
Abstract
Background:
Readiness for return to sports involves both physical and psychological aspects of recovery; however, the relationship between psychological and physical variables after anterior cruciate ligament (ACL) reconstruction (ACLR) is poorly understood.
Hypothesis:
ACLR patients with a higher psychological readiness would demonstrate better functional testing results at 6 months.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Participants were evaluated at 6 months after ACLR with various patient-reported outcome metrics: Hospital for Special Surgery Pediatric Functional Activity Brief Scale, pediatric or adult International Knee Documentation Committee Questionnaire (IKDC), Patient-Reported Outcomes Measurement Information System (PROMIS) - Psychological Stress Experience and ACL - Return to Sport After Injury (ACL-RSI) scale. Functional testing included quadriceps, hamstrings, and gluteal strength testing; Y-balance test; single-leg single hop, crossover hop, and triple hop tests; and timed 6-m hop test. Pearson correlation coefficient and multivariable regression were used to determine associations between the limb symmetry index (LSI) on functional testing and patient-reported outcomes. Those with LSI deficits <20% (better performance) were compared with those with deficits >20% (worse performance).
Results:
A total of 229 participants (89 male, 140 female) with a median age of 17 years (range, 10.3-30.6 years) were enrolled. IKDC had a moderate negative correlation with PROMIS - Psychological Stress Experience (r = -0.39; 95% CI = -0.49, -0.27; P < .001) and a moderate positive correlation with ACL-RSI (r = 0.55; 95% CI = 0.46, 0.64; P < .001). A total of 151 patients completed functional testing. ACL-RSI demonstrated a positive correlation with single-hop LSI (r = 0.21; 95% CI = 0.05, 0.35; P = .01) and timed 6-m hop (r = 0.28; 95% CI, 0.42; P = .001). When adjusting for sex, age, and graft type, patients who had <20% deficit on the single-hop test scored 16.6 points higher on ACL-RSI (P = .001), and those with <20% deficit on crossover hop testing scored a mean 13.9 points higher on ACL-RSI (P = .04)
Conclusion:
Higher psychological readiness for return to sport was associated with better performance and greater symmetry on hop testing 6 months after ACLR, suggesting a potential link between physical and psychological recovery.
Anterior cruciate ligament (ACL) tears are one of the most common adolescent and young adult knee injuries with increasing incidence in ACL reconstruction (ACLR) over time.6,14,30,37,42,49 Return to presurgery level of physical activity is typically feasible at 6 to 12 months after ACLR surgery; however, up to two-thirds of ACLR patients are not returning to preinjury activity levels even by 12 months postoperation.2,8,22 Complicating this goal is the risk of retear postoperation. In addition, it is reported that as many as 20% to 25% of young ACLR patients sustain secondary ACL injury, identified as either retear of the graft or ACL tear in the contralateral limb.4,47 Reinjury is more prevalent in younger athletes and those that return to higher-intensity sports, especially for the first 2 years after ACLR surgery.45,48 Determining when a young patient is ready to return to sport after ACLR therefore requires a patient-centered approach that recognizes both the physical readiness of the athlete and the risks associated with reinjury.
Methods to prevent reinjury and guide a young athlete to a successful return to sports include early weightbearing rehabilitation protocols, patient-reported outcome (PRO) scores, and functional testing.5,43 Functional testing provides an objective evaluation to assess a patient's physical response to rehabilitation and readiness to return to sport. A commonly used battery of testing includes single-leg hop, lower limb strength, and limb symmetry tests with emphasis placed not only on developing the appropriate strength ratios but also on balance and quality of movement.12,36
A new frontier is psychological readiness. Psychological readiness is reported in the literature as another important variable in a young athlete's return to sports.1,29,35 Fear of reinjury in particular can impede an athlete's ability to return to the preinjury level of fitness.9,22 Other studies suggest that motivation to return, a negative perception of the injury's influence on their lives, and a lack of goals can negatively affect return-to-sports outcomes.1,19,23
Despite growing scientific investigations and reports with regards to psychological readiness after ACLR surgery, more data are needed on the association between psychological readiness and physical function for young athletes recovering from ACLR surgery. Our primary aim was to assess the relationship between psychological readiness and physical function in young athletes undergoing functional testing at 6 months postoperatively. We hypothesized that, in pediatric and adolescent ACLR patients, higher psychological readiness would be associated with better functional testing results at 6 months.
Methods
Participants between the ages of 10 and 30 years who had undergone primary ACLR were enrolled prospectively at a single large academic pediatric sports medicine center between December 1, 2018, and March 31, 2020. The following criteria were set as inclusion criteria of the current study: participants who had (1) undergone primary ACLR surgery, (2) completed the PROs, and (3) performed functional testing at 6 months of follow-up (5- to 8-month acceptable range). Also, participants who underwent concomitant meniscal repair, partial meniscectomy, lateral extra-articular tenodesis, or anterolateral ligament reconstruction along with ACLR were also included. Exclusion criteria included revision ACLR, history of previous ipsilateral knee surgery, multiligamentous knee surgery, or incomplete PROs at follow-up. Graft type was chosen using shared decision-making by the surgeon and patient/family and according to surgeon preferences and included both hamstring (HS) tendon, bone-patellar tendon-bone (BPTB), quadriceps, and iliotibial band (ITB) autografts as well as anterior tibialis and Achilles tendon allografts. ACLR surgery was performed by 1 of 6 surgeons (M.D.M., D.E.K., M.A.C., Y-M.Y., M.S.K., L.J.M.) at the current study institution. Baseline demographic data including sex, age, primary sport, and time to return to sports was collected; concomitant meniscal pathology at the time of surgery was also noted. Patients and their families provided written assent/consent for participation in this study.
The postoperative rehabilitation protocol involved weightbearing immediately after the operation; those with concomitant meniscal repair surgeries had limited/partial weightbearing for 6 weeks postoperation. Regardless of concomitant meniscal repair, all patients at postoperation weeks 6 to 12 were to increase their strength and range of motion with the goal of returning to light running and plyometrics at 4 months. This postoperative physical therapy protocol was standardized across the 6 surgeons. Functional testing and patient outcome questionnaires, regardless of graft type or sport, were completed approximately 6 months postoperatively, consistent with previous literature in this realm.31,39
Patients completed a paper or electronic questionnaire via REDCap (Vanderbilt University) and performed functional testing at their 6-month follow-up visits. The questionnaire was a compilation of 4 previously validated PRO metrics: ACL - Return to Sport After Injury (ACL-RSI), the Patient-Reported Outcomes Measurement Information System (PROMIS) - Psychological Stress Experience (PROMIS-PSE), adult International Knee Documentation Committee (IKDC) for patients aged ≥18 years, pediatric IKDC (Pedi-IKDC) for patients aged <18 years, and the Hospital for Special Surgery Pediatric Functional Activity Scale (HSS Pedi-FABS). The ACL-RSI measures psychological readiness in return to sport via scores for emotion and confidence, with a higher score indicating a more positive psychological readiness, and was recently validated in pediatric and adolescent populations.10,44 The PROMIS-PSE assesses perception of disruption, controllability, manageability, anger, and fear, with higher scores indicating higher levels of stress and lower psychological readiness. 7 Previously shown to have no statistically significant differences, the IKDC (patients >18 years old) and the Pedi-IKDC (patients 10-18 years old) subjective scores were used to assess symptoms and functions in activities of daily living and were compared directly.18,20,33,38 The HSS Pedi-FABS quantifies the activity level of athletes. 16
Functional testing was performed by the department's injury prevention staff members (certified athletic trainers and strength and conditioning specialists) and consisted of 3 components: strength, balance, and hop tests. Four muscle groups - quadriceps (knee extensors), HS (knee flexors), gluteus maximus (hip extensors), and gluteus medius (hip abductors) - were tested using isometric measures as previously reported.27,41 The Y-balance test was used to assess balance and a composite score was calculated in accordance with previous documentation of this test.24,39 For single-leg hop tests, distance (in meters) was measured for single hop, crossover hop, and triple hop tests, while time (in seconds) was measured in the 6-m timed hop test. The testing procedure of the hop tests has been previously reported.3,32 The functional testing staff members were blinded to the results of the psychological testing (D.S.).
Statistical Analysis
Patient characteristics were summarized for the cohort. Mean, standard deviation, median, and interquartile range were used to summarize continuous variables, while frequency and percentage were used to summarize categorical variables. PROs were also summarized, including ACL-RSI scores, HSS Pedi-FABS scores, adult and Pedi-IKDC scores, and PROMIS-PSE scores. In functional testing, 152 patients participated in the hop testing; however, 1 person was excluded from the hop testing measurements because all their hop measurements were >3 standard deviations away from the mean. Correlations were determined between functional testing outcomes scores and PROs scores using Pearson correlation coefficient. Pearson correlation coefficient and multivariable regression were used to determine associations between the limb symmetry index (LSI) on functional testing and PROs. Those with LSI deficits <20% (better performance) were then compared with those with deficits >20% (worse performance). This cutoff was chosen by the senior authors (M.D.M., M.A.C.) based on literature demonstrating that the majority of skeletally immature patients do not achieve a 90% LSI (corresponding to an LSI deficit of 10% or less) at 6-month follow-up.17,26,40 A 95% CI was also estimated for significant correlations. P values of <.05 were considered significant.
Results
A total of 229 participants, median age of 17 years (range, 10.3-30.6 years) and 39% male (89/229), were enrolled in the study. Figure 1 details the eligible patient flow diagram. Complete cohort characteristics can be found in Table 1. A total of 58% of the cohort had HS tendon autografts (132/229), 20% had BPTB autografts (45/229), and 10% had ITB autografts (23/229), with the remaining 12% (29/229) receiving Achilles tendon allograft, anterior tibialis allograft, or quadriceps autografts. Soccer was the sport played most frequently (30%), followed by basketball (19%). A total of 20 patients (9%) from the overall cohort had a complication within the 6-month study period. The leading complication was arthrofibrosis in 9 patients (3.9%), with 4 of these patients (1.7%) undergoing surgical treatment. Other complications included superficial infection in 6 patients (2.6%), nerve injury in 2 patients (0.9%), allergic reaction in 1 patient (0.4%), contact dermatitis in 1 patient (0.4%), and painful hardware with subsequent removal of hardware in 1 patients (0.4%). The 2 patients with nerve injuries had a superficial peroneal nerve compression and postoperative saphenous nerve irritation, respectively; 6 patients required oral antibiotic treatment for a superficial infection, 1 patient received topical anti-irritation ointment, and 1 patient was treated conservatively for an allergic reaction resulting in swelling and redness around the wound dressing. Functional outcomes are outlined in Table 2. The median time between surgery and functional testing was 6 months (range, 5.1-8.0 months). PROs are listed in Table 3. The functional testing LSI measurements by graft type can be found in Table 4.
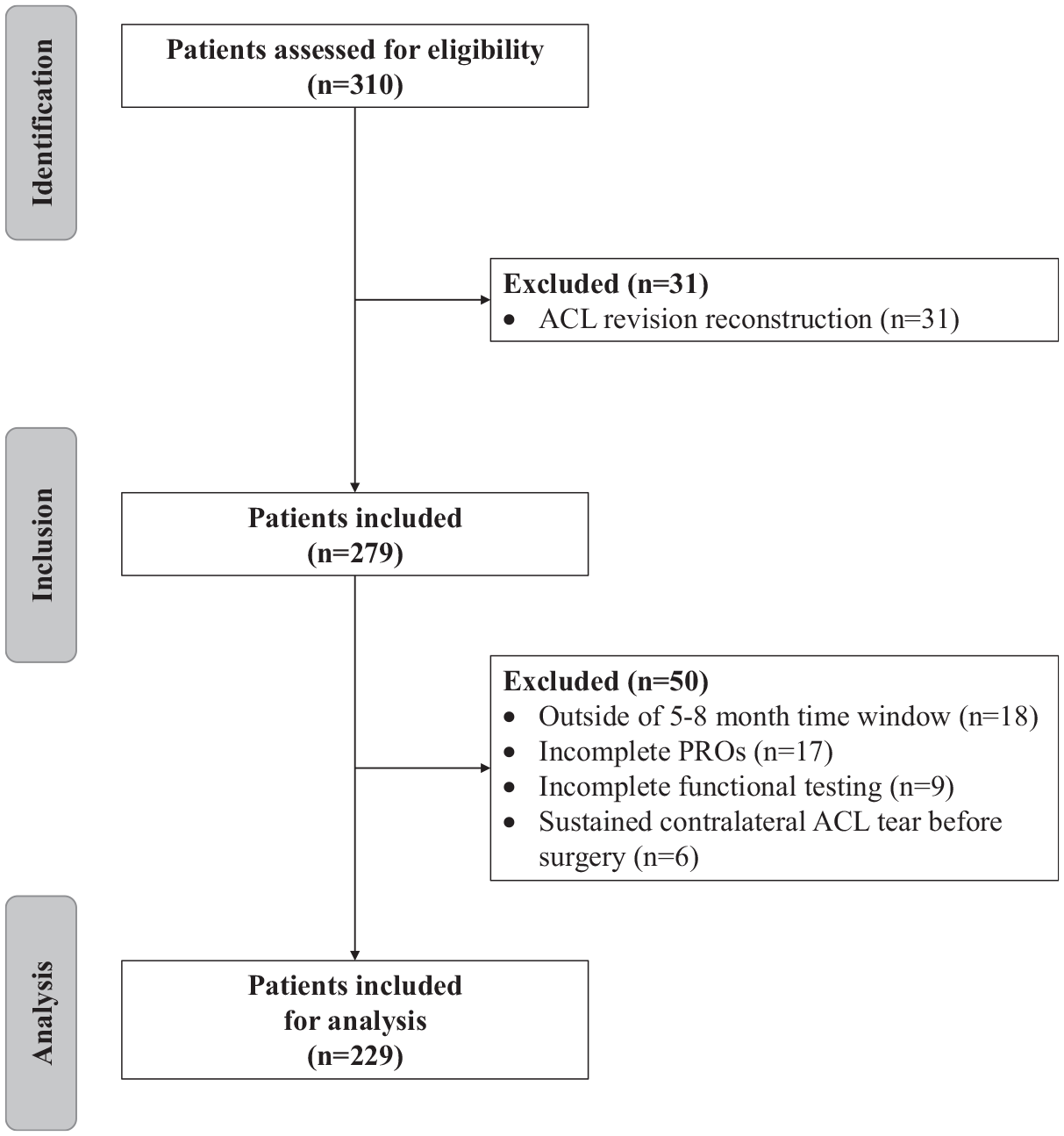
Consort diagram detailing how the final cohort of patients used in analysis was chosen. ACL, anterior cruciate ligament; PRO, patient-reported outcome.
Cohort Characteristics (N = 229) a

Data are presented as frequency (%) unless otherwise indicated. ACL, anterior cruciate ligament; BMI, body mass index; BPTB, bone-patellar tendon-bone; HS, hamstring; ITB, iliotibial band; IQR, interquartile range.
Number outsde of the parentheses represents the number of cases with available data for the given characteristic.
Functional Outcomes (N = 229) a

Data are presented as mean ± SD unless otherwise indicated. HS, hamstring; IQR, interquartile range; LSI, limb symmetry index.
Number in parentheses represents the number of cases with available data for the given characteristic.
Patient-Reported Outcomes (N = 229) a

ACL-RSI, Anterior Cruciate Ligament Reconstruction - Return to Sport after Injury; HSS Pedi-FABS, Hospital for Special Surgery Pediatric Functional Activity Brief Scale; IKDC, International Knee Documentation Committee; IQR, interquartile range; PRO, patient-reported outcome; PROMIS-PSE, Patient-Reported Outcomes Measurement Information System - Psychological Stress Experience.
Number in parentheses represents the number of cases with available data for the given characteristic.
IKDC refers to a composite of both adult and pediatric forms of the PRO.
Functional Testing LSI Measurements by Graft Type (N = 229) a

Data are presented as mean ± SD. LSI, limb symmetry index; BPTB, bone-patellar tendon-bone; HS, hamstring; ITB, iliotibial band. Dashes indicate no available data.
Number in parentheses represents the number of cases with available data for the given characteristic.
Only one patient recevied a quadriceps autograft, and they did not complete all of their 6-month testing. Therefore, they are missing values for some of the testing measures.
There was a weak positive correlation between the single-hop LSI and ACL-RSI scores (r = 0.21; 95% CI = 0.05, 0.35; P = .01). There was a weak positive correlation between the 6-m timed hop LSI and ACL-RSI scores (r = 0.28; 95% CI = 0.11, 0.42; P = .001) (Figure 2). There was a moderate negative correlation between IKDC scores and PROMIS-PSE scores (r = -0.39; 95% CI = -0.49, -0.27; P < .001). Conversely, there was a moderate positive association between IKDC scores and ACL-RSI scores (r = 0.55; 95% CI = 0.46, 0.64; P < .001) (Figure 3).
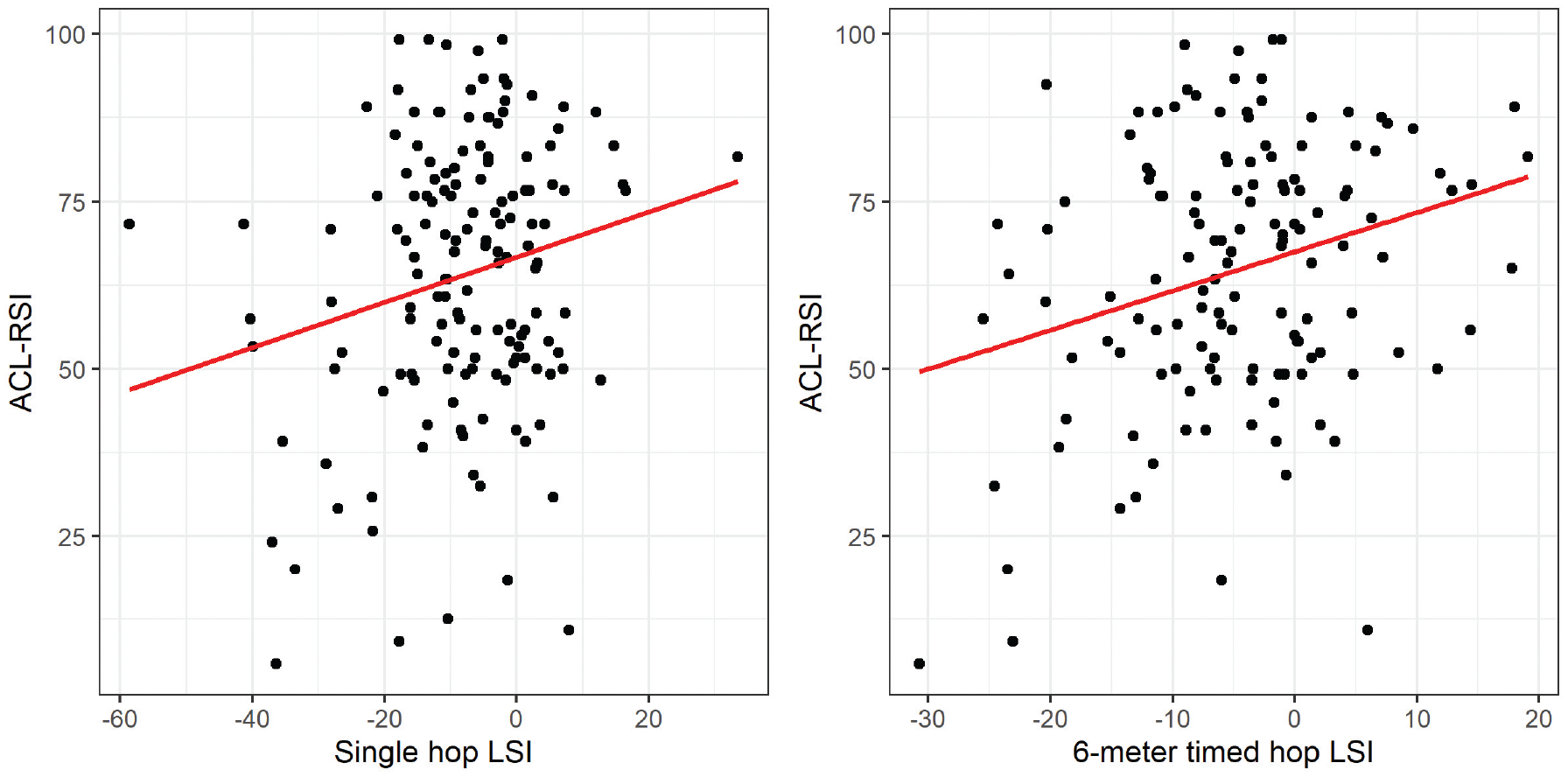
Correlation between hop testing measurements and ACL-RSI scores. There was a weak positive correlation between the single-hop LSI and ACL-RSI scores (r = 0.21; 95% CI = 0.05, 0.35; P = .01) and a weak positive correlation between the 6-m timed hop LSI and ACL-RSI scores (r = 0.28; 95% CI = 0.11, 0.42; P = .001). ACL-RSI, Anterior Cruciate Ligament - Return to Sport after Injury; LSI, limb symmetry index.

Correlation between PROs. There was a moderate negative correlation between IKDC scores and PROMIS-PSE scores (r = -0.39; 95% CI = -0.49, -0.27; P < .001) and a moderate positive association between IKDC scores and ACL-RSI scores (r = 0.55; 95% CI = 0.46, 0.64; P < .001). IKDC here refers to a composite of both adult and pediatric forms of the PRO. ACL-RSI, Anterior Cruciate Ligament - Return to Sport after Injury; IKDC, International Knee Documentation Committee; PRO, patient-reported outcome; PROMIS-PSE, Patient-Reported Outcomes Measurement Information System - Psychological Stress Experience.
Patients who performed better than a 20% deficit on their single-hop test scored on average 16.6 points higher on the ACL-RSI compared with patients with worse than a 20% deficit adjusting for sex, age at consent, and graft type (β = 16.56; 95% CI = 6.72, 26.41; P = .001). Patients who had better than a 20% deficit on their 6-m timed hop test scored on average 15.4 points higher on the ACL-RSI compared with patients who had worse than a 20% deficit (β = 15.39; 95% CI = 2.71, 28.07; P = .02), adjusting for sex, age at consent, and graft type. Patients who did better than a 20% deficit in their crossover hop test scored on average 13.9 points higher on their ACL-RSI questionnaire compared with patients who did worse than a 20% deficit (β = 13.93; 95% CI = 0.38, 27.48; P = .04), adjusting for sex, age at consent, and graft type.
Discussion
This prospective cohort study demonstrated that, at 6 months after ACLR, there was an association between higher psychological readiness (ACL-RSI) and better symmetry on hop testing. Of the 151 patients in our cohort who completed functional testing, there was a positive correlation between ACL-RSI scores and single-hop LSI (r = 0.21, P = .01) and 6-m timed hop LSI values (r = 0.28, P = .001) and a negative correlation between PROMIS-PSE and IKDC scores (r = -0.39, P < .001). Patients with <20% limb symmetry deficit on single hop, 6-m timed hop, and crossover hop testing scored 16.6 points (P = .001), 15.4 points (P = .02), and 13.9 points (P = .04) higher, respectively, on ACL-RSI.
Psychological readiness related to ACLR rehabilitation and return to sports has been reported in the literature; however, there has been little focus on the pediatric and adolescent population. In a recently published prospective cohort study of 176 patients with a mean age of 17.1 years, Milewski et al 31 found that psychological readiness and subjective perceptions of knee function after ACLR, via PROMIS-PSE and IKDC scores, were better in preadolescent (aged 10-14 years) patients and patients who had iliotibial grafts. Likewise, in their study of 93 adolescent athletes (aged ≤17 years), Kostyun et al 21 found that ACL-RSI scores were decreased before surgery and increased at all timepoints postoperatively. These 2 studies also identified that female patients had worse scores than male patients on ACL-RSI and PROMIS-PSE.21,31 Although both studies identified patient characteristics that may influence psychological readiness in young patients after ACLR, neither study correlated these findings with functional outcomes. Pascual-Leone et al 34 found that lower grit scores in pediatric patients were associated with reduced range of motion at 3 months after ACLR and meniscal repair, identifying a link between subjective psychological parameters and functional testing. Although they utilized a different scoring scale compared with our study, it seems that grit relates to a person's perseverance for long-term goals and has been associated with various psychological metrics.11,15 In a qualitative study by DiSanti et al, 13 psychosocial barriers to return to sport were more prevalent than physical barriers in their cohort of 10 adolescent patients, highlighting the importance of understanding the psychological aspect of recovery in younger patients.
In a mostly adult cohort with a mean age of 28 years, Webster et al 46 showed that greater limb symmetry on single-leg single hop for distance test, higher subjective knee scores (IKDC), younger age, shorter time to surgery, and male sex were associated with psychological readiness as measured with ACL-RSI. Our study mirrors these findings in a pediatric and adolescent population with the addition of more extensive functional testing such as strength, balance, and additional hop tests as well as PROMIS-PSE scoring. Similarly, Ardern et al 1 studied adults (mean age, 27.3 years) and found that psychological responses before surgery and during recovery were positively associated with a return to sport at 12 months. Our findings suggest that athletes with higher psychological readiness at 6 months showed better hop test symmetry, which may be more feasible to return to sports.
With the understanding that psychological readiness is associated with physical function after ACLR, the next layer of intervention is how to ensure young athletes are prepared psychologically for surgery and the extensive recovery process. Utilizing ACL-RSI and PROMIS-PSE in the preoperative and early postoperative period may help identify patients needing psychological intervention. It may be appropriate at times to refer patients to a sport psychologist for formalized psychological care on a case-by-case basis. The doctor-patient or physical therapist-patient relationship is also an area where realistic goal setting and encouragement can be provided to patients to reinforce their intrinsic motivation and self-esteem. There is ongoing innovative research in this field, notably on guided imagery. A randomized controlled trial that utilized imagery found improved knee laxity and lower anxiety levels in the experimental groups. 25 A narrative review by Matsuzaki et al 28 highlighted unique considerations of psychological recovery for young athletes, such as collaboration with parents and family, short-term goal setting with young athletes, and emphasizing 1-on-1 attention during provider visits.
The strengths of this study include the large sample size and inclusion of mostly pediatric and adolescent patients undergoing prospective analysis on how psychological readiness influences return to sport outcomes. As mentioned previously, many of the studies in this field have focused on adult populations, allowing our study to draw meaningful conclusions for the pediatric population. Another strength of this study is the inclusion of not only PRO instruments, which can be subjective in nature, but also objective physical performance testing.
There are several limitations to this study. The primary limitation is that we cannot determine causation or temporality between psychological readiness and functional scoring. It is possible that patients who are noticing functional improvements are having better psychological outcomes. Because of this, we are limited in our conclusions to say that there is only a correlation between psychological readiness and functional testing after ACLR. In addition, this study was completed at a single tertiary care pediatric hospital, which does not account for extensive geographic and patient population generalizability. Although the inclusion of a large variety of graft types and techniques as well as concomitant meniscal procedures provides a robust cohort for analysis, it also may be a confounding variable limiting our conclusions. Another limitation is that our follow-up period was limited to 6 months, and we cannot comment on longer-term outcomes. Although attempted, not all questionnaires were completed before functional testing given the nature of busy clinical office visits, which means a patient's mental state could have been affected by their performance on the follow-up testing. Likewise, we do not have preoperative psychological assessments with which to compare our findings, which could offer an important area of subsequent research in this field.
Conclusion
This study demonstrated psychological readiness is associated with objective postoperative physical function, measured with single-leg hop testing in pediatric and adolescent patients at 6 months after ACLR. ACL-RSI and PROMIS-PSE scores can assist in evaluating pediatric, adolescent, and young adult psychological readiness and should be considered for routine use alongside functional metrics. Further studies should identify which patients are more vulnerable to adverse effects of poor psychological readiness and aim to develop interventions for psychological readiness in addition to standardized physical rehabilitation protocols.
Footnotes
Final revision submitted January 31, 2024; accepted March 4, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.D.M. has received royalties from Elsevier and serves on the board of directors for PRiSM. M.A.C. has received royalties from Springer Inc and serves on the board of directors for PRiSM. Y-M.Y. is a consultant for Smith+Nephew and serves on the editorial board for the American Journal of Sports Medicine. E.J.S. has received education payments from Smith+Nephew and hospitality payments from Stryker and Zimmer Biomet Holdings. M.S.K. has received royalties from OrthoPediatrics and education payments from Kairos Surgical. D.E.K. has received education payments from Kairos Surgical and consulting fees from DePuy Synthes Products. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
IRB Approval was given by the Boston Children’s Hospital IRB for this study.