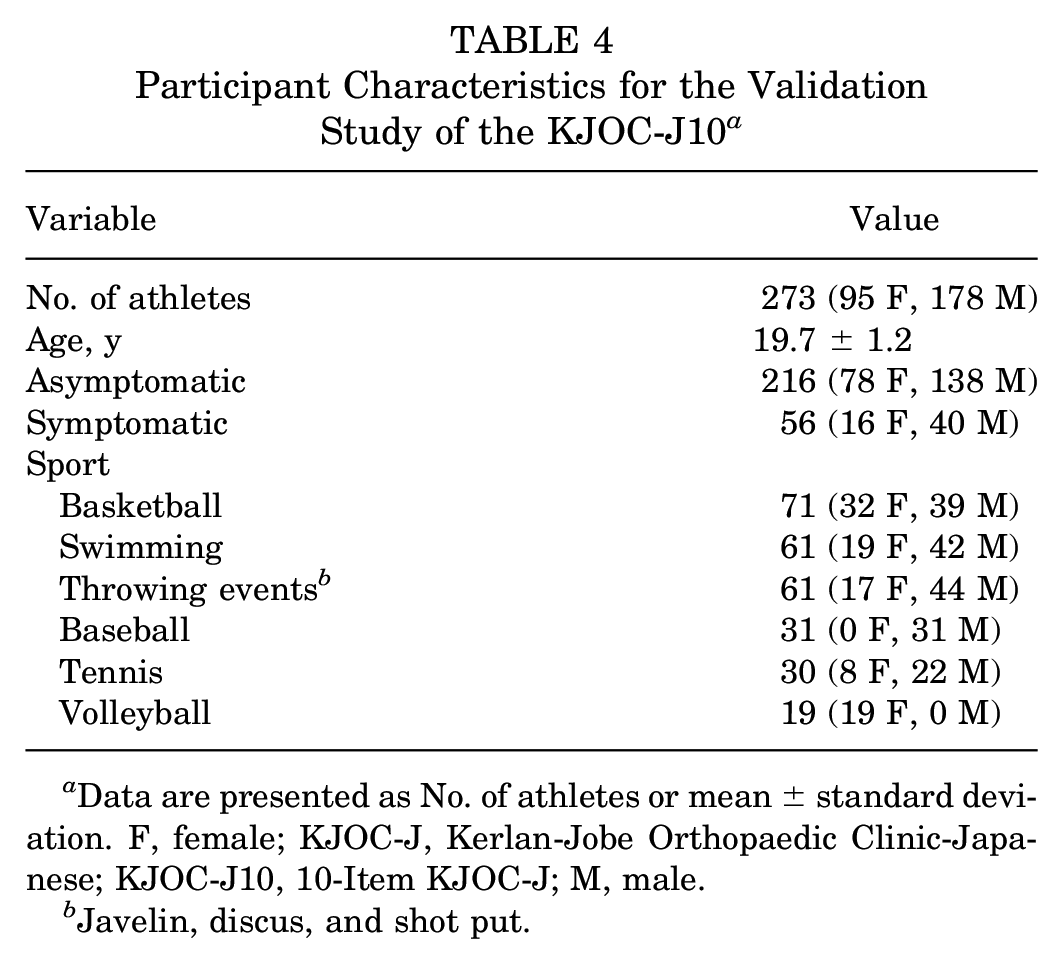
Data are presented as No. of athletes or mean ± standard deviation. F, female; KJOC-J, Kerlan-Jobe Orthopaedic Clinic-Japanese; KJOC-J10, 10-Item KJOC-J; M, male.
Javelin, discus, and shot put.
Results of the Validation Study of the KJOC-J10 a

Data are presented as mean ± standard deviation unless otherwise indicated. ICC, intraclass correlation coefficient; KJOC-J, Kerlan-Jobe Orthopaedic Clinic-Japanese; KJOC-J10, 10-Item KJOC-J; VAS, visual analog scale.
P < .001 for all ICC values.
Discussion
The KJOC-J showed good internal consistency, constructive validity, and test-retest reliability. Therefore, the study findings suggest that the KJOC-J is a valid subjective assessment tool for evaluating shoulder and elbow function in Japanese overhead athletes. Moreover, a strong correlation was found between the VAS and 10-point formats of the KJOC-J, implying that the 10-point scale format may be just as applicable as the VAS format.
The Cronbach alpha values indicated that the KJOC-J had good internal consistency. This result is consistent with those of previous studies.8,10,11,13,14,17,19,22 In addition, the correlation coefficient between the KJOC-J and the DASH demonstrated that the constructive validity of the KJOC-J was moderate (r = −0.581). This result is also in line with the findings of previous studies comparing the KJOC in other languages to the DASH.8,12-14,19,22 In contrast, the original English version 1 of the KJOC showed a strong correlation with the DASH (r = 0.84). This discrepancy between the present study and previous study by Alberta et al 1 may be attributed to the participants’ status and the sensitivity of the DASH. The mean DASH value was 1.9 in all participants and 6.9 (range, 0-30.8) in symptomatic athletes. The MDC for the DASH ranged from 10.81 to 17.23 in previous studies.4,6 Additionally, most items in the DASH have been designed to evaluate functional impairment in daily living and not the specific demands of overhead athletes. 8 Thus, our symptomatic athletes may have shown little functional impairment in their daily lives, although they had upper extremity problems during overhead activities. Therefore, the functional status of our participants was not adequately evaluated using the DASH, which may have resulted in the discrepancy between the present and previous studies regarding the correlation between the KJOC and the DASH. In other words, the results suggest that the KJOC would be sufficiently sensitive to assess changes in the functional status of the affected upper extremities in overhead athletes with few functional limitations in daily activities. This hypothesis is supported by previous studies demonstrating that the KJOC is sufficiently sensitive to detect subtle changes in shoulder or elbow function levels in overhead athletes.5,7,16
The KJOC-J showed good test-retest reliability in the present study, which is consistent with that in previous studies on the translation of the original KJOC into other languages.8,13,14,19,22 Test-retest reliability in this study was also on the same level as the previous study by Alberta et al 1 (ICC, 0.87 for the present study; ICC, 0.88 for the original study). Furthermore, most items of the KJOC-J showed moderate to good reliability. Therefore, we conclude that the KJOC-J is a reliable tool for evaluating arm status in overhead athletes. However, items 1 and 5 showed poor test-retest reliability. Item 5 assesses the effect of arm problems on relationships with coaches, management, and agents. The German version of the KJOC also reported poor reliability for item 5; half of the participants were amateur-level athletes. 19 Most participants in this study were amateur athletes and did not have contracts like professional players. Given the participants’ characteristics in the previous German study 19 and the present study, competitive level with or without contraction might have affected the results of item 5. In contrast, we could not provide a reasonable explanation for the poor reliability of item 1, which relates to difficulty in getting loose or warm before competition or practice. The present results imply that responses of the upper extremities to warmups may change within a short period, and the physical response to warmups may reflect the physiological status of athletes. Thus, future studies are warranted to investigate the time-dependent changes in the response to warmups in overhead athletes and their relationship with the risk of shoulder and elbow injuries.
The original KJOC uses the VAS format because it seems more sensitive to changes in the participants’ status than a Likert-type scale. 1 Results of the correlation analysis between the VAS and 10-point scale formats of the KJOB-J indicated that the total score and most score items (except for item 5) showed strong associations between the formats. Adapting the KJOC into the 10-point format may allow more widespread usage through digital application tools such as Google Forms. However, the sensitivity of the 10-point assessment of the KJOC score is unknown, whereas the KJOC in its current VAS format has shown high sensitivity for detecting subtle changes in shoulder and elbow functions in overhead athletes.5,7 Considering that the MDC of the KJOC-J was 13.2 in the present study, the 10-point scale format may not allow for detecting slight changes in shoulder and elbow function. Future studies are necessary to compare the sensitivity of the KJOC between the VAS and the 10-point formats.
Limitations
This study has some limitations. First, the specific characteristics of the study population, which comprised professional and amateur athletes, might have affected the outcomes of the KJOC-J. Second, the sensitivity of the KJOC-J and KJOC-J10 is unclear; thus, future prospective studies are necessary to investigate time-dependent changes in the KJOC-J in overhead athletes. Third, the simultaneous completion of the KJOC-J and KJOC-J10 scores may have affected the results of the correlation analysis if participants attempted to match their responses between the 2 versions. Fourth, although free online tools—such as Google Forms—only provide a 10-point scale, using a 100-point scale instead of a 10-point scale might improve interchangeability between KJOC-J and KJOC-J10 scores. Finally, most of our participants were basketball and swimming athletes. This selection bias should be noted when interpreting the present results.
Conclusion
The study results demonstrated good internal consistency, validity, and reliability of the KJOC-J, indicating that it is a valid assessment tool for shoulder and elbow functions in Japanese overhead athletes. Moreover, a strong correlation was found between the VAS and 10-point formats of the KJOC-J.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241291861 – Supplemental material for Translation and Cross-cultural Adaptation of the Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Score Into Japanese and Comparison of Visual Analog Scale and 10-Point Scale Formats
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241291861 for Translation and Cross-cultural Adaptation of the Kerlan-Jobe Orthopaedic Clinic Shoulder and Elbow Score Into Japanese and Comparison of Visual Analog Scale and 10-Point Scale Formats by Tomonobu Ishigaki, Hirotake Yokota, Hiroshi Akuzawa, Noriko Akiho-Toyoda, Keisuke Ushiro, Yuki Ebihara, Shigeharu Tanaka, Tadashi Wada, Hirofumi Jigami, Hisashi Matsumoto, Yu Ito, Takanori Kikumoto, Yuiko Matsuura, Ryo Hirabayashi, Chie Sekine, Noriaki Yamamoto, Go Omori and Mutsuaki Edama in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank the translators for their assistance. They also appreciate Dr Shintaro Sato, Dr Daisuke Sugimoto, and Mr Suguru Ohta for introducing the translators.
Final revision submitted April 6, 2024; accepted April 29, 2024.
Authors
Tomonobu Ishigaki, PT, PhD (Athlete Support Research Center, Niigata University of Health and Welfare, Niigata City, Niigata, Japan; Institute for Human Movement and Medical Sciences, Niigata University of Health and Welfare, Niigata, Japan; Institute of Life Innovation Research Center, Toyo University, Tokyo, Japan); Hirotake Yokota, PT, PhD (Athlete Support Research Center, Niigata University of Health and Welfare, Niigata, Japan; Institute for Human Movement and Medical Sciences, Niigata University of Health and Welfare, Niigata, Japan); Hiroshi Akuzawa, PT, PhD (Athlete Support Research Center, Niigata University of Health and Welfare, Niigata, Japan; Institute for Human Movement and Medical Sciences, Niigata University of Health and Welfare, Niigata, Japan); Noriko Akiho-Toyoda, MA (Student Support Organization, Niigata University of Health and Welfare, Niigata, Japan); Keisuke Ushiro, MS (Faculty of Physical Education, Department of Sports and Physical Education, Kokushikan University, Tama, Tokyo, Japan); Yuki Ebihara, MS (Faculty of Physical Education, Department of Sports and Physical Education, Kokushikan University, Tama, Tokyo, Japan); Shigeharu Tanaka, PhD (Faculty of Physical Education, Department of Sports and Physical Education, Kokushikan University, Tama, Tokyo, Japan); Tadashi Wada, PhD (School of Science and Engineering, Human Informatics Course, Kokushikan University, Tokyo, Japan); Hirofumi Jigami, PT, PhD, JSPO-AT, (School of Science and Engineering, Human Informatics Course, Kokushikan University, Tokyo, Japan); Hisashi Matsumoto, PT, JSPO-AT (Department of Rehabilitation, Orthopaedic Hokushin Hospital, Sapporo, Japan); Yu Ito, PT, MS, JSPO-AT (Department of Rehabilitation, Orthopaedic Hokushin Hospital, Sapporo, Japan); Takanori Kikumoto, PT, PhD, JSPO-AT (Athlete Support Research Center, Niigata University of Health and Welfare, Niigata, Japan; Institute for Human Movement and Medical Sciences, Niigata University of Health and Welfare, Niigata, Japan); Yuiko Matsuura, PT, PhD, JSPO-AT (Athlete Support Research Center, Niigata University of Health and Welfare, Niigata, Japan; Institute for Human Movement and Medical Sciences, Niigata University of Health and Welfare, Niigata, Japan); Ryo Hirabayashi, PT, PhD (Athlete Support Research Center, Niigata University of Health and Welfare, Niigata, Japan; Institute for Human Movement and Medical Sciences, Niigata University of Health and Welfare, Niigata, Japan); Chie Sekine, PT, PhD, JSPO-AT (Athlete Support Research Center, Niigata University of Health and Welfare, Niigata, Japan; Institute for Human Movement and Medical Sciences, Niigata University of Health and Welfare, Niigata, Japan); Noriaki Yamamoto, MD, PhD (Institute for Human Movement and Medical Sciences, Niigata University of Health and Welfare, Niigata, Japan; Department of Orthopedic Surgery, Niigata Rehabilitation Hospital, Niigata, Japan); Go Omori, MD, PhD (Athlete Support Research Center, Niigata University of Health and Welfare, Niigata, Japan); Mutsuaki Edama, PT, PhD, JSPO-AT (Athlete Support Research Center, Niigata University of Health and Welfare, Niigata, Japan; Institute for Human Movement and Medical Sciences, Niigata University of Health and Welfare, Niigata, Japan).
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was received from the Project for Establishment of Sports Medicine and Science Support System in Local Communities 2023 through the Japan Sports Agency. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Niigata University of Health and Welfare (reference No. 19002-230209).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.