
Abstract
Background:
Accurate coronal alignment is crucial in medial open wedge high tibial osteotomy (MOWHTO). Postoperative changes in the joint line convergence angle (JLCA) can cause coronal alignment errors. A preemptive JLCA compensation method has been proposed to address this; however, its clinical value remains unclear.
Purpose:
To assess the accuracy of the preemptive JLCA compensation method for correction angle calculation in MOWHTO.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent MOWHTO for varus osteoarthritis alignment between 2010 and 2024 were reviewed. The patients were classified into 2 groups based on whether the preemptive JLCA compensation method was applied (group 1: the conventional Miniaci method, group 2: the preemptive JLCA compensation method). After propensity score matching for sex, body mass index, hip–knee–ankle (HKA) angle, Kellgren-Lawrence grade, and correction angle on standing radiography, we conducted a comparative analysis of radiologic outcomes (weightbearing ratio) and functional outcomes (Lysholm score and International Knee Documentation Committee [IKDC] scores). Acceptable alignment was defined as a postoperative weightbearing line ratio between 55% and 70%.
Results:
After propensity score matching, 20 patients were included in each group. The mean preoperative HKA angle was varus 6.2°± 2.2° and 6.3°± 2.2° (P = .922), while the correction angle measured by the Miniaci method was 10.0°± 2.1° and 10.3°± 1.7° for the conventional and preemptive JLCA compensation method group, respectively (P = .855). The mean postoperative weightbearing line ratio at 1 year postoperatively was 64.1 ± 7.4 and 62.5 ± 4.7 for the conventional and preemptive JLCA compensation methods, respectively, with no significant difference. However, 95.0% of patients in the JCLA modification group achieved acceptable target alignment, compared with 60.0% (12/20) in the conventional group (P = .014). Despite the significant difference in coronal alignment accuracy, functional outcomes showed no significant difference between the 2 groups.
Conclusion:
The preemptive JLCA compensation method significantly improved correction accuracy, with 95.0% of patients achieving acceptable target alignment, compared with 60.0% with the conventional Miniaci method, although no significant differences in clinical scores were found in the short-term follow-up period.
Medial open-wedge high tibial osteotomy (MOWHTO) is a surgical procedure commonly performed for advanced knee osteoarthritis.3,8,13 This technique aims to achieve a varus-malaligned knee in a mild valgus position, thereby reducing the load on the medial compartment and alleviating symptoms.6,14,18 One key factor for successful outcomes is achieving appropriate postoperative alignment. Target coronal alignment is generally planned such that the weightbearing line passes through the Fujisawa point, which corresponds to 62.5% of the tibial plateau width from the medial edge.1,12,16 Among various methods for calculating the correction angle, the Miniaci method is commonly used to determine the correction angle required to achieve the target alignment.2,21
However, even when the Miniaci method targeting the Fujisawa point is performed with precise radiographic calculations, not all patients achieve appropriate postoperative alignment. This may result from the fact that preoperative measurements consider only bony factors and neglect the condition of the soft tissues. Notably, after realignment of the lower extremity, altered biomechanics changes the force on the surrounding soft tissues of the knee, leading to unplanned, individual variations in the joint line convergence angle (JLCA, the angle between the 2 lines tangential to the femoral condyles and tibial plateau) depending on tissue tightness or laxity. Several studies have attempted to estimate the degree of change in JLCA postoperatively.9,19,20 Recently, Jung et al 5 proposed a formula to predict postoperative JLCA change using preoperative JLCA, JLCA under valgus stress test, and preoperative joint line obliquity, which demonstrated superior predictive accuracy compared with the previous reports (Estimated JLCA change = 0.493 × (JLCA under valgus stress) –0.727 Standing JLCA) + 0.189 × (Joint line obliquity)-1.587). 4 Furthermore, a method for utilizing the estimated JLCA change for the calculation of the correction angle was proposed (preemptive JLCA compensation method). However, previous studies have only simulated the method using postoperative radiographs, and the actual correction-angle results calculated by the proposed preemptive JLCA compensation method have not been reported. Because the JLCA change prediction was based on a correction angle derived from the conventional Miniaci method rather than from the preemptive JLCA compensation method, validation of this new method is necessary. By evaluating the results of the preemptive JLCA compensation method, our study provides clinical evidence supporting a more accurate approach to correcting angle calculations in MOWHTO. We hypothesized that this method would yield a superior clinical outcome.
Methods
This study was approved by the institutional review board, and the requirement for informed consent was waived because of its retrospective nature. The medical records of patients who underwent MOWHTO for advanced osteoarthritis, typically defined as Kellgren-Lawrence (KL) grades 3 and 4, with varus alignment from 2010 to 2024, were retrospectively reviewed. Patients who underwent MOWHTO using correction angle measurement with the Miniaci method targeting the Fujisawa point with or without preemptive JLCA compensation were included. The exclusion criteria were (1) follow-up period of <1 year, (2) hinge fracture confirmed on postoperative radiography, and (3) insufficient outcome data. The preemptive JLCA compensation method was initiated in April 2023, after which all eligible patients were treated using this technique. To apply the preemptive JLCA compensation method, the correction angles were measured on the supine radiograph, weightbearing radiograph with the conventional method, and weightbearing radiograph with the JLCA modification angle. When the preemptive JLCA compensation method yielded a smaller correction angle than that on the supine radiograph, it was considered an outlier and not applied. This was because the supine radiograph reflects lower-extremity alignment without lateral joint opening, a known cause of postoperative JLCA change; thus, the preemptive JLCA compensation method was not utilized. Eligible patients were classified based on whether the preemptive JLCA compensation method was used. Propensity score matching was performed on sex, body mass index (BMI), HKA angle, KL grade, and correction angle on standing radiographs between the 2 methods. A positive value of the HKA angle indicated varus alignment, and the KL grade was defined as a higher grade on full-extension weightbearing anteroposterior (AP) and 45º flexion posteroanterior (PA) views. The final sample included 2 groups based on the correction angle measurement method (group 1, conventional method; group 2, preemptive JLCA compensation method) (Figure 1).

Flowchart for patient inclusion. JLCA, joint line convergence angle.
Surgical Indication
At our institution, the indications for MOWHTO were as follows: (1) age <70 years; (2) advanced osteoarthritis defined as KL grade 3 or 4 on the medial compartment of the affected knee; (3) hip–knee–ankle (HKA) >5°, with positive values indicating varus alignment; (4) absence of advanced osteoarthritis in the lateral and patellofemoral compartment; and (5) no major limitation of range of motion, defined as flexion contracture >15° or active flexion angle <100°.
Correction Angle Measurement by Preemptive JLCA Compensation Method
Before applying the preemptive JLCA compensation method, the estimated JLCA change was calculated using a previously reported formula consisting of JLCA on the 0° knee flexion valgus stress view AP radiograph obtained by applying 150 N using a Telos stress device (vgJLCA0), JLCA on a standing AP radiograph (preJLCAstd), and preoperative joint line obliquity (preJLO) (Figure 2). Both JLCA and preJLO were defined as positive values when the lateral apex or inclination was directed laterally.

Measurement of the (A) preoperative JLCA under valgus stress radiograph, and (B) preoperative standing JLCA (angle between the yellow lines) and JLO (angle between the blue lines, with the lower blue line representing the line parallel to the ground). JLCA, joint line convergence angle; JLO, joint line obliquity.
The estimated JLCA change was calculated by applying the variables to the formula reported by the previous study (estimated ΔJLCA = 0.493 × (vgJLCA0) − 0.727 × (preJLCAstd) + 0.189 × (preJLO) − 1.587). 4 After calculation, the tibia and the fibula were rotated on the weightbearing whole lower extremity radiography using ImageJ software (National Institute of Health Image). Specifically, the tibia and fibula were rotated by the estimated JLCA change, using the midpoint of the tibial spine as the rotation center. The correction angle was measured on the rotated image using the Miniaci method. When the correction angle measured on the rotated image was between the correction angles on supine and standing radiographs, a 3-dimensional patient-specific instrument (3D PSI) gapper (Kneevigate, Skyve) was created after simulating the correction using Mimics software (Version 17; Materialize) for segmentation, and OnKnee-U software (Skyve) for simulation (Figure 3).

Correction angle measurement using the preemptive JLCA compensation method. Before the measurement, the estimated JLCA is calculated. (A) The midpoint of the tibial spine (tip of the yellow arrowhead), the Fujisawa point (62.5% of the tibia plateau, red asterisk), the target hinge area (tip of the blue arrow), and the ankle center (green circle) are marked. The area including the whole tibia and fibula is marked (red line). (B) The marked area is rotated to the degree of estimated JLCA change (0.493 × vgJLCA0− 0.727 × preJLCAstd+ 0.189 × preJLO − 1.587) in accordance with the previously reported formula toward the direction of valgization, with the center of rotation being the midpoint of the tibial spine. (C) After the rotation, the correction angle is measured using the Miniaci method. (D) MOWHTO to the degree of the planned correction angle is simulated, and the 3D PSI gapper is printed according to the simulated data.
Surgical Procedure and Rehabilitation
A single senior orthopaedic surgeon performed all procedures (S.-H.K.). Before osteotomy, diagnostic arthroscopy and concomitant procedures for cartilage and meniscal lesions were performed. After arthroscopy, an osteotomy was performed. A longitudinal incision was made midway between the anterior and medial borders of the tibia, and the pes anserinus was partially detached to expose the osteotomy site. The osteotomy level was set 4 cm below the joint line from the starting point, confirmed on fluoroscopy, with the hinge point located in the upper one-third of the proximal tibiofibular joint, as described in the previous study. 4 Gap distraction was performed using the adjustable bone spreader. For the preemptive JLCA compensation method, a 3D PSI gapper was used to maintain the gap during plate fixation. 5 The detached pes anserinus was reattached by embedding it under the locking plate.
Patient Evaluation
Descriptive data, subjective functional scores, and radiological data were retrospectively analyzed. The descriptive data included age, sex, height, weight, and BMI.
Radiological variables included both pre- and postoperative variables. The HKA angle, weightbearing line ratio, KL grade of the medial compartment on full extension weightbearing AP and 45º flexion PA views at each follow-up period, and correction angle measured on weightbearing whole lower extremity radiography by the Miniaci method were included. For patients in group 2, additional measurements of the correction angle on supine whole-lower-extremity radiographs were performed. Two experienced physicians (J.B. and S.-H.J.), blinded to each other's results and group allocation, independently measured the radiological variables. The intraclass correlation coefficient (ICC) was calculated to assess interobserver reliability.
Subjective functional outcomes were assessed, including the visual analog scale (VAS) for Pain, Lysholm score, International Knee Documentation Committee (IKDC) subjective score, Knee injury and Osteoarthritis Outcome Score (KOOS), and Western Ontario and McMaster Universities (WOMAC). These scores were prospectively reported preoperatively, at 6 months postoperatively, and annually thereafter. Thresholds of minimal clinically important difference (MCID) for the VAS, IKDC subjective, Lysholm, KOOS symptoms, KOOS Pain, KOOS activities of daily Living (ADL), KOOS Sports/Recreation, KOOS Quality of Life (QoL), and WOMAC scores were derived from a distribution-based method, applying 0.5 standard deviation to define meaningful clinical improvement (14.8, 7.8, 10.2, 10.2, 9.7, 8.6, 13.6, 9.7, and 8.0, respectively).
Ethical Approval
This study was approved by the institutional review board (IRB) of Severance Hospital, and the requirement for informed consent was waived owing to its retrospective nature (IRB No. 4-2025-0285).
Statistical Analysis
An a priori power analysis was performed to determine the minimum sample size for each group. Based on the reported proportion of overcorrection patients from another method to reduce overcorrection, 9 and comparing with a previous study analyzing the change of JLCA, a minimal number of patients for adequate power was 19 patients for each group for the significance level (alpha) and power (1 – beta) set as .05 and 0.8, respectively. 4 For the propensity score matching, the MatchIt package in R Version 4.4.1 (R Core Team, R Foundation for Statistical Computing) was used. All statistical analyses, except propensity score matching, were conducted using SPSS Version 26 (IBM Inc). For continuous variables, normality was confirmed using the Shapiro-Wilk test. The student t test for normally distributed data and the Mann-Whitney U test for non-normally distributed data were used for between-group comparisons. For categorical variables, the Pearson chi-square test or the Fisher exact test was used. The Pearson correlation test was used to analyze the correlation. Statistical significance was set at P < .05.
Results
A total of 117 patients were included in this study after excluding 2 patients, resulting in a lower correction angle derived from the JLCA modification than from the correction angle on the supine radiograph. Among the included patients, 97 underwent correction using the conventional method (group 1), and 20 using the preemptive JLCA compensation method (group 2) (Figure 1). No significant differences were found in the descriptive data (Table 1). At 1-year postoperatively, 95.0% of group 2 patients achieved acceptable alignment, which was significantly higher than that in group 1 (60.0%), while other pre- and postoperative radiographic variables did not differ significantly between the groups (Table 2). The reliability of the radiological measurements for continuous variables was good to excellent, with ICC values 10 ranging from 0.883 to 0.936. For categorical variables, reliability was assessed 11 as having substantial agreement, with kappa values of 0.684 and 0.730.
Comparison of Baseline Demographic Data and Intraoperative Data a

Values are presented as mean ± SD or number of patients. Group 1, the conventional Miniaci method; Group 2, the preemptive JLCA compensation method. BMI, body mass index.
Comparison of Radiologic Outcomes a
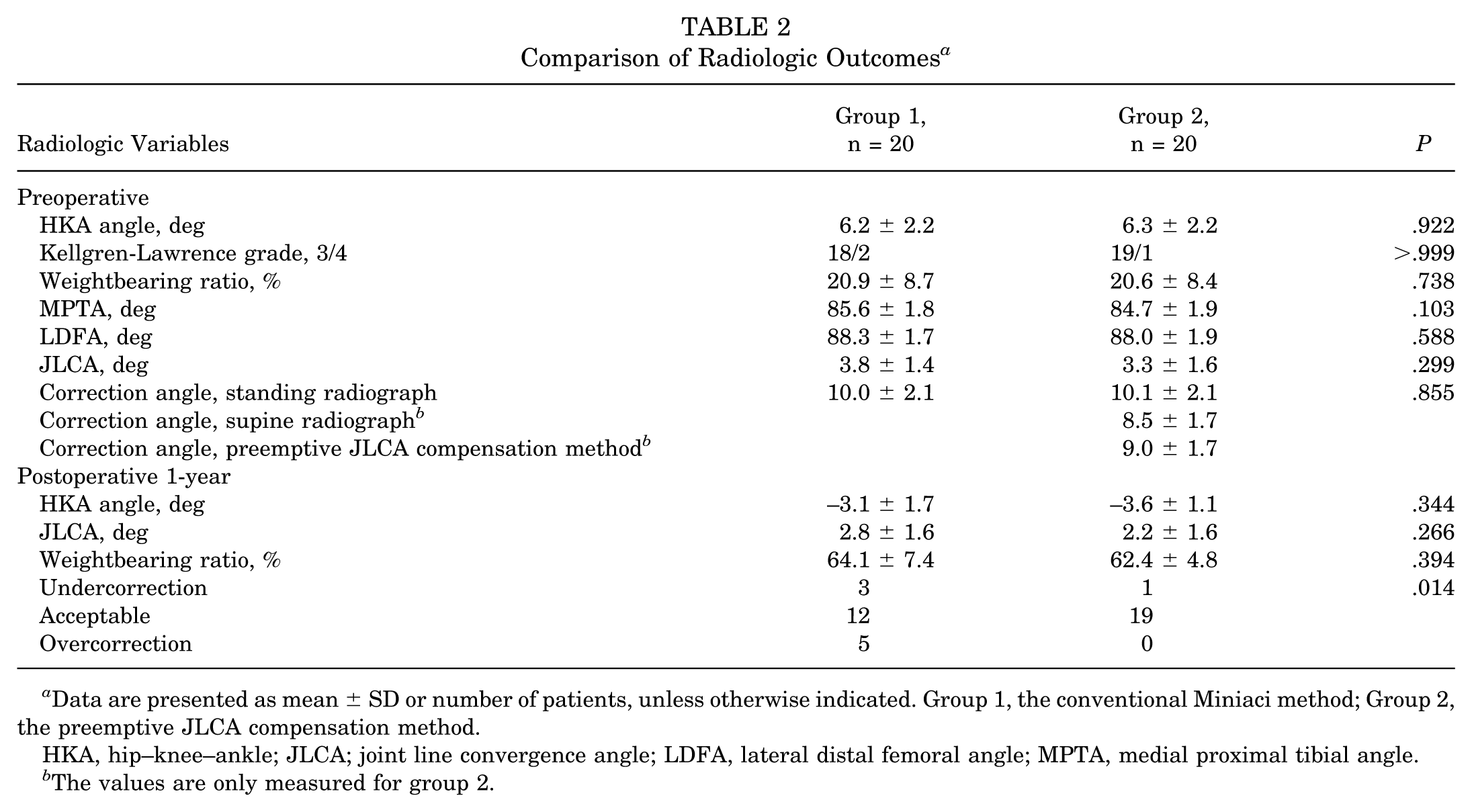
Data are presented as mean ± SD or number of patients, unless otherwise indicated. Group 1, the conventional Miniaci method; Group 2, the preemptive JLCA compensation method.
HKA, hip–knee–ankle; JLCA; joint line convergence angle; LDFA, lateral distal femoral angle; MPTA, medial proximal tibial angle.
The values are only measured for group 2.
Subjective functional outcomes were also not significantly different between the 2 groups. Furthermore, the proportion of patients who achieved improvement beyond the MCID did not differ significantly between the 2 groups (Table 3).
Comparison of Clinical Scores a

Data are presented as mean ± SD, unless otherwise indicated. Group 1, the conventional Miniaci method; Group 2, the preemptive JLCA compensation method. ADL, activities of daily living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MCID, minimal clinically important differences; Postop, postoperative; Preop, preoperative; QoL, quality of life; Sport/Rec, sports/recreation; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities.
Values are presented as the number of patients.
Comparison with the corresponding preoperative variables.
In group 2, the correlation between the estimated JLCA change and the actual change from the preoperative period to 1 year postoperatively was analyzed. The mean estimated JLCA change was 1.0°± 0.9°, whereas the JLCA change at 1 year postoperatively was 1.1°± 1.5°. No significant correlation was found between the estimated changes and the changes at 1 year postoperatively (r = 0.337; P = .146).
Discussion
The main finding of this study was that the preemptive JLCA compensation method achieved superior accuracy, with 95.0% of patients attaining acceptable postoperative alignment, compared with 60.0% with the conventional method.
One of the most crucial goals of MOWHTO is to achieve the target coronal alignment postoperatively, as previous studies have reported adverse outcomes under or overcorrection.7,12,15 However, not all patients undergoing MOWHTO achieve acceptable alignment, and therefore several previous studies have reported methods for more accurate correction.9,20 Among them, Shin et al 20 reported that, for the conventional method of correction angle measurement, using supine radiographs rather than standing radiographs resulted in better accuracy. 20 This could be attributed to changes in the weightbearing line after surgery; postoperative varus alignment causes medial dominant loading and increased JLCA during weightbearing, whereas lateral shift of the loading axis postoperatively reduces this effect. 17 Both the supine radiography method and the preemptive JLCA compensation method aim to adjust the correction angle by taking the effect of soft tissue into account. However, the preemptive JLCA compensation method has its strength in that it could reflect the effect of weightbearing adequately, whereas supine radiography neglects it as a whole. Nevertheless, the correction angle from supine radiography remains important for the preemptive JLCA compensation method. Considering that the supine radiography method entirely excludes the influence of soft tissue during weightbearing, any patient who had a lower degree of correction angle measured by the preemptive JLCA compensation method compared with supine radiography was regarded as an outlier in predicting JLCA changes; thus, the preemptive JLCA compensation method was not applied in such cases. Further studies are required to achieve a more accurate realignment for patients with a smaller correction angle using the preemptive JLCA compensation method than using the supine radiography method.
A previous study that reported the estimated JLCA change used in our method retrospectively simulated postoperative radiographs based on the calculated JLCA change. 4 However, such retrospective simulations have limited clinical applicability because they cannot account for JLCA changes associated with reduced correction angle. Notably, the actual JLCA change and estimated value did not have a significant correlation when applying the correction angle of the preemptive JLCA compensation method. The mean difference of 1.1° between the correction angle from standing radiography and the preemptive JLCA compensation method could be a cause of this insignificance. Despite its insignificance, the proposed preemptive JLCA compensation method still has its strength for accurate correction, resulting in an acceptable range in 95.0% of patients. Therefore, the clinical implication of the current preemptive JLCA compensation method is to accurately correct coronal alignment rather than estimate the change in JLCA.
Another factor influencing correction accuracy is the use of 3D PSIs. Because the JLCA medication method adjusts the correction angle in 0.1° increments, 3D PSI plays a crucial part in the process. Although the superior outcome for group 2 patients in achieving target alignment could stem from the use of 3D PSI, 3D PSI itself did not result in superior postoperative coronal alignment. The proportion of patients achieving acceptable postoperative alignment did not significantly differ between group 1, which included patients with and without the application of 3D PSI, and the patients enrolled in the previous study, which only included patients with 3D PSI, showed no significant differences (Appendixtable A3). Considering these results, the superior outcome of the preemptive JLCA compensation method is more likely to stem from the method itself rather than the utilization of the 3D PSI.
Limitations
This study had some limitations. First, its retrospective nature introduced a potential risk of selection bias owing to the study design. Second, although the proposed method demonstrated high accuracy, a few patients showed a lower correction angle with the preemptive JLCA compensation method than with supine radiography. Thus, the preemptive JLCA compensation method was not utilized. Further studies are needed to identify alternative treatment methods for these patients. Third, although the discrepancy and nonsignificant correlation between the estimated and actual JLCA change could be attributed to the degree of modification after applying the preemptive JLCA compensation method, the potential clinical implications warrant further studies. Fourth, this study included only short-term follow-up, and further research should assess long-term outcomes. Fifth, although the number of patients per group exceeded the minimum required by the a priori power analysis, the overall sample size remained relatively small.
Conclusion
The preemptive JLCA compensation method significantly improved correction accuracy, with 95.0% of patients achieving acceptable target alignment, compared with 60.0% with the conventional Miniaci method. However, no significant differences in clinical scores were found in the short-term follow-up period.
Footnotes
Appendix
Comparison of Postoperative Coronal Alignment With Regard to the Utilization of 3D PSI a

| Radiologic Variables b | Group 1
c
|
Previous Study
d
|
P |
|---|---|---|---|
| Postop coronal alignment e | .879 | ||
| Undercorrection | 3 | 7 | |
| Acceptable | 10 | 29 | |
| Overcorrection | 7 | 25 |
Group 1, the conventional Miniaci method; Group 2, the preemptive JLCA compensation method. MOWHTO, medial open wedge high tibial osteotomy; Postop, postoperative; PSI, patient-specific instrument; 3D, 3-dimensional.
Values are presented as the number of patients.
Including patients both with and without the application of 3D PSI.
All included patients had undergone MOWHTO using 3D PSI.
Acceptable alignment defined as 62.5% ± 6.25%, to compare with the result of previous study.
Final version submitted November 26, 2025; accepted December 12, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: Kyoung-Tak Kang is the Chief Executive Officer of Skyve and Clevion Co, Ltd. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval for this study was obtained from Severance Hospital (IRB No. 4-2025-0285).