
Abstract
Background:
Psychological readiness to return to sports (RTS) has been associated with second anterior cruciate ligament (ACL) injury. However, this relationship is controversial because covariates such as anatomic and knee function characteristics have not been adequately considered.
Purpose/Hypothesis:
To investigate whether psychological readiness in the early postoperative period can predict the occurrence of a second ACL injury within 24 months after primary ACL reconstruction (ACLR) using propensity score analysis. It was hypothesized that patients with high ACL–RSI after injury (ACL-RSI) scores at 3 months postoperatively would have a second ACL injury within the projected postoperative period.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 169 patients who underwent primary ACLR using hamstring tendon autografts between November 2017 and July 2021 and also underwent knee functional assessments at 3 months postoperatively. The ACL-RSI scale was used to assess psychological readiness for RTS. A second ACL injury was defined if ipsilateral or contralateral ACL injury was confirmed by examination within 24 months postoperatively. Based on a previous study showing that 65 was the highest cutoff value for the ACL-RSI score for RTS, we classified patients into 2 groups: those with high ACL-RSI scores (≥65; group H) and those with low ACL-RSI scores (<65; group L). We generated 1-to-1 matched pairs using propensity score analysis and used log-rank testing to compare the rate of second ACL injury between the 2 groups.
Results:
More patients returned to any sports activities within 12 months in group H than in group L (90% vs 73%; P = .03). A second ACL injury within 24 months postoperatively was identified in 7% of patients (13/169). The rate of second ACL injury was significantly higher in group H than in group L (17.6% vs 3.4%; P = .001). In 43 matched pairs extracted using propensity scoring, the rate of second ACL injury was also higher in group H than in group L (18.6% vs 4.7%; P = .04).
Conclusion:
Patients with a higher ACL-RSI score at 3 months exhibited a significantly higher incidence of second ACL injury within 24 months after primary ACLR.
Keywords
Although most patients regain knee stability and return to preinjury sports activity after an anterior cruciate ligament (ACL) injury, approximately 5% to 10% of patients sustain a second ACL injury (ACL graft failure or a contralateral ACL injury) within 2 years after primary ACL reconstruction (ACLR).13,29,30,36 Because patients with a second ACL injury have lower subjective outcomes and an increased risk of future knee osteoarthritis than those without a second ACL injury, 12 it is important to identify the risk factors for a second ACL injury.
Some studies have reported potential risk factors for second ACL injury—such as younger age,17,35 early return to high-activity sports,6,13,14 greater posterior tibial slope (PTS),25,32 and asymmetry of knee kinematics and strength.14,26 In addition, recent studies have suggested that psychological readiness to return to sports (RTS) is associated with a second ACL injury. Piussi et al 27 reported that patients who sustained ACL rerupture within 2 years after primary ACLR had higher ACL–RTS after injury (ACL-RSI) scores at 8 and 12 months after surgery than those who did not suffer ACL rerupture. Previous studies have reported that a higher ACL-RSI score in the early postoperative period could predict RTS while also predicting a second ACL injury.2,18,28 Conversely, it has been reported from other studies that a low ACL-RSI score was associated with a second ACL injury.21,22 Therefore, the relationship between ACL-RSI and a second ACL injury remains controversial. In addition, these studies did not adequately consider covariates such as anatomic characteristics, knee function, or RTS because of the limited sample size. Hence, the relationship between psychological readiness and second ACL injury remains unclear. Statistical methods based on the propensity score (PS) have recently been used to adjust covariates in clinical research. PS analysis can include more variables and adjust confounding factors more effectively than traditional multivariate analyses that directly incorporate many variables. 15
This study aimed to investigate whether the ACL-RSI score in the early postoperative period (at 3 months postoperatively) is associated with a second ACL injury within 24 months after primary ACLR with hamstring tendon autografts. PS analysis was used to adjust covariates such as patient characteristics and postoperative knee function. The study hypothesized that patients with high ACL-RSI scores in the early postoperative period would have a higher likelihood of a second ACL injury within 24 months of ACLR.
Methods
Study Patients
This ongoing, single-center, prospective cohort study included patients with or without meniscal and cartilage injury who underwent primary ACLR with hamstring tendon autografts between November 2017 and July 2021. All patients regularly participated in some sports activity before an ACL rupture and underwent knee functional tests approximately 3 months after primary ACLR. Patients were excluded according to the following criteria: (1) bilateral ACLR; (2) multiligament reconstruction; (3) history of ACLR on the ipsilateral or contralateral side; (4) ACLR using a bone–patellar tendon–bone graft; (5) history of lower limb surgery; (6) other surgery during or after primary ACLR, except for meniscus surgery (meniscectomy or meniscal repair); (7) no participation in any sports activity regularly before ACL rupture; (8) incomplete patient characteristics and surgical data; or (9) failure to follow-up after postoperative knee functional testing at 3 months. This study was performed according to the Declaration of Helsinki. The study protocol was approved by our ethics committee, and all included patients provided informed consent.
All patients were referred from other hospitals, and surgery was decided on after confirming recovery of the range of motion of the knee. Double-bundle ACLR was performed primarily, with single-bundle ACLR performed on patients with open epiphysis or those with partial ACL tears. All patients underwent the same postoperative time-based rehabilitation protocol until 6 months postoperatively. Inpatient rehabilitation began 3 days after surgery, and outpatient rehabilitation was conducted at rehabilitation centers in our hospitals or local hospitals. Postoperative regular follow-up was scheduled at least at 3, 6, 12 months, and 2 years after surgery.
Patient Characteristics
The following descriptive and surgical data were recorded from patient interviews and medical records: age at the time of surgery; sex; body mass index; preinjury Tegner activity level; time from injury to primary ACLR; reconstruction technique (single- or double-bundle 19 ); medial or lateral meniscal injury that needed surgical treatment (meniscectomy and/or meniscal repair); cartilage injury; and PTS. The PTS was evaluated using the proximal anatomic axis PTS measurement technique on lateral knee radiographs. Lateral knee radiographs were taken with the patients standing in a neutral position, and the x-ray beam was focused directly on the midsagittal plane of the knee. Midpoints 5 and 15 cm distal to the joint line on the anterior and posterior tibial cortices were identified. These midpoints were connected by a vertical line to establish the longitudinal axis for the PTS calculation.7,11
Knee Functional Assessments
All patients were evaluated for knee function approximately 3 months after ACLR. Measures recorded included the isokinetic quadriceps and hamstring strength, patients’ subjective evaluation, and anterior tibial translation. These variables were also evaluated routinely at approximately 6, 12, and 24 months after ACLR for patients who visited the clinic for examination at those times.
Isokinetic quadriceps and hamstring strength were measured at 60 deg/s using an isokinetic dynamometer (Genu PLUS; Inter Reha). Each patient performed 2 practice contractions followed by 5 maximal effort contractions, and the peak extension and flexion torque were measured. The limb symmetry indexes for quadriceps strength (LSI-Q) and hamstring strength (LSI-H) were calculated by normalizing the involved limb peak torque with the uninvolved limb and multiplying the result by 100%.
The International Knee Documentation Committee (IKDC) subjective form was used to assess patients’ subjective knee function. This joint-specific outcome measure consists of 18 items. Scores range from 0 to 100, with higher scores indicating better subjective knee function. The IKDC subjective form has been shown to be a valid, reliable, and responsive measure of outcomes after ACLR.1,24
The anterior tibial translation was assessed using a KT-2000 arthrometer (MEDmetric) with maximum manual force. The side-to-side difference in anteroposterior tibial displacement between the involved and uninvolved knees was recorded.
Psychological Readiness to RTS
The Japanese version of the ACL-RSI scale was used to assess psychological readiness for RTS. This scale consists of 12 items and includes 3 domains—emotions, confidence, and risk appraisal. Each score is summed and averaged between 0 and 100, with higher scores indicating greater psychological readiness. This scale has been previously validated for patients after ACLR.16,33 ACL-RSI and knee function were assessed simultaneously .
Return to Sports
To determine whether patients would RTS activities, we administered a questionnaire to inquire whether patients would return to playing sports within 12 and 24 months after surgery. 31 RTS was defined as participating in a match or practice game for any sports activities. We recorded the number of patients who sustained a second ACL injury during sports activity within 12 and 24 months after primary ACLR.
Second ACL Injury
The primary endpoint of this study was the number of days from surgery to the second ACL injury. The second ACL injury was defined if the ipsilateral or contralateral knee was injured in a second incident, and ACL injury was confirmed by the surgeon’s examination within 24 months after surgery. We asked patients the date of their second ACL injury and calculated the time from primary ACLR to the date of the second ACL injury. Patients without a second ACL injury underwent a follow-up evaluation until 24 months postoperatively to complete the study.
Statistical Analysis
The study patients were classified into 2 groups according to the ACL-RSI score: the group with high ACL-RSI scores (group H) and the group with low ACL-RSI scores (group L). An ACL-RSI score of 65 at 3 months after primary ACLR was used as the cutoff point for grouping the patients. This value is the highest reported cutoff point for RTS. 28 Univariate analyses included the unpaired t test, Mann-Whitney U test, chi-square test, and Fisher exact test to compare characteristics, knee function variables, and psychological readiness 3 months after primary ACLR between the 2 groups. The RTS rates 12 and 24 months after surgery were also compared between the 2 groups.
PS Matching Analysis
To adjust for confounding factors, we conducted PS matching to compare the rate of second ACL injury between the study groups. First, we calculated the PS using a logistic regression model. The dependent variable was the ACL-RSI score at 3 months after primary ACLR. Independent variables were the following patient characteristics and 3-month postoperative knee function variables: age at the time of surgery; sex; body mass index; preinjury Tegner score; time from injury to surgery; surgical technique; medial or lateral meniscal injury; cartilage injury; PTS; LSI-Q; LSI-H; IKDC subjective score; and anterior tibial translation. Next, PS matching analysis was performed by nearest-neighbor matching with a caliper width of 0.2 for 1 to 1 matching. 4 For the matched patients, univariate analyses and the calculation of the standardized difference were performed to compare the 2 groups to check the covariate balance. A standardized difference of ≥0.1 represented an acceptable balance. 5
Kaplan-Meier Survival Analysis With/Without PS Matching
Kaplan-Meier survival statistics and the log-rank test were used to evaluate the second ACL injury and differences in event-free survival rates according to ACL-RSI at 3 months (group H vs group L) after primary ACLR in all patient cohorts and matching cohorts.
Cox Regression Analysis
Since PS matching excludes unmatched patients, a Cox proportional hazard regression analysis with crude and PS-adjusted covariates, including all the patients, was performed to address selection bias. 3 Cox proportional hazard regression analysis data are presented as hazard ratios with 95% CIs. The minimum sample size for Cox proportional hazard regression analysis was 165 patients, assuming a reinjury rate of 3% for group H and 15% for group L, with an alpha level of .05 and a beta of 80%.
All statistical analyses were conducted using R version 4.1.1 (The R Foundation for Statistical Computing). The threshold for statistical significance was set at P < .05 for all comparisons.
Results
Of the 399 patients, 169 patients were included in this study. A flowchart of the patient inclusion process is shown in Figure 1. The median follow-up period was 730 days (range, 186-730 days). Among the 169 included patients, 125 patients (74%) had 24 months of follow-up data. A second ACL injury within 24 months after primary ACLR occurred in 7.7% (13/169) of patients at a median of 361 days (range, 191-722 days). ACL graft failure occurred in 9 patients at a median of 262 days (range, 191-582 days). Contralateral ACL injury occurred in 4 patients at a median time of 542 days (range, 270-722 days). Of the 13 patients who sustained a second ACL injury, 10 patients were injured during participation in their preinjury sport, 1 patient was injured during participation in a sport different from the preinjury sport, 1 patient was injured due to a fall, and 1 was injured due to an unknown reason.

Flowchart of patient inclusion. ACL, anterior cruciate ligament.
Comparison of Patients With Versus Without Second ACL Injury
Patients who sustained a second ACL injury within 24 months after primary ACLR (n = 13) were significantly younger, had a higher preinjury Tegner score, a higher LSI-Q score, and a higher ACL-RSI score at 3 months postoperatively compared with patients who did not sustain a second ACL injury (n = 156). No significant differences were found in the RTS rate within 12 and 24 months between the 2 groups (Table 1). The comparison results between the 13 patients who sustained a second ACL injury within 24 months postoperatively and uninjured patients who completed 24 months of follow-up (n = 112) are shown in Appendix Table A1. The area under the receiver operating characteristic curve was 0.68, and the cutoff value obtained from the present study was 65 points (Appendix Figure A1).
Comparison of Characteristics and Knee Function Between Patients With and Without Second ACL Injury a

Values are presented as mean ± SD or n (%). Bold P values indicate statistically significant differences between groups (P < .05). ACLR, anterior cruciate ligament reconstruction; ACL-RSI, ACL-return to sport after injury; BMI, body mass index; IKDC, International Knee Documentation Committee; LSI-H, limb symmetry index for hamstring strength; LSI-Q, limb symmetry index for quadriceps strength.
The side-to-side difference at manual maximum force was measured using a KT-2000 arthrometer. Positive values mean anterior translation. Greater value means more anterior translation in the operative side relative than that in the nonoperated side.
Data from 11 patients in the no second ACL injury group were not available.
Data from 19 patients in the no second ACL injury group were not available.
Comparison of Patients With High Versus Low ACL-RSI Scores
Of the 169 patients, 51 patients (30.2%) had an ACL-RSI score of ≥65 and were included in group H, and 118 patients (69.8%) had an ACL-RSI score of <65 and were included in group L. The mean patient age in group H was significantly lower. Regarding knee function 3 months after primary ACLR, the LSI-Q and IKDC subjective scores were significantly higher in group H than in group L (Table 2).
Comparison of Characteristics and Knee Function Between Group H and Group L a
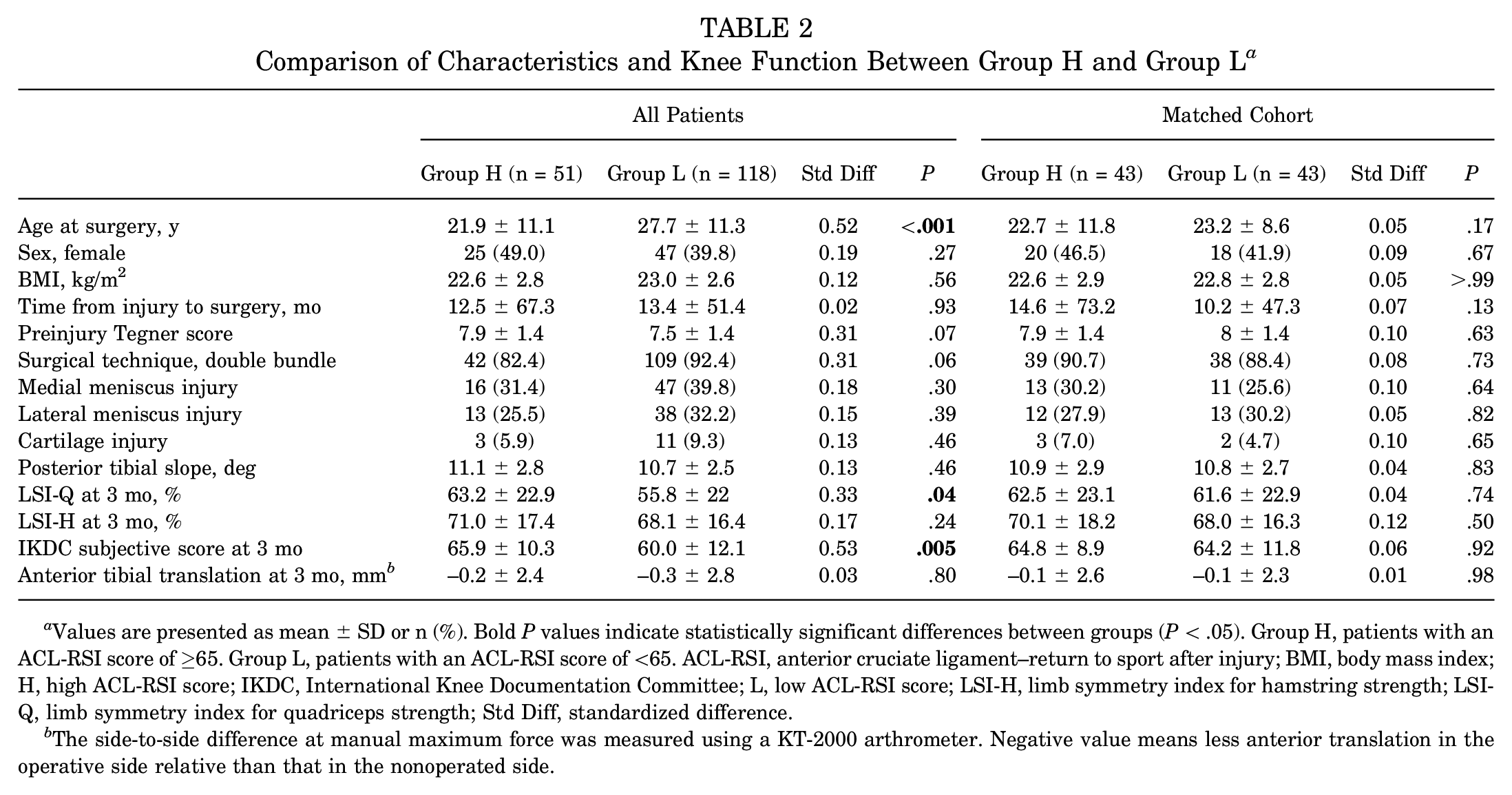
Values are presented as mean ± SD or n (%). Bold P values indicate statistically significant differences between groups (P < .05). Group H, patients with an ACL-RSI score of ≥65. Group L, patients with an ACL-RSI score of <65. ACL-RSI, anterior cruciate ligament–return to sport after injury; BMI, body mass index; H, high ACL-RSI score; IKDC, International Knee Documentation Committee; L, low ACL-RSI score; LSI-H, limb symmetry index for hamstring strength; LSI-Q, limb symmetry index for quadriceps strength; Std Diff, standardized difference.
The side-to-side difference at manual maximum force was measured using a KT-2000 arthrometer. Negative value means less anterior translation in the operative side relative than that in the nonoperated side.
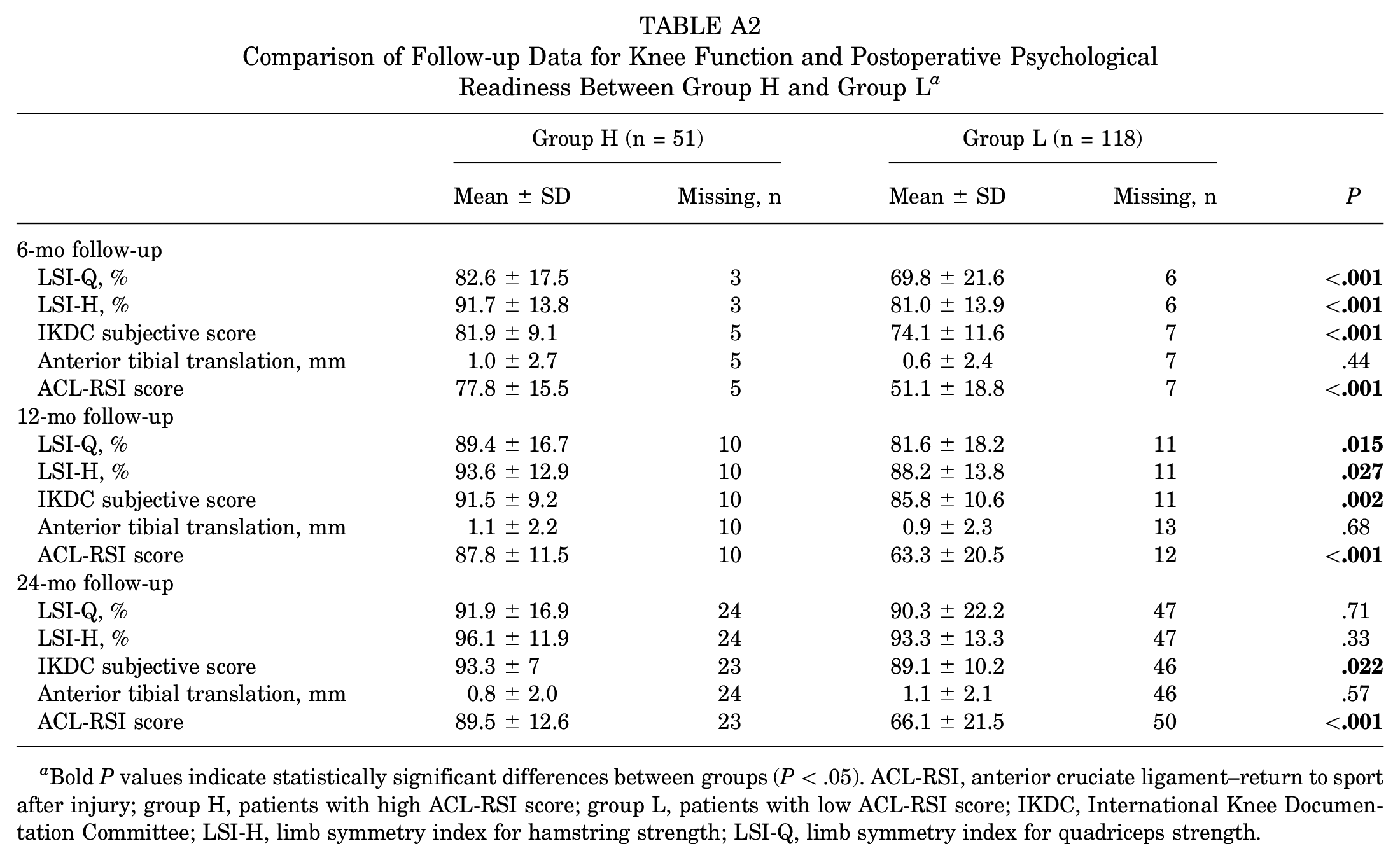
The rates of return to any sports activities were 78.5% (124/158 patients) within 12 months and 90.7% (136/150) within 24 months after surgery. The patients in group H had a significantly higher rate of return to any sports within 12 months postoperatively (90% vs 73% for group L; P = .03) (Figure 2). The LSI-Q, LSI-H, IKDC subjective score, anterior tibial translation, and ACL-RSI scores at 6, 12, and 24 months in both study groups are shown in Appendix Table A2. LSI-Q, LS-H, and IKDC subjective scores at 6 and 12 months were significantly higher in group H than in group L.
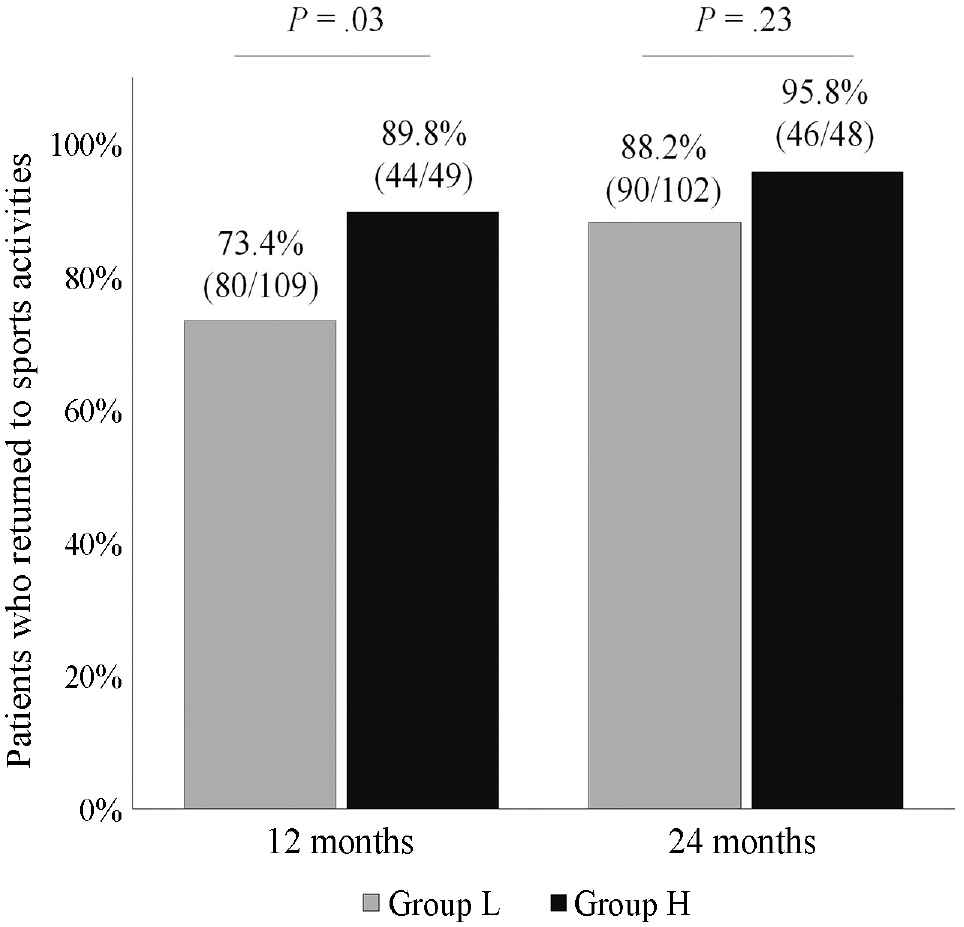
The percentage of patients who returned to sports activities within 12 and 24 months postoperatively. Group H included patients with high ACL-RSI scores; group L included patients with low ACL-RSI scores. ACL-RSI, anterior cruciate ligament–return to sport after injury .
PS Matching Analysis
Regarding PS matching, 43 pairs were generated (43/51 patients in group H, 43/118 patients in group L). The C-statistic value was 0.73. After PS matching, the standardized difference for characteristics and knee function measures was ≤0.10 for all but 1 variable between the matched groups (Table 2).
Kaplan-Meier Survival Analysis With or Without PS Matching
In all the patients, the Kaplan-Meier survival statistics and the log-rank test showed that patients in group H had a significantly higher incidence of second ACL injury within 24 months after surgery than patients in group L (17.6% [9/51 patients] vs 3.4% [4/118 patients], respectively). In the matched pairs, the Kaplan-Meier survival statistics and the log-rank test also showed that group H exhibited a significantly higher incidence of second ACL injury within 24 months after surgery than group L after PS matching (18.6% [8/43 patients] vs 4.7% [2/43 patients], respectively) (Figure 3).

The Kaplan-Meier survival curve for the incidence of second ACL injury within 24 months after primary ACLR in patients (A) without propensity score matching and (B) with propensity score matching. ACLR, anterior cruciate ligament reconstruction; ACL-RSI, anterior cruciate ligament–return to sport after injury.
Cox Proportional Hazard Regression Analyses
The Cox proportional hazard regression analyses with crude and adjusted PS indicated that a higher ACL-RSI score at 3 months after primary ACLR was significantly associated with the occurrence of a second ACL injury within 24 months (Table 3).
Results of the Cox Proportional Hazard Regression Analyses a

ACL-RSI, anterior cruciate ligament–return to sport after injury; group H, patients with high ACL-RSI scores; group L, patients with low ACL-RSI scores; HR, hazard ratio.
After adjusting for propensity score as a covariate.
Discussion
In the present study, patients with a higher ACL-RSI score at 3 months after primary ACLR with hamstring tendon autografts had a significantly higher rate of second ACL injury within 24 months after surgery. These findings indicated that patients with a greater psychological readiness to RTS in the early postoperative period after ACL surgery are an independent predictor of a second ACL injury.
Several recent studies have focused on the association of the ACL-RSI score with a second ACL injury. In a retrospective study, Piussi et al 27 reported that patients who experienced ACL graft failure within 2 years after primary ACLR had higher ACL-RSI scores at 8 and 12 months after surgery than those who did not experience failure. 27 The authors of that study suggested that greater psychological readiness for RTS might increase the risk of ACL graft failure. Conversely, McPherson et al 21 reported that younger (≤20 years) patients with a second ACL injury had a significantly lower ACL-RSI score at 12 months than younger patients without a second ACL injury. The same authors also reported that young patients who sustained a second ACL injury at a mean of 2 years had a significantly smaller change in the ACL-RSI score from preoperative to 12 months than patients who did not sustain a second ACL injury. 22 These results suggest that a low ACL-RSI score could be associated with a second ACL injury, contradicting the results of our study. The reason for the opposite associations between their study and our study may be attributed to differences in the patient population and timing of the second ACL injury since their studies included only young patients who could RTS after ACLR, the observed relationship could be different with the inclusion of older patients. Therefore, further studies are needed to examine differences by subject characteristics, especially with age groups or RTS.
In the present study, PS analyses revealed that the ACL-RSI score at 3 months postoperatively was independently associated with a second ACL injury, even after adjusting for age, PTS, and knee function covariates. Since an increasing number of studies have revealed that the ACL-RSI score is associated with RTS activity after ACLR, the ACL-RSI score can be an important criterion for RTS activity.2,18,23,28 However, early postoperative RTS is generally considered a risk for second ACL injury.6,14 In the present study, patients in group H exhibited a higher percentage who returned to sports within 1 year (89.8% vs 73.4%; P = .03) and better muscle recovery (LSI-Q, 89.4 ± 16.7 vs 81.6 ± 18.2 ; P = .015) compared with group L patients. It is possible that patients who had high psychological readiness in the early postoperative period increased activity or returned to sports in the early postoperative period, resulting in a second ACL injury. Some studies have reported that better knee functions8,20 and returning to a high activity level sports after primary ACLR34,35 were associated with a second ACL injury. Therefore, the results of this study suggest that patients with greater psychological readiness for RTS in the early postoperative period should be given adequate information about the risk of a second ACL injury and the ideal timing of RTS after ACLR.
Limitations
This study has some limitations. The sample size was limited, as this study was conducted at a single institution. Patients who underwent ACLR using bone–patellar tendon–bone grafts and did not participate in any sports activity were excluded. Therefore, the results should be generalized with caution. In addition, 44 patients did not have complete 24-month follow-up data in this study, so this study may have selection bias. In addition, we used PS analyses to adjust the covariates. However, potential risk factors—such as the history of family ACL injury9,10 and size of graft 17 —were not adjusted for. Furthermore, the timing of RTS activity 14 has not been investigated and should be considered in future studies. We used a cutoff score of 65 on the ACL-RSI scale to divide the study groups, but other cutoff values may provide different results. Finally, although the same rehabilitation protocol was applied to all the patients in this study, the details of the program, including frequency and intensity, were not assessed. Despite all the limitations, the results of the present study represent information that may be beneficial in preventing secondary ACL injuries.
Conclusion
Patients with a higher ACL-RSI score at 3 months postoperatively exhibited a significantly higher incidence of second ACL injury within 24 months after primary ACLR with hamstring tendon autograft. The results of this study indicated that patients with high psychological readiness for RTS in the early postoperative period are at a higher risk of second ACL injury than other patients and should be closely monitored.
Footnotes
Appendix
Comparison of Follow-up Data for Knee Function and Postoperative Psychological Readiness Between Group H and Group L a
| Group H (n = 51) | Group L (n = 118) | P | |||
|---|---|---|---|---|---|
| Mean ± SD | Missing, n | Mean ± SD | Missing, n | ||
| 6-mo follow-up | |||||
| LSI-Q, % | 82.6 ± 17.5 | 3 | 69.8 ± 21.6 | 6 |
|
| LSI-H, % | 91.7 ± 13.8 | 3 | 81.0 ± 13.9 | 6 |
|
| IKDC subjective score | 81.9 ± 9.1 | 5 | 74.1 ± 11.6 | 7 |
|
| Anterior tibial translation, mm | 1.0 ± 2.7 | 5 | 0.6 ± 2.4 | 7 | .44 |
| ACL-RSI score | 77.8 ± 15.5 | 5 | 51.1 ± 18.8 | 7 |
|
| 12-mo follow-up | |||||
| LSI-Q, % | 89.4 ± 16.7 | 10 | 81.6 ± 18.2 | 11 |
|
| LSI-H, % | 93.6 ± 12.9 | 10 | 88.2 ± 13.8 | 11 |
|
| IKDC subjective score | 91.5 ± 9.2 | 10 | 85.8 ± 10.6 | 11 |
|
| Anterior tibial translation, mm | 1.1 ± 2.2 | 10 | 0.9 ± 2.3 | 13 | .68 |
| ACL-RSI score | 87.8 ± 11.5 | 10 | 63.3 ± 20.5 | 12 |
|
| 24-mo follow-up | |||||
| LSI-Q, % | 91.9 ± 16.9 | 24 | 90.3 ± 22.2 | 47 | .71 |
| LSI-H, % | 96.1 ± 11.9 | 24 | 93.3 ± 13.3 | 47 | .33 |
| IKDC subjective score | 93.3 ± 7 | 23 | 89.1 ± 10.2 | 46 |
|
| Anterior tibial translation, mm | 0.8 ± 2.0 | 24 | 1.1 ± 2.1 | 46 | .57 |
| ACL-RSI score | 89.5 ± 12.6 | 23 | 66.1 ± 21.5 | 50 |
|
Bold P values indicate statistically significant differences between groups (P < .05). ACL-RSI, anterior cruciate ligament–return to sport after injury; group H, patients with high ACL-RSI score; group L, patients with low ACL-RSI score; IKDC, International Knee Documentation Committee; LSI-H, limb symmetry index for hamstring strength; LSI-Q, limb symmetry index for quadriceps strength.
Acknowledgements
The authors thank the staff of Kobe University Hospital for its support during this study.
Final revision submitted December 3, 2023; accepted January 10, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the Japan Society for the Promotion of Science grant-in-aid for scientific research (KAKENHI; grant No. JP 21K11336). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kobe University Graduate School of Medicine (reference No. B190055).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.