
Abstract
Background:
Anterior cruciate ligament injury poses a major effect on the quality of life of patients. Anterior cruciate ligament reconstruction (ACLR) remains the mainstay of treatment.
Purposes:
To (1) test for the correlation of patients’ characteristics such as body mass index (BMI), age, smoking status, and postoperative infrapatellar numbness with the subjective outcome of primary ACLR and (2) investigate whether postsurgical complications can be related to the studied patients’ characteristics.
Study Design:
Case series; Level of evidence, 4.
Methods:
Demographic data and operational notes from patients who underwent primary ACLR at the institute between 2011 and 2022 were extracted. Patients’ surgical outcomes were evaluated subjectively using the International Knee Documentation Committee (IKDC) score and the Knee injury and Osteoarthritis Outcome Score (KOOS). Pre- and postoperative scoring were completed at postoperative follow-up in December of 2022, patients completed both the IKDC and the KOOS questionnaires. Patients were asked to rate their knee function out of 10 before and after surgery. This rating was based on the patients’ self-assessment of their functional ability without the use of a formal instrument. Knee function was assigned as better, worse, or the same through a comparison of patients’ reported scores before and after surgery.
Results:
Male patients comprised 108 (98.2%) of the total cohort, the mean ± SD age at the time of surgery was 27.92 ± 7.39 years, and BMI was 26.54 ± 3.89. The mean follow-up time was 48.92 ± 27.99 months. Most patients did not need postsurgical intervention (n = 97; 88.2%), while 4 (3.6%), 7 (6.4%), and 2 (1.8%) needed revision, debridement, or both, respectively. The mean IKDC score and KOOS, respectively, were 74.37 ± 20.17 and 85.50 ± 14.83. Patients’ BMI had a significant effect on IKDC score (74.68 ± 20.0; P < .001), and infrapatellar numbness after surgery also affected patients’ IKDC score (P = .002) and KOOS (P = .043). The age at the time of ACLR was associated with contralateral leg surgery (P = .017).
Conclusion:
This study showed that higher BMI and infrapatellar numbness negatively affect the subjective outcomes after primary ACLR. Older age at the time of primary ACLR was associated with a higher likelihood of surgery in the contralateral leg.
Keywords
Anterior cruciate ligament (ACL) injury is a serious knee injury and can have a major effect on the quality of life of patients. 15 ACL reconstruction (ACLR) is the preferred treatment option.9,27 ACLR represents about 80% of all knee ligament surgeries and is still the primary approach for young, active individuals experiencing this injury. 29
Many scoring systems have been developed to evaluate patient-related outcomes after ACLR. The Knee injury and Osteoarthritis Outcome Score (KOOS) and International Knee Documentation Committee (IKDC) score are 2 examples of the most used scoring systems.13,27 The outcome of ACLR can depend on many patient-related factors and other surgical technique–related factors. 8 There is conflicting evidence regarding the influence of age, sex, and time interval between injury and surgery on outcomes.2,8,12,30,35 A retrospective study reported a positive correlation between age and time interval from injury to surgery with the incidence of contralateral ACLR after 5 years of primary ACLR. 7 Patients with lower baseline physical activity and greater body mass index (BMI) have been reported to have worse outcomes.8,30 Previous studies showed that individuals who smoked and underwent ACLR had worse outcomes and an elevated incidence of complications postoperatively.8,12,25,26 Two cohort studies reported that graft diameter used during ACLR didn’t affect the outcome of surgery and the rates of revision.2,32
Complications may arise postoperatively in relation to some factors and can be predictors of a reduction in IKDC and KOOS scores, indicating a decline in knee function and patient-reported outcomes. Numbness at the infrapatellar aspect of the knee was a frequently reported complaint after primary ACLR by a randomized clinical trial 24 and a prospective study. 6
Although some studies3,12 have investigated how factors such as demographics (e.g., age, sex, and BMI) affect the outcomes of primary ACLR, the literature lacks a study that explores the impact of these variables, along with postoperative complications, on subjective ACLR outcomes (IKDC/KOOS). Therefore, we aimed to investigate the relationship between patient characteristics, postoperative complications, and surgical outcomes of primary ACLR, as measured by the IKDC and KOOS.
Methods
Patients and Study Design
This is a retrospective study of factors (e.g. BMI, smoking status) affecting primary ACLR surgery outcomes and postsurgical complications (e.g. patellar numbness). It was conducted on patients who underwent primary ACLR at our institute in Jordan between January 2011 and July 2022. All patients underwent arthroscopic primary ACLR with hamstring tendon autograft harvested via vertical anteromedial incision.
Eligibility criteria were as follows: patients between 15 and 40 years of age with ACL injury identified on magnetic resonance imaging by an orthopaedic surgeon and who underwent primary ACLR (M.Alkhatatba) at our institute. Patients with previous knee surgery, injury to other ligaments, revision surgery, and generalized laxity (defined by Beighton score ≥5) 22 were excluded from the study. Figure 1 shows the flowchart of eligible participants for this study.

Flowchart for the screening process. *Patients with previous knee surgery, injury to other ligaments, revision of surgery, generalized joint laxity, or no contact information.
After institutional review board approval, data were collected using patients’ records and intraoperative notes. These data included patients’ age at the time of surgery, current age, sex, BMI, smoking status, the pattern of ACL injury (which was identified during arthroscopy at the time of ACLR to be either a partial or complete tear of the ACL), whether it was associated with a meniscal injury, the time interval between injury and surgery, the size of graft used in reconstruction, and follow-up period.
Postoperative follow-up for all patients was carried out in the first week of December 2022. Contact was attempted exclusively via telephone, and if no response was received, up to three attempts were made before patients were excluded from the study. After successful contact, patients were asked to fill out the IKDC and KOOS forms, which were then emailed to us upon completion.
During follow-up, we asked patients yes/no questions about whether they experienced specific complications, such as the need for any other surgical interventions. If they answered ’yes,’ we confirmed the reported complications by reviewing their medical records to ensure accuracy. Specifically, patients were asked about the need for other interventions after the initial reconstruction (such as revision in case of ACLR failure, debridement in case of infection), whether a contralateral leg surgery was conducted, and if they had any complaints of infrapatellar numbness.
We asked patients to subjectively rate their knee function on a scale of 0 to 10, where 0 represents the inability to perform daily activities, and 10 reflects normal/excellent knee function. This rating was based on the patients’ self-assessment of their functional ability. We subtracted their preoperative scores from their postoperative scores. Based on the resulting score, patients were classified into 3 groups of knee function: better (positive change, score >0), worse (negative change, score <0), and unchanged (score = 0).
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics (Version 27; IBM). Frequencies and percentages were used to report categorical data, while continuous variables were reported using mean ± SD. Mean differences between continuous data were evaluated using independent-samples t test, analysis of variance, or their equivalent nonparametric test. Categorical data were analyzed using chi-square or Fisher exact test. Pearson correlation coefficient and Spearman rank coefficient were used to correlate continuous variables. Missing data were pairwise excluded. P≤ .05 was deemed significant.
Results
A total of 110 patients were included in this study. Most patients were male (n = 108; 98.2%). Mean ± SD age overall was 27.92 ± 7.39 years at the time of surgery and 31.65 ± 7.96 years at follow-up. Mean BMI at the time of surgery was 26.54 ± 3.89, and 59 patients (53.6%) were smokers. Most patients had a complete ACL injury (n = 102; 92.7%), and 72 patients (65.5%) had an associated meniscal injury. The time interval between injury and reconstruction was 18.37 ± 28.06 months, while the mean follow-up time was 48.92 ± 27.99 months (range [minimum, maximum] = 137.17 months [5.52, 142.69 months]). The mean graft diameter was 7.5 ± 0.63 mm in size. Patient demographics are presented in Table 1. Bivariate analysis of demographics and subjective scoring systems showed a significant correlation between BMI and IKDC score (74.68 ± 20.0; P < .001) but no statistically significant correlation with KOOS (85.79 ± 14.58; P = .074). Other patient characteristics did not show a significant correlation with either IKDC score or KOOS (Table 1).
Patient Characteristics by Mean IKDC Score and KOOS (N = 110) a

BMI, body mass index; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score.
One case missing (n = 109).
Upon classifying patients by their postsurgical knee function, the BMI of patients with better knee function after surgery (26.27 ± 3.86) did not statistically differ from patients with worse or unchanged knee function (27.95 ± 3.61 and 28.37 ± 4.52, respectively) (P = .217). Table 2 demonstrates the difference in knee function after surgery by patient demographics. Mean IKDC score and KOOS, respectively, were statistically different among patients with better (77.68 ± 18.21 and 87.54 ± 12.92), worse (62.10 ± 20.34 and 79.06 ± 15.30), and unchanged (45.42 ± 20.10 and 65.68 ± 24.77) knee function after surgery (P < .001 and P = .012 for IKDC and KOOS, respectively) (Figure 2).
Patient Characteristics by Knee Function After Surgery (N = 110) a

BMI, body mass index; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score.
One case missing (n = 109).

Bar chart of International Knee Documentation Committee (IKDC) score and Knee injury and Osteoarthritis Outcome Score (KOOS) based on knee function after surgery.
Most patients did not need postsurgical intervention (n = 97; 88.2%), while 4 patients (3.6%) underwent surgical revision, 7 (6.4%) underwent debridement, and 2 (1.8%) had both revision and debridement. In addition, 15 patients (13.6%) had surgery in the contralateral leg. A total of 41 patients (37.3%) complained of infrapatellar numbness after reconstruction, and 22 (20%) complained of giving way. Table 3 lists patient postoperative complications. There was a significant difference in IKDC score and KOOS between patients who complained of infrapatellar numbness (67.15 ± 19.55 and 82.44 ± 14.86, respectively) and those who did not (78.65 ± 19.43 and 87.33 ± 14.62) (P = .002 and .043 for IKDC and KOOS, respectively). Other postoperative complications (postsurgical intervention, contralateral leg surgery) were not significantly associated with either the IKDC score (P = .890 and .709, respectively) or KOOS (P = .493 and .671, respectively).
Patient Postsurgical Complications by Mean IKDC Score and KOOS (N = 110) a
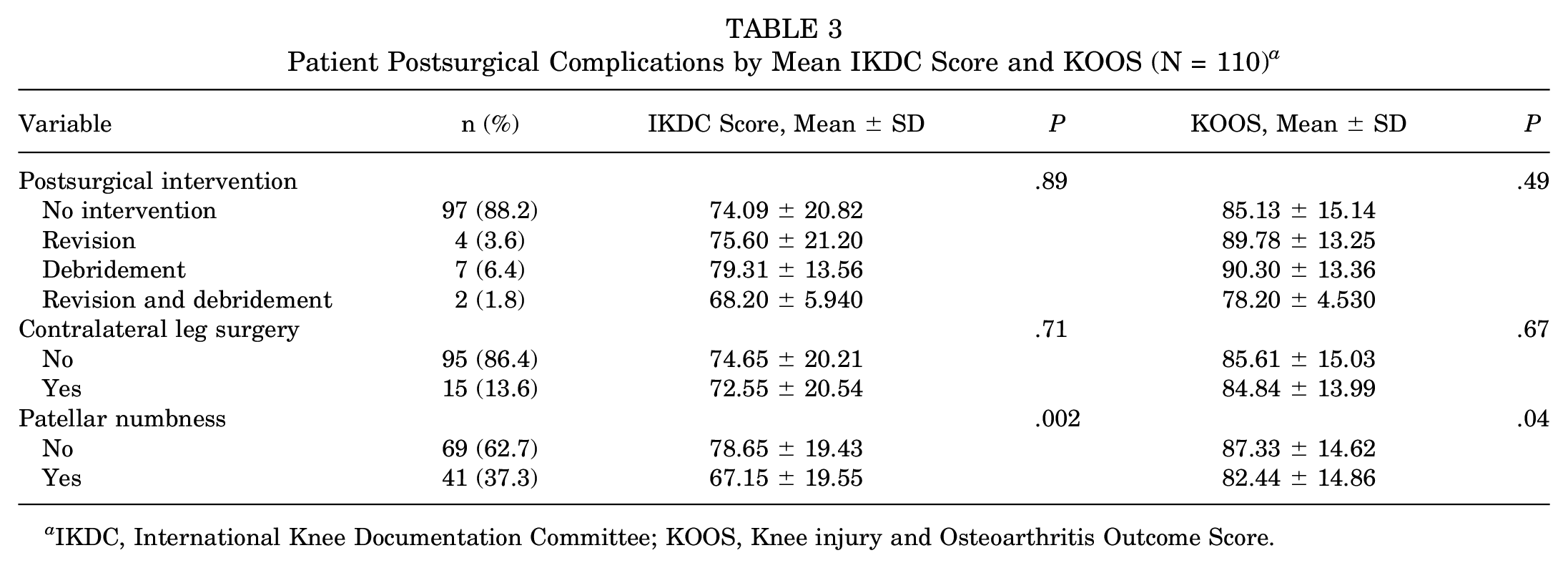
IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score.
Finally, Table 4 associates patient demographics with their postoperative complications. Whether or not a patient smoked significantly influenced whether the patient needed intervention after reconstruction (smokers: n = 1 [7.7%]; nonsmokers: n = 12 [92.3%]) or no intervention (smokers: n = 58 [59.8%]; nonsmokers: n = 39 [40.2%]) (P < .001). The need for a contralateral leg surgery after primary ACLR was significantly affected by the patient’s age at the time of surgery (P = .017). Other patient demographics did not correlate significantly with their reported complications. Figure 3 visualizes the relationship between age at the time of surgery and meniscal injury (P = .411) and the effect of timing from injury to surgery on developing meniscal injury (P = .173).
Patient Characteristics by Surgical Complications (N = 110) a

Data presented as n (%) or mean (SD). BMI, body mass index.
Includes patient who underwent revision, debridement, or both.
One missing case (n = 109).

Effect of age at time of surgery on the chance of developing meniscal injury compared with the timing from injury to surgery. The red line indicates the difference in the mean time interval from injury to surgery between patients who sustained a meniscal injury and those who did not sustain a meniscal injury.
Discussion
This retrospective study followed patients who underwent primary ACLR for a mean of 49 months. We observed that greater BMI and infrapatellar numbness were associated with lower subjective outcome scores. Furthermore, patients’ age at the time of primary ACLR was positively correlated with the likelihood of surgery in the contralateral knee. Age at surgery, time from injury to surgery, and graft diameter were not associated with a change in subjective outcomes.
In this study, a greater BMI was found to be significantly associated with a lower IKDC score after primary ACLR surgery. However, it was not found to influence how the patients perceived their knee function before and after surgery. In the study by Kowalchuk et al, 17 obesity (BMI >25) was associated with a lower IKDC score. However, Ballal et al 3 found no significant difference in outcome between normal and high BMI in patients after primary ACLR. This variability may be explained by the difference in follow-up period lengths between our study (48.92 months) and their study (≥24 months). Due to the contradictory results in the literature, the relationship between BMI and outcome after primary ACLR needs more exploration.
Infrapatellar numbness is a commonly reported finding in patients after ACLR due to injury to the infrapatellar branch of the saphenous nerve during surgery.6,16 A prospective study reported that a greater incidence of infrapatellar numbness was noted in patients who had hamstring tendon grafts compared with quadriceps tendon grafts. 31 Cohen et al 6 found that the numbness decreased with time after surgery, with sensation completely restored in some patients. In this study, even though our mean follow-up interval was around 49 months, 41 patients (37.3%) still reported numbness. We found that on average, people with numbness had a lower IKDC score and KOOS. Therefore, we concluded that it was worthwhile to take measures to avoid injury to the infrapatellar nerve during surgery and take into consideration the type of graft used, as this reflects directly on patients’ perception of knee function. We found no association between BMI and infrapatellar numbness, as demonstrated in Table 4.
In our study, the mean age at surgery was 27.92 years. Younger age at surgery has been reported to have a positive effect on patient-reported outcomes. 12 We did not find a significant relationship between age at surgery and patient-reported outcomes. We did, however, find that younger age at surgery significantly correlated with a lower likelihood of contralateral leg surgery in the future. In contrast, older age has been established in the literature to have lower odds of contralateral leg surgery.7,11,33 This difference was difficult to interpret since each study had a different definition for the older age group. For example, Cristiani et al 7 defined older age as ≥25 years, which is younger than that of our sample (27.92 years).
Tobacco smoking has been established in orthopaedic literature as a cause of impaired wound healing, delayed bone union, and loosening of implants after arthroplasty. 5 However, few studies have focused on the effect of smoking on the outcomes of arthroscopic procedures after ligamentous injuries of the knee.5,14,17 Our study showed that tobacco smoking is not associated with a change in patient-reported outcomes after primary ACLR.
Patients in our study had a mean period between ACL injury and ACLR of 18.4 months. We found no correlation between time from injury to surgery and patient-reported outcomes. This contrasts with a recent meta-analysis of 24 studies that concluded earlier surgical repair yields a better outcome compared with delayed surgery. 19 Delaying ACLR (>3 months) also leads to a greater risk of medial meniscal injury. 28 The issue remains that, to this day, no consensus exists regarding what cutoff point qualifies as “early” intervention. Some studies considered early intervention to be within 3 weeks of injury, while others considered ≤6 months to be an early intervention after injury. 19
The sample in the current study is mostly composed of young male patients. Patients with these characteristics (younger age, male sex) have previously been reported to have better patient-reported outcomes after ACLR. 12 Most patients in this study (92.7%) had a complete ACL tear which is a high percentage compared with percentages reported by Alsubaie et al. 1 This finding could be explained by the delayed time from injury to surgery, as partial tears can progress to complete tears. 10 Fayard et al 10 found that 39% of young active patients with partial ACL tears managed nonsurgically progressed to complete tears 43 months after the initial injury. Alsubaie et al 1 found that fatigue was more likely to be associated with a partial ACL tear compared with a complete tear. In our study, there was no significant difference between the partial and complete tear groups in the IKDC score or KOOS.
The menisci play an important role in knee stability and shock absorption. Concomitant injury of the menisci with ACL injury is common, with medial meniscal tears being more common than lateral meniscal tears. 23 In our study, the presence of a concomitant meniscal injury did not affect the patient-reported outcomes (neither IKDC nor KOOS). This result is in line with other similar studies on the relationship between meniscal injury and ACLR outcome scores.4,18 Not finding a significant effect of concomitant meniscal injury on IKDC/KOOS scores was unexpected, as a concomitant meniscal injury with ACL injury has been found to be associated with an increased prevalence of osteoarthritis at long-term follow-up. 20 Our study may have failed to detect the effect of meniscal injury on the outcome of ACLR, as this is a long-term outcome that requires a longer follow-up time to be assessed compared with our mean follow-up of 48.92 months.
The mean graft width used in our patients was 7.5 mm. We found no significant effect of graft width on clinical outcomes or postsurgical complications. A cohort study on 18,425 patients reported that the use of a graft diameter ≥9 mm had reduced the risk of early ACLR revision. 34 In our study, there was little variation in graft width used. Our surgeries mostly used a graft diameter of either 7 or 8 mm, with only 3 grafts >9 mm. Therefore, we could not validate the effect of various graft diameters on surgical outcomes.
As demonstrated in Figure 3, the time interval between injury and primary ACLR insignificantly affected the presence of concomitant meniscal injury. This finding contradicts what Lu et al have reported. 21 This could be due to the long mean time interval between injury and ACLR found in our study (mean ± SD, 18.37 ± 28.06 months) compared with what Lu et al 21 considered to be delayed ACLR, which was >50 days between injury and surgery.
Limitations
Our study is not without limitations. Our sample was limited to patients who underwent primary ACLR surgery at King Abdullah University Hospital. The study sample size in terms of female sex (n = 2) and partial ACL injury pattern (n = 8) was inadequate. According to Hamrin Senorski et al, 12 male patients have a better functional outcome after ACLR; however, we could not assess this relationship in our study due to the small female subcohort. Male patients represented 98% of our sample, which roughly reflects the proportion of patients by sex with ACL injuries in Jordan, mostly because female patients in our society are less likely to engage in high-impact sports. This is a retrospective follow-up study on the subjective outcomes after primary ACLR. We had no control over the management or level of activity of patients throughout the follow-up period. Clinical examination and imaging of patients were not feasible, which meant we could not objectively investigate clinical outcomes and long-term postoperative complications such as osteoarthritis, joint laxity, or stiffness.
Conclusion
Our study showed that a greater BMI and infrapatellar numbness negatively affected subjective outcomes after primary ACLR. An older age at the time of primary ACLR was associated with a greater likelihood of surgery in the contralateral leg.
Footnotes
Acknowledgements
The authors thank Esra’a Alhomaimat for her contribution to data collection.
Final revision submitted March 2, 2024; accepted April 4, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from King Abdullah University Hospital and Jordan University of Science and Technology (No. 97-2022).