
Abstract
Background:
The relationship between postoperative alignment and clinical outcomes after double-level osteotomy (DLO) has not been clarified.
Purpose:
To examine the radiological and clinical outcomes after DLO and specifically evaluate the influence of the joint-line convergence angle (JLCA) on the accuracy of alignment correction and surgical outcomes.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Included were 74 knees in 51 patients (mean age, 61.0 years) who underwent DLO for varus osteoarthritic knees and who had a minimum of 2 years of follow-up. The target hip-knee-ankle angle (HKAA) for the intended limb alignment was set to 1° valgus. The lateral distal femoral angle, medial proximal tibial angle, JLCA, and HKAA were measured on preoperative and postoperative radiographs. Outliers in alignment correction were defined as a deviation of ≥3° from the originally intended HKAA. Clinical outcomes were assessed using the Knee injury and Osteoarthritis Outcome Score (KOOS). In the data analysis, the influence of the radiological parameters on the postoperative outcomes was statistically assessed.
Results:
Radiological and clinical evaluation at 2-year follow-up showed significant improvement from preoperative values (P < .001). The HKAA was corrected from 13.4°± 3.0° varus preoperatively to 0.5°± 2.8° varus at 2 years, indicating a slight undercorrection. Regarding clinical outcomes, significant pre- to postoperative improvement was found on the KOOS (from 185.0 ± 71.2 to 387.9 ± 70.5; P < .001). Overall, 22 of the 74 knees (29.7%) were deemed to be outliers at the 2-year follow-up (19 knees [25.7%] in undercorrection, 3 knees [4.1%] in overcorrection). Postoperative KOOS values were significantly worse in the outliers than in the nonoutliers (344.4 ± 77.7 vs 405.8 ± 59.3; P < .001), and both pre- and postoperative JLCA was significantly larger in the outlier group. The receiver operating characteristic curve analysis indicated a preoperative cutoff JLCA of 6.0° for predicting postoperative alignment outliers.
Conclusion:
A preoperative JLCA of ≥6° was found to be a significant prognostic factor affecting the radiological and clinical outcomes after DLO for varus osteoarthritic knees by compromising the accuracy of deformity correction, resulting in suboptimal postoperative alignment.
Osteotomy around the knee is a well-established and widely performed treatment for knee osteoarthritis (OA). Traditionally, high tibial osteotomy (HTO) has been the most popular procedure performed for varus unicompartmental knee OA, and satisfactory results have been reported in the literature.10,12,33 However, studies have shown that in cases of severe varus deformity, correcting the deformity with HTO alone can result in nonphysiological joint-line obliquity (JLO) and require a large amount of correction.1,28,36 In addition, the use of nonphysiological JLO may lead to inferior clinical outcomes.16,37,41 A recent surgical simulation study found that correcting varus deformity with HTO alone restores physiological bone and joint shape in only 28% of patients, with a third of patients requiring double-level osteotomy (DLO). 9 Therefore, in recent years, improvements in surgical technique have expanded the indications for DLO, especially in active patients with severe varus knee OA, and satisfactory clinical outcomes have been reported.8,9,13,15,25,26
The surgical concept of osteotomy around the knee is to restore optimal bone and joint geometry to create a favorable biomechanical environment at the knee. Therefore, it is critical to correct the deformity accurately according to the surgical plan. However, even if the surgery is performed as planned in the preoperative surgical simulation, there are cases of postoperative malalignment with over- or undercorrection. There are some factors such as large joint-line convergence angle (JLCA), osteotomy height, hinge height, and body mass index reported as causes of malcorrection after HTO.3,22 Among those, previous relevant studies have shown that JLCA associated with excessive soft tissue laxity in the knee joint is a predominant factor to affect the prediction of alignment correction leading to malcorrection in HTO.3,23 Varus deformity of the knee is composed of bony and articular components, and a large JLCA substantially contributes to intra-articular deformity. Significant intra-articular deformity, as indicated by a large JLCA, has been shown to be a risk factor for corrective errors in HTO.3,19,20,24 Recent studies on HTO have demonstrated the efficacy of using mathematical formulas such as (JLCA − 2)/2 in the setting of preoperative planning to attain optimal postoperative alignment3,23; however, the influence of JLCA on the accuracy of coronal alignment correction and the relationship between postoperative alignment and clinical outcomes after DLO have not been fully tested or reported.
The purpose of this study was to examine the radiological and clinical outcomes after DLO and in particular to assess the impact of JLCA on the accuracy of alignment correction and surgical outcomes. We hypothesized that corrective errors after DLO will occur and that a large JLCA is a factor leading to unintended postoperative malalignment associated with poor outcomes.
Methods
Study Population and Design
This study was approved by our ethics institutional review board, and written informed consent was obtained from all included patients. For this retrospective study, we included 74 consecutive knees in 51 patients with varus knee OA who underwent DLO at a single hospital between April 2015 and December 2019. All patients had ≥2 years of follow-up clinical and radiological data (mean follow-up period, 49.3 ± 15.3 months; range, 24-89 months).
In our practice, DLO is indicated when there is a combined deformity in the femur and the tibia and the patient wishes to retain high levels of daily activity or continue deep sitting on his or her heels (Japanese-style sitting) regardless of age. Knee osteotomy including DLO is contraindicated for knees with the following clinical factors: flexion contracture >15°, bicompartmental (medial and lateral) OA, inflammatory diseases such as rheumatoid arthritis, and low demands in daily life. Total or unicompartmental knee arthroplasty was adopted as a surgical option in these situations.
Surgical Options and Procedures
Surgeries were performed by a single senior surgeon (H.N.). The decision for surgical indication was made based on the assessment of the whole lower limb alignment and bone/joint geometries. Before surgery, radiological evaluation and surgical planning were conducted on a long-leg weightbearing radiograph using digital planning software (mediCAD; Hectec), as described in our previous study. 25 Preoperative planning included simulation of deformity correction with the aim of restoring the physiological joint line. In patients where the predicted postoperative mechanical medial proximal tibial angle (mMPTA) was ≥95° after correction with HTO alone in the surgical simulation, DLO was considered as a surgical option and the subsequent simulation was performed accordingly. When planning the DLO, the postoperative hip-knee-ankle angle (HKAA) was set to 1° valgus.
Surgery was performed with patients under general anesthesia; postoperative pain control was achieved with peripheral nerve blocks or periarticular local infiltration analgesia. An air tourniquet was not used during surgery. Before the osteotomy, arthroscopic examination and procedures for intra-articular pathologies such as meniscal and chondral lesions were performed as needed. The DLO procedure used in our practice was described in our previous study. 25 Briefly, the surgery began with a lateral closing-wedge distal femoral osteotomy using a minimally invasive biplanar osteotomy technique developed by van der Woude et al. 40 During the initial study period, a TomoFix medial distal femoral anatomical plate (DePuy Synthes) was bent so that it corresponded to the individual's anatomy and was used for femoral fixation. In May 2018, the fixation device was changed to the TriS distal femoral osteotomy plate (Olympus). The femoral osteotomy was followed by a medial opening-wedge HTO using the technique proposed by Lobenhoffer and Agneskirchner. 21 An artificial bone substitute (β-tricalcium phosphate; Osferion 60; Olympus Terumo Biomaterials) was inserted into the osteotomy gap in all cases. During the initial study period, tibial fixation was achieved using the TomoFix medial high tibial plate (DePuy Synthes). The fixation device was changed to the TriS plate (Olympus) in August 2018.
Postoperative Rehabilitation
Immediate postoperative range of motion was allowed without a brace. However, weightbearing was not allowed for 3 weeks after surgery. Partial weightbearing using crutches bearing two-thirds of the patient's body weight was started at 3 weeks, progressing to full weightbearing at 4 weeks. Return to work-related activity such as sedentary and heavy labor was allowed after 2 and 4 months, respectively. Return-to-sports activities was recommended 6 months after surgery, with confirmation of adequate muscle strength and solid bony healing at the osteotomy site.
Radiographic Measurements and Clinical Outcomes
Pre- and postoperative radiological and clinical data were reviewed for data acquisition and subjected to analysis. Clinical outcomes were assessed using the Knee injury and Osteoarthritis Outcome Score (KOOS) preoperatively and 2 years postoperatively. In addition, clinical data relating to subsequent revision surgery were retrieved from patients’ records up to the last follow-up. During the radiological evaluation, Kellgren-Lawrence grade, mechanical lateral distal femoral angle (mLDFA), mMPTA, JLCA, and HKAA were measured for analysis.
In a subgroup analysis of postoperative HKAA, outliers were defined as knees with a deviation of ≥3° from the target postoperative HKAA of 1° valgus, in accordance with the definition adopted by Hasegawa et al 14 and Lee et al. 18 Knees considered outliers were further divided into an undercorrection group (≥2° varus) and an overcorrection group (≥4° valgus) to determine differences in patient characteristics and radiographic and clinical outcomes.
Statistical Analysis
All statistical analyses were performed using JMP (Version 14.0.2; SAS Institute). The normality of data distribution was assessed by the Shapiro-Wilk test. Statistical comparisons between groups were made using the unpaired t test for parametric data, the Mann-Whitney U test for nonparametric variables, and the chi-square test for categorical data, with the significance level set at P < .05.
The relationship between clinical outcomes and radiological parameters was statistically assessed. In addition, we conducted a Pearson correlation analysis for relationships between the preoperative JLCA and the other preoperative radiological parameters, and a receiver operating characteristic (ROC) curve analysis was conducted to identify the threshold of preoperative JLCA as a predictor to discriminate postoperative outliers from nonoutliers. As a predictive parameter, an area under the ROC curve (AUC) of <0.7 was defined as poor, <0.9 as good, and >0.9 as excellent. The Youden index was calculated to identify the most relevant cutoff values.
Interclass correlation coefficients (ICCs) for the intra- and interobserver agreements were calculated to assess the reliability of the radiologic measurements. Intraobserver reliability was assessed for the results measured by a single observer (S.O.) with a 4-week interval between repeated measurements, while the 2 senior orthopaedic surgeons (H.N. and S.O.) independently conducted radiographic measurements to assess interobserver reliability. Intra- and interobserver reliability was assessed for all measurements. The intraobserver ICC values for HKAA, mLDFA, JLCA, and mMPTA were calculated to be 0.97, 0.94, 0.95, and 0.87, respectively, while the corresponding values for the interobserver ICC were 0.97, 0.90, 0.88, and 0.85, respectively. As good to excellent reliability was obtained in all analyses, the results of the measurements taken by a single observer (S.O.) were used for the subsequent analyses.
To assess the statistical power of this study, a 2-tailed post hoc power analysis was conducted using G*Power (Version 3.1.9.6; Franz Faul, Universität Kiel) to compare the postoperative KOOS between the outlier and nonoutlier groups. The results showed that the total sample size of 74 in this study could achieve an adequate power of 1 −β of 0.931, with an α of .05.
Results
The characteristics of the study cohort (N = 74 knees) are summarized in Table 1. Radiological outcomes indicated that the HKAA was significantly corrected from 13.4°± 3.0° varus to 0.5°± 2.8° varus after 2 years (P < .001), indicating a slight undercorrection on average; the mLDFA, JLCA, and mMPTA also improved significantly from preoperatively to postoperatively (P < .001 for all) (Table 2). Regarding clinical outcomes, significant pre- to postoperative improvement was found on the KOOS (from 185.0 ± 71.2 to 387.9 ± 70.5) as well as all KOOS subscales (P < .001 for all) (Table 2). All of the patients underwent hardware removal surgery after confirmation of healing at the osteotomy site; however, no surgery-related complications (eg, deep infection, hinge fracture requiring additional treatment) were encountered during the study period. Pearson correlation analysis indicated a significant association between JLCA and preoperative HKAA (r = −0.647; P < .001) (Table 3).
Characteristics of the Study Cohort (N = 74 knees) a

Values are expressed as No. of knees or mean ± SD (range). BMI, body mass index; K-L, Kellgren-Lawrence.
Comparison of Pre- and Postoperative Radiological and Clinical Results a

Values are expressed as mean ± SD; values in parentheses are ranges. Boldface P values indicate statistically significant difference between groups (P < .05). ADL, Activities of Daily Living; HKAA, hip-knee-ankle angle; JLCA, joint-line convergence angle; KOOS, Knee injury and Osteoarthritis Outcome Score; mLDFA, mechanical lateral distal femoral angle; mMPTA, mechanical medial proximal tibial angle; QoL, Quality of Life; Sport/Rec, Sport and Recreation.
Association of Preoperative JLCA With Other Radiological Parameters a

Boldface P value indicates statistical significance (P < .05). HKAA, hip-knee-ankle angle; JLCA, joint-line convergence angle; mLDFA, mechanical lateral distal femoral angle; mMPTA, mechanical medial proximal tibial angle.
Overall, 22 of the 74 knees (29.7%) were deemed to be outliers at the 2-year follow-up (19 knees [25.7%] in undercorrection, 3 knees [4.1%] in overcorrection). Preoperative and postoperative HKAA and JLCA were significantly higher and 2-year postoperative KOOS significantly worse for outliers than for nonoutliers (Table 4). The majority of outliers (19 of 22 knees) exhibited undercorrection, and clinical outcomes in this group were significantly poorer (Table 5). One patient in the outlier group underwent conversion to total knee arthroplasty after 3 years.
Comparison of Patient Characteristics and Radiological and Clinical Values Between Outliers and Nonoutliers a

Values are expressed as No. of knees or mean ± SD. Boldface P values indicate statistically significant difference between groups (P < .05). BMI, body mass index; HKAA, hip-knee-ankle angle; JLCA, joint-line convergence angle; K-L, Kellgren-Lawrence; KOOS, Knee injury and Osteoarthritis Outcome Score; mLDFA, mechanical lateral distal femoral angle; mMPTA, mechanical medial proximal tibial angle.
Outliers were defined as knees with a deviation of ≥3° from the intended postoperative HKAA (≥2° varus or ≥4° valgus).
Comparison of Demographic, Radiological, and Clinical Values Between Outliers With Under- and Overcorrection a

Values are expressed as No. of knees or mean ± SD. Boldface P values indicate statistically significant difference between groups (P < .05). HKAA, hip-knee-ankle angle; JLCA, joint-line convergence angle; K-L, Kellgren-Lawrence; KOOS, Knee injury and Osteoarthritis Outcome Score; mLDFA, mechanical lateral distal femoral angle; mMPTA, mechanical medial proximal tibial angle. Undercorrection and overcorrection were defined as postoperative HKAA ≥2° varus and ≥4° valgus, respectively.
Regarding the threshold of preoperative JLCA values to predict postoperative outliers, ROC curve analysis showed that a preoperative JLCA cutoff value of 6.0° was significantly associated with postoperative outliers (AUC = 0.742; sensitivity = 68%; specificity = 83%; P < .001) (Figure 1). Patients with a preoperative JLCA of ≥6.0° had a 10.2-fold higher risk of postoperative outliers compared with those with a preoperative JLCA of <6.0° (odds ratio = 10.2; 95% CI, 3.2-32.3; P < .001).
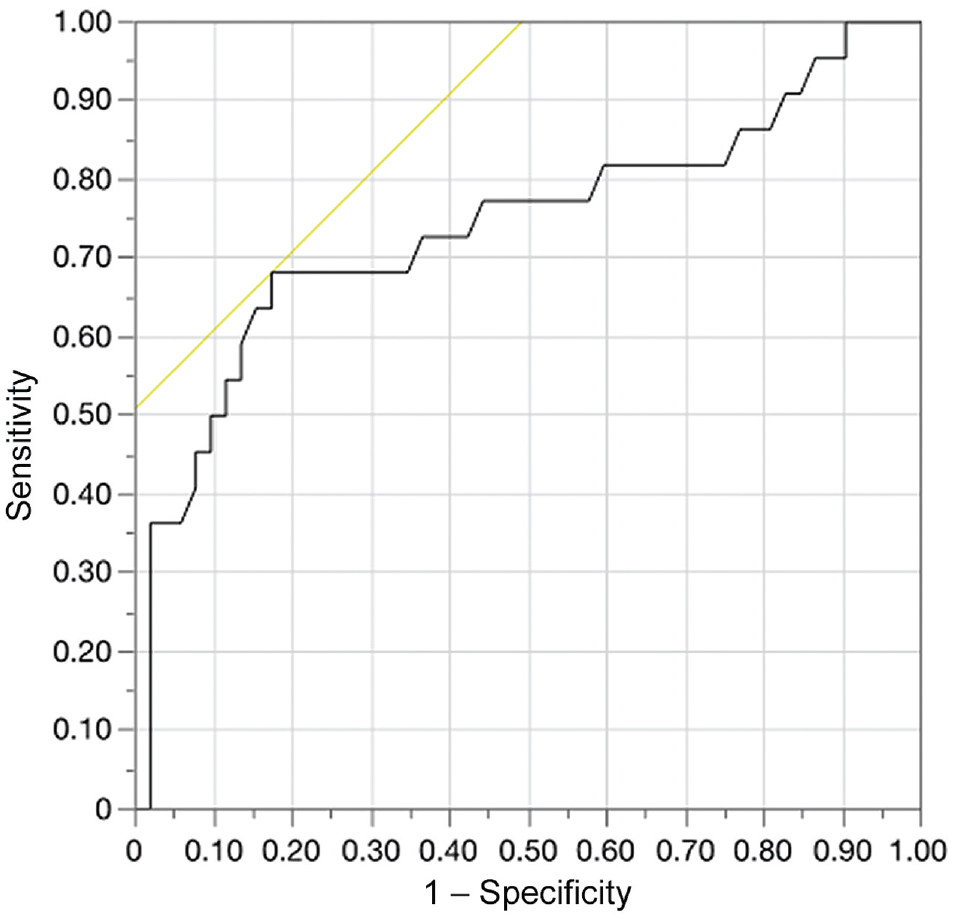
Receiver operating characteristic curve analysis identified the preoperative joint-line convergence angle (JLCA) threshold as a predictor for discriminating between postoperative outliers and nonoutliers in coronal alignment correction. Analysis revealed a preoperative JLCA value cutoff of 6.0°, which was significantly associated with postoperative outliers (area under the receiver operating characteristic curve = 0.742; sensitivity = 68%; specificity = 83%; P < .001).
Discussion
The most important finding of this study was that a preoperative JLCA of ≥6° was found to be a significant prognostic factor affecting the radiological and clinical outcomes in DLO performed for varus osteoarthritic knees. The ROC curve analysis showed that a preoperative JLCA of 6° was the threshold value that compromised the accuracy of deformity correction and resulted in suboptimal postoperative alignment.
Previous studies have shown that accurate alignment correction is important for successful clinical outcomes in HTO performed for varus knee OA.6,11,30 Malalignment in HTO has been reported to be caused by errors in correction of bony deformities or misestimation of postoperative changes in intra-articular deformities. The use of navigation systems and patient-specific instrumentation have been proposed and proven as effective measures to avoid errors in bony correction.31,39,42 However, even with precise bony correction achieved, there are still cases of corrective error.20,35 In those cases, a failure to cope with intra-articular deformities can be a factor in inducing corrective errors, and it has been noted that excessive medial and lateral soft tissue laxity appearing in large JLCAs may be a potential source. Previous clinical studies have shown that a large JLCA is associated with postoperative malalignment after medial opening-wedge HTO.19,20,35,36 However, there have been no studies investigating the relationship between JLCA and DLO surgical outcomes. The present study demonstrated that a large preoperative JLCA was closely correlated with HKAA. Therefore, a larger preoperative JLCA was associated with severe varus alignment, which is consistent with the results of a previous study. 5 The problem of a large JLCA may be more frequently encountered in DLO than HTO, as DLO is indicated for the correction of severe varus deformities.
Comparative analysis between outliers and nonoutliers in this study demonstrated that preoperative JLCA values were significantly higher in outliers, which corresponds with previous study results reported for HTO.3,14,19,24,35 However, in contrast to previous studies where outliers were predominantly overcorrected, the outliers in this study showed more postoperative undercorrection (Figure 2). This difference may be due to the different target HKAA across studies. In our practice, we aim for an HKAA of 1° valgus after DLO, whereas the majority of surgeons conventionally aimed for a postoperative alignment with a weightbearing line ratio of around 62% (more valgus than our target alignment) in HTO.11,19,37 As for target HKAA in DLO, a recent systematic review stated that a valgus HKAA of 0° to 4° has been generally adopted as a target postoperative alignment. 2

Images from a 75-year-old female patient who underwent DLO. (A) Preoperative standing whole-leg radiograph showing a severe varus deformity of the right knee with a JLCA of 7.6°. (B) Intraoperative alignment is confirmed under fluoroscopic guidance to achieve the intended alignment. (C and D) Postoperative standing whole-leg radiograph showing undercorrection, with an HKAA of 5.2° varus and a higher residual postoperative JLCA of 4.8°. DLO, double-level osteotomy; HKAA, hip-knee-ankle angle; JLCA, joint-line convergence angle. mLDFA, mechanical lateral distal femoral angle; mMPTA, mechanical medial proximal tibial angle.
The optimal postoperative alignment for satisfactory clinical results after DLO remains a matter of debate. The current study showed that a postoperative HKAA of 0.4°± 1.4° valgus in the nonoutlier group leads to fairly satisfactory clinical outcomes. In the outlier group, residual varus alignment negatively influenced clinical outcomes, while the overcorrection group exhibited better clinical outcomes compared with the undercorrection group (Table 5). Based on these study results, undercorrection with residual varus alignment should be avoided in DLO.
As stated before, a large JLCA has been noted to be a cause of malcorrection associated with unfavorable outcomes in HTO, and various approaches to avoidance of the correction error have been proposed in previous studies. In preoperative surgical planning of HTO for knees with large JLCA, several studies have addressed the issue of correction planning with weightbearing radiographs.22,29,34,38 To avoid such correction errors, Ogata et al 29 and Shin et al 34 proposed the use of a nonweightbearing supine view for preoperative planning of HTO. Dugdale et al 7 reported the influence of the JLCA on correction angle in the preoperative planning of HTO and recommended subtraction in preoperative calculation to avoid overcorrection in knees with increased lateral joint separation. Other suggestions for improved surgical accuracy include the use of perioperative JLCA change prediction formulae using standing, supine, or stress radiographs.35,38 In particular, recent studies have demonstrated the efficacy of using a simple formula such as (JLCA − 2)/2 to estimate soft tissue correction for prevention of correction error.3,23 However, there is still no standard solution for estimating perioperative JLCA change. Regarding the cutoff value of JLCA as defined in this study, Behrendt et al 3 demonstrated that a JLCA value of ≥4° was a risk factor for overcorrection in HTO. The cutoff JLCA value of 6° in the present study was higher than that used by Behrendt et al, who defined outliers based on the location of the intersection point of the mechanical tibiofemoral axis with the tibial plateau. This difference in definition of outliers may account for the larger cutoff value in the present study.
In addition to soft tissue laxity, substantial cartilage and subchondral bone loss in the medial tibial plateau is another factor that leads to large JLCA. To address this problem, Chiba et al 4 developed the tibial condylar valgus osteotomy, which attempts to improve joint stability and congruity by leveling the eroded medial tibial plateau. 17 However, this osteotomy technique has a limitation in the amount of valgus correction when performed as an isolated procedure. Therefore, further research on surgical modification, including combined osteotomies, may be required to establish an optimal surgical approach based on an accurate understanding of the deformity.
Limitations
There are several limitations regarding the design and contents of this study. First, the study was designed as a case-control study with a relatively short-term follow up. Second, potential factors influencing surgical outcomes other than bone and joint deformities such as intraoperative hinge fractures, osteotomy height and hinge height were not considered in the analysis. However, in regard to hinge fractures, there were no cases with unstable lateral tibial hinge fractures requiring additional treatment in this series. Furthermore, the significance of femoral hinge fractures in closing-wedge distal femoral osteotomy remains unclear with regard to corrective loss of coronal alignment.27,32 Third, status of alignment such as mechanical axis of the lower limb immediately after surgery was not evaluated. Thus, the change in radiological parameters during the postoperative time course could not be figured out. Fourth, knee JLO and compensation for coronal alignment by the ankle and hip joints, which may affect the overall lower limb alignment, were not considered in the analysis. Fifth, although not statistically significant, there were differences in some of the baseline characteristics, such as HKAA and KOOS, between the outlier and nonoutlier groups, which may have induced biases in the comparative analysis between the groups.
Further prospective studies involving a larger sample size are needed to establish optimal management strategies to avoid corrective errors for severe varus osteoarthritic knees with a large JLCA.
Conclusion
A large preoperative JLCA was a significant prognostic factor affecting radiological and clinical outcomes. A preoperative JLCA of ≥6° was found to result in less accurate deformity correction, suboptimal postoperative alignment, and poor clinical outcomes.
Footnotes
Acknowledgements
The authors acknowledge Nicholas Pollifrone for his assistance with the English-language editing for this article.
Final revision submitted February 1, 2024; accepted March 4, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hyogo College of Medicine (ref No. 2218).