
Abstract
Background:
Growth-specific physical characteristics in adolescence may mediate throwing-related loads and movement patterns associated with elbow injuries. In a previous study, the authors calculated the forearm-hand inertia, which is the moment of inertia centered at the elbow joint.
Purpose:
To determine the relationship of forearm-hand inertia values with throwing motion patterns and elbow valgus load in adolescent baseball players.
Study Design:
Descriptive laboratory study.
Methods:
A total of 35 adolescent baseball players underwent measurements by dual-energy x-ray absorptiometry (DXA) scans and a throwing trial. Forearm-hand inertia was determined as the joint moment around the elbow using the subregion analysis mode of DXA. Elbow valgus torque and ball speed during throwing were measured using a dedicated sensor and speed gun, and throwing efficiency was calculated by dividing the elbow valgus load by the ball speed. Players were divided according to the throwing motion pattern in which maximum acceleration occurred: pelvis–upper arm–forearm (proximal-to-distal sequencing [PDS] group; n = 19) or pelvis-forearm–upper arm (proximal upper extremity [PUE] group; n = 16). The groups were compared in terms of ball speed, elbow valgus torque, throwing efficiency, and forearm-hand inertia using t tests and analysis of covariance, with forearm-hand inertia as covariates. The chi-square test was used to examine the relationship between throwing motion patterns and forearm-hand inertia.
Results:
The PUE group had a higher elbow valgus load (effect size [ES] = 0.65; P = .03), throwing efficiency (ES = 0.63; P = .02), and forearm-hand inertia values (ES = 0.64; P = .04) than the PDS group. In addition, a significant relationship was observed with throwing patterns when forearm-hand inertia values were 350 kg·m2 (OR, 2.36; 95% CI, 1.09-5.12; P = .012) and 400 kg·m2 (OR, 1.68; 95% CI, 0.99-2.85; P = .037).
Conclusion:
Study results indicated that growth-specific physical characteristics in adolescent baseball players exhibited in forearm-hand inertia mediated the relationship between high elbow valgus and poor throwing efficiency caused by poor throwing motion patterns.
Clinical Relevance:
A better understanding of the details in muscle function with throwing mechanics may prevent future injuries.
Throwing-related elbow injury commonly occurs among adolescent baseball players. Otoshi et al 25 reported that more than half (54.3%) of adolescent Japanese baseball players aged 6 to 17 years have experienced elbow pain. Prospective cohort studies have revealed that elbow injury occurs in approximately 25% of pitchers.15,22 Risk factors include overuse due to year-round throwing, 24 inadequate rest throughout the season, 41 and playing in multiple leagues. 19 Conversely, in addition to the playing and pitching frequency11,18 and player position,15,32 modifiable factors, such as poor posture, flexibility of lower extremity muscles, 9 and poor throwing biomechanics, 13 can contribute to throwing-related elbow injury. Such injuries continue to occur among baseball players,15,18,19,32 and more knowledge is needed regarding their prevention and treatment.
Throwing mechanics are believed to be risk factors for throwing elbow injuries. Anz et al 3 reported that the magnitude of the elbow valgus torque at the late cocking phase was correlated with the incidence of throwing injury among professional baseball pitchers and suggested that throwing mechanics are a risk factor for elbow injuries. Therefore, an understanding of the throwing motion is essential to prevent elbow injuries in baseball players.
Rauch et al 29 reported that the growth pattern of each joint segmentation of the extremities proceeds peripherally during the youth stage. In addition, because body proportions, including adult, and youth mass ratios, differ, the ratio of length to mass in each segment varies throughout the growth period. Considering the throwing technique of a baseball player, the heavier mass distal to the elbow joint is presumed to be a factor in increasing the elbow load. According to a report investigating the relationship between the elbow valgus torque during throwing and the segment mass of the upper limb using dual-energy x-ray absorptiometry (DXA), the elbow valgus torque is positively correlated with the mass of the hand and forearm. 38 In a previous study by our author group, 40 we calculated the forearm-hand inertia, which is the moment of inertia centered at the elbow joint, using the region analysis mode in DXA, and found that the peak increase in forearm-hand inertia on the throwing side is approximately at 12 years of age. Furthermore, the throwing mechanism during youth is also specific, with a small elbow flexion angle 12 and peak acceleration timing distal to the elbow and preceding that of the proximal region. 36 Thus, growth-specific physical characteristics in adolescence may mediate the throwing-related load and movement patterns associated with elbow injuries.
In the current study, we examined the relationship of forearm-hand inertia values with throwing motion patterns and elbow valgus load in adolescent baseball players. We hypothesized that the components of the relationship between throwing motion patterns and elbow torque in adolescent baseball players would involve growth-specific physical variables.
Methods
Participants
Included in this study were 35 adolescent baseball players (30 right-handed and 5 left-handed, 7 pitchers and 28 fielders) aged 13 to 15 years who belonged to the Pony League, a competitive league for junior high school students, and practiced baseball at least twice a week on weekends. The throwing motion of all participants was the overthrow, or three-quarter pitch. All participants were healthy and had no injuries at the time of this study (August 2021). The protocol for this study received ethics committee approval, and the participants and their guardians received a detailed explanation of the experimental procedure and risks of the research before participation, after which written informed consent/assent was obtained.
Assessment Procedures
The measurements were composed of DXA scans and a throwing trial, which were performed over 2 days. During DXA, the participants’ height and weight were measured with their clothes but no shoes using a stadiometer to the nearest 0.1 cm and a digital scale to the nearest 0.1 kg. All participants underwent the DXA measurements before the throwing trial. The throwing trial was conducted in an outdoor baseball ground maintained under standard environmental conditions.
DXA Measurement
Whole-body DXA scans were performed using a Hologic QDR-series densitometer and analyzed using Version 12.4.3 of the accompanying software after calibration by qualified personnel. The participants were placed in the supine position so that the midline of the body coincided with the centerline of the examination table. The supine posture involved the following: the shoulder joint at 45°, the forearm pronated, the hip and knee fully extended, and the feet fixed such that the toes were in contact with one another and did not move during scanning. The subregion analysis mode of DXA was used for data analysis. We collected the data, which were compartmentalized to the smallest region of interest and arranged at constant intervals, from the elbow joint that passes through the lateral epicondyle of the humerus to the end of the fingers on the throwing side. 40 Based on the procedure for calculating the moment of inertia as reported by Ganley and Powers, 14 the integrated value of the square of the mass in each section and the distance from the center of the elbow joint were calculated as the forearm-hand inertia value.
Throwing Trial
A total of 20 body markers were attached to major landmarks for motion capture and biomechanical analysis. These markers were attached bilaterally to the distal end of the toe, lateral malleolus, lateral femoral epicondyle, greater trochanter, anterior and posterior inferior iliac spine, lateral tip of the acromion, and lateral humeral epicondyle on both sides. Additionally, 2 markers were placed on the radial and ulnar styloid processes of the throwing arm. The players were then fitted with a motusBaseball sensor and sleeve (Motus Global) to evaluate the elbow valgus load. The sensor was placed on the medial aspect of the ulna, 5 cm distal to the medial epicondyle of the humerus (Figure 1).
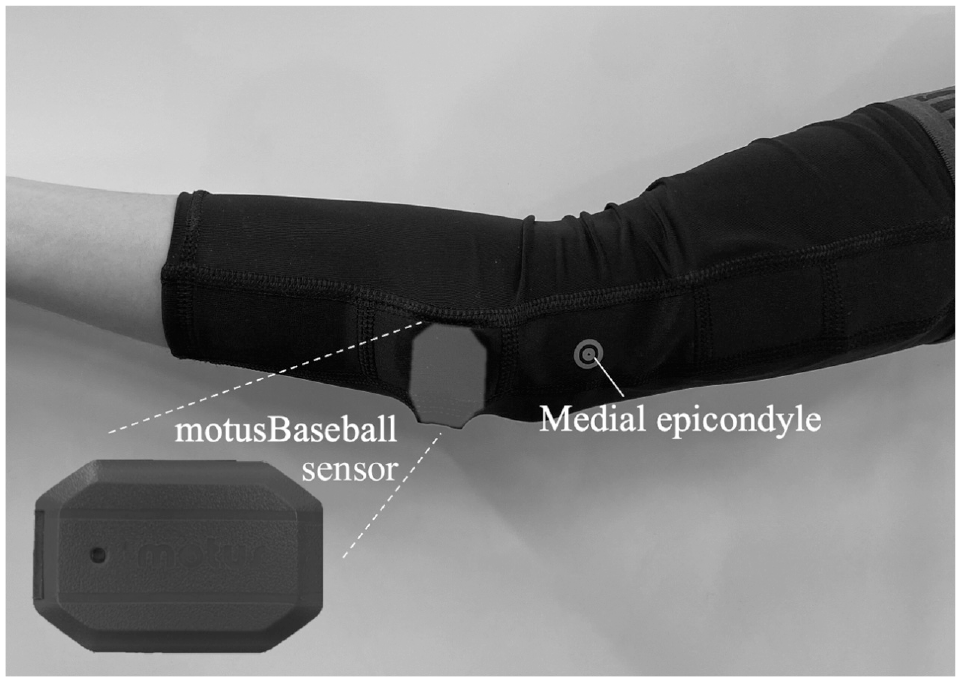
Attachment position of the motusBaseball sensor.
After performing a simple warm-up, including dynamic stretching, running, and throwing for about 20 minutes, the throwing trial was performed. The players threw balls from a basic mound that was 18.44 m from home base (Figure 2). The players were instructed to throw with maximum effort and aim at the center of the strike zone. Motion data were collected using 3 high-speed cameras at 240 Hz (Gig-E; Q'sfix Corp) placed on the batter's side, back, and front (obliquely).

Assessment of the throwing motion.
The throwing trials involved 3 throws to the strike zone, and the fastest strike throws that could be measured using the radar gun were analyzed as representative data for each player. Data on the elbow valgus were collected via Bluetooth to an iOS device (Apple Inc) using standard-issue device software. 5 Previous studies have shown that the Motus sensor obtains measurements that correlate well with laboratory measurements4,5 and provides precise and reproducible data.20,23 Because ball speed and elbow valgus load are positively correlated,17,31 throwing efficiency was calculated by dividing the elbow valgus load by the ball speed.
Classification of Throwing Motion Patterns
The throwing V motion was analyzed using Frame Dias V motion analysis software (DKH). The coordinate system was designed with the x-axis in line with the throwing direction and the z-axis as the vertical direction, while the y-axis was determined as the cross product of the z- and x-axes. Because we were interested in the timing of kinetic sequencing distal to the elbow, we included the pelvis, upper arm, and forearm in the analysis based on the assessment of 5 parameters (pelvis, trunk, upper arm, forearm, and hand) as described by Scarborough et al. 36 The pelvic segment consisted of the midpoints of the anterior and posterior inferior iliac spine on each side, and the direction was from the nonthrowing to the throwing side. The upper arm segment was measured from the lateral tip of the acromion to the lateral humeral epicondyle markers on the throwing side. The forearm segment was measured from the lateral humeral epicondyle to the midpoint of the radial and ulnar styloid process markers on the throwing side.
The biomechanical variables measured included maximum angular velocity of the pelvis, upper arm, and forearm segments, calculated as the square root of the sum of the 3 planar velocities of the sagittal, frontal, and transverse planes for each segment. This definition of angular segment velocity was derived from previous studies that investigated kinetic sequencing, including those for overhead throwing and the golf swing. 28 Thus, the kinematic sequence was defined as the timing of the peak of each segment's total angular velocity. The analysis of the throwing motion included the phase from the maximum knee height on the nonthrowing side to ball release. Digitizing was performed on the landmarks necessary for the analysis.
The players were classified according to the throwing motion pattern in which the maximum acceleration occurred: the pelvis–upper arm–forearm sequence (defined as the proximal-to-distal sequencing [PDS] group) or the pelvis-forearm–upper arm sequence (defined as the proximal upper extremity [PUE] group).
Statistical Analysis
A statistical power analysis was conducted for sample size estimation. Based on previous studies, the estimated intragroup standard deviation of elbow valgus in youth baseball players was 5 N·m, 30 and the estimated difference between the PDS and PUE groups was approximately 5 N·m. 35 Therefore, we calculated that a minimum of 12 players in the PUE group was needed to achieve 80% power and an alpha of .05.
The participants’ chronological age, height, weight, baseball experience, ball speed, elbow valgus load, and forearm-hand inertia were analyzed using descriptive statistics (mean ± standard deviation). After confirming data normality, the t test was performed to compare differences in ball speed, elbow valgus load, throwing efficiency, and forearm-hand inertia between the PDS and PUE groups. In addition, to assess the effects of forearm-hand inertia, 1-way analysis of covariance with the Bonferroni post hoc test was performed to analyze the ball speed, elbow valgus load, and throwing efficiency, with forearm-hand inertia as the covariate. Effect size (ES) was calculated for each analysis. The criteria for interpreting the magnitude of the ES were >0.2 (small), >0.6 (moderate), >1.2 (large), and >2.0 (very large). 16 In addition, we analyzed the relationship between throwing motion pattern and forearm-hand inertia using the chi-square test. The cutoff values for forearm-hand inertia were based on the mean and standard deviation of the participants in this study and our previous study 40 and were set at 300, 350, and 400 kg·m2.
For all statistical analyses, the level of significance was set at P < .05. All data were analyzed using SPSS for Windows (Version 28.0; IBM Corp).
Results
There were 19 players in the PDS group and 16 players in the PUE group; thus, the minimum sample size needed to achieve 80% power was achieved. All participants had at least 1 year of baseball experience. Table 1 shows the descriptive data of the participants overall and according to study group. There were no significant differences in the descriptive characteristics between the PDS and PUE groups. Furthermore, we found no group differences in the descriptive characteristics between pitchers and fielders or right-handed and left-handed players.
Participant Characteristics, Ball Speed, Elbow Valgus, and Forearm-Hand Inertia Values a
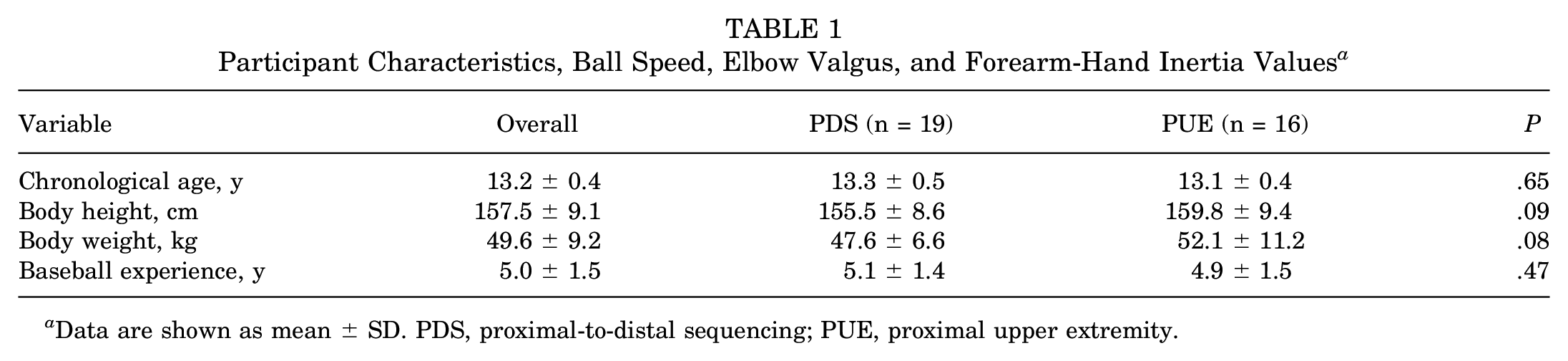
Data are shown as mean ± SD. PDS, proximal-to-distal sequencing; PUE, proximal upper extremity.
Table 2 shows the differences in ball speed, elbow valgus load, throwing efficiency, and forearm-hand inertia between the 2 throwing motion patterns. The t test showed that the PUE group had a higher elbow valgus load (ES = 0.65; P = .03), throwing efficiency (ES = 0.63; P = .02), and forearm-hand inertia values (ES = 0.64; P = .04) than the PDS group. Furthermore, when comparisons were conducted using analysis of covariance with forearm-hand inertia as the covariate, no significant differences in any of the variables were found between the PDS and PUE groups.
Differences in Ball Speed, Elbow Valgus Load, Throwing Efficiency, and Forearm-Hand Inertia Values Between Throwing Motion Patterns a

Data are shown as mean ± SD. Boldface P values indicate a statistically significant difference between groups (P < .05). ANCOVA, analysis of covariance; ES, effect size; PDS, proximal-to-distal sequencing; PUE, proximal upper extremity.
Covariate: forearm-hand inertia.
Table 3 presents the relationship between forearm-hand inertia classified according to cutoff point and throwing motion pattern. A significant relationship was observed with throwing patterns when forearm-hand inertia values were 350 kg·m2 (OR, 2.36; 95% CI, 1.09-5.12; P = .012) and 400 kg·m2 (OR, 1.68; 95% CI, 0.99-2.85; P = .037).
Relationship Between Throwing Motion Pattern and Forearm-Hand Inertia a

Boldface P values indicate statistical significance (P < .05). OR, odds ratio; PDS, proximal-to-distal sequencing; PUE, proximal upper extremity.
Discussion
Our results revealed that although the PUE group indicated higher throwing efficiency and elbow valgus torque than the PDS group, forearm-hand inertia mediated both relationships (ES = 0.64, P = .04). In addition, a significant relationship was observed with throwing patterns when forearm-hand inertia values were 350 kg·m2 (OR, 2.36; 95% CI, 1.09-5.12; P = .012) and 400 kg·m2 (OR, 1.68; 95% CI, 0.99-2.85; P = .037). The present study is the first to clarify the relationship of growth-specific physical characteristics with throwing motion patterns and elbow valgus load. Although previous studies have reported the relationship between elbow valgus torque and upper limb mass in youth baseball players, 38 and that the moment of inertia around the elbow corresponds to the period of maximum height increase during adolescence, 40 how these correlations mediate actual throwing motion patterns and elbow load have not been established.
Given that pelvic and trunk rotation and timing deviations in peak angular velocity during throwing have been reported to increase stress on musculoskeletal structures in the throwing arm and increase the risk of injury,2,6,27 evaluation of the kinematic sequence pattern of the throwing motion might also be clinically useful. Scarborough et al 34 found no trials that demonstrated the proposed 5-segment, proximal (pelvis)–to–distal (hand) sequence in pitching trials in high school and older baseball players, with the most frequently performed sequence being the pelvis, trunk, arm, hand, and forearm. Throwing motion was analyzed in this study by considering the forearm and hand as a single segment in addition to the pelvis and upper arm. We found that 45.7% (16/35) of adolescent baseball players were classified as belonging to the PUE group. In a previous study that classified the throwing trials of 30 baseball players in high school and higher levels into kinematic sequences, 35.8% (81/226) of the players were classified with the PUE pattern, which started from the pelvis. 36 Based on the findings of previous studies, adolescent baseball players may be more likely to exhibit the peripheral precedence throwing pattern. The results of the present study indicated that the PUE group had higher forearm-hand inertia values than the PDS group. Furthermore, forearm-hand inertia values were associated with throwing motion patterns when the cutoff point for inertia was set at 350 kg·m2, and the PUE group included players with high forearm-hand inertia values. Fleisig et al 13 speculated that the ball size relative to a player's physical characteristics and body size may play a role in the throwing motion pattern of youth baseball players. Thus, the state of physical growth of the player may also affect their throwing motion pattern.
Previous studies have considered that a greater elbow valgus torque might increase throwing-related elbow pain.7,18 Thus, investigating ways of reducing the elbow valgus load during throwing is necessary. We found that the PUE group had greater elbow valgus torque than the PDS group, which is consistent with previous studies, 36 although the age and playing level of the participants differed. Considering that Fleisig et al 13 showed that elbow valgus torque increases with age and level, modifying poor throwing motion patterns may be a consistent issue in reducing elbow injuries in baseball players. Interestingly, however, when we adjusted forearm-hand inertia values as covariates for differences in elbow valgus torque and throwing efficiency between the PUE and PDS groups, no differences were found between the 2 groups. These findings suggest the possibility that a physical growth characteristic influenced by peripheral advanced growth patterns on limbs 29 may mediate the relationship between the throwing motion pattern and elbow valgus torque in adolescent baseball players.
Given that exercises specifically designed for improving upper limb muscle hypertrophy are rarely performed during adolescence (the participants specifically train only in baseball), retroactively modifying the forearm-hand inertia values would likely be difficult. In other words, modifiable factors related to elbow injury risk should be assessed, especially in adolescent baseball players, who are undergoing the period of maximum increase in forearm-hand inertia values. 40 Sakata et al 33 applied interventions in 9 stretching programs and 9 strength exercises in youth baseball players aged 8 to 11 years and revealed that the intervention group had fewer medial elbow injuries than the nonintervention group. This means that improvement in physical function may reduce elbow load. Downs et al 8 found that increased upper arm length is a risk factor for adolescent baseball players, indicating the need to develop a program that considers the physical characteristics specific to adolescence. Particularly because the function of the shoulder girdle muscles appears to help support the upper limbs and reduce the elbow load during the throwing motion, 10 an approach to improving the function of the shoulder girdle muscles may be essential for adolescent baseball players.
Ball speed is one factor that predicts elbow load, as some studies have suggested a positive relationship between ball speed and elbow valgus torque.26,37 Although the PDS group was presumed to exhibit an efficient kinetic chain and higher ball speed, no difference in ball speed was observed between the PDS and PUE groups in this study. Manzi et al 21 reported that pitchers with a proper sequence had the fastest ball velocity. Presumably, the difference in the age and level of the participants in the current study may have contributed to the difference in results from those of previous studies. Aguinaldo and Escamilla 1 found that trunk power generated during throwing predicts ball speed. In addition, Takei et al 39 reported that an increase in trunk lean mass occurs during adolescence when peak height velocity occurs. In other words, the trunk lean body mass of adolescent baseball players is still undergoing growth, and throwing mechanics alone may not explain ball speed.
Limitations
Our study has several limitations. First, the throwing trial was conducted only 3 times because of the limited time schedule. Second, the study cohort all came from a single baseball team. Thus, extrinsic factors, such as practice time and loads that may be related to throwing mechanics, were not investigated. Analyzing the throwing mechanics of adolescent baseball players in other populations and follow-up studies are necessary to understand the relationships between player physique and elbow load. Last, this study did not determine whether there is a relationship of forearm-hand inertia with throwing-related injuries. In the future, prospective follow-up and clarification of the relationships of forearm-hand inertia with throwing motion pattern and elbow injury will help identify any causal relationship.
Conclusion
Our study demonstrated that growth-specific physical characteristics in adolescent baseball players exhibited in forearm-hand inertia mediated the relationship between high elbow valgus and poor throwing efficiency caused by poor throwing motion patterns. This finding may be specific to adolescent baseball players and provides an important consideration in the development of programs for throwing injury prevention. In addition, considering the difficulty of modifying the forearm-hand inertia retroactively, the study findings may encourage clinicians and coaches to focus on improving muscle function, such as the scapular stabilizing muscles, which play a crucial role in supporting the upper extremity during throwing. A better understanding of the details of muscle function with throwing mechanics may prevent future injuries.
Footnotes
Acknowledgements
The authors sincerely thank the players who participated in this study. They also thank Chiaki Hakkei, the head coach of one of the baseball teams.
Correction (October 2024):
Article updated to correct the Acknowledgment section.
Final revision submitted February 8, 2024; accepted February 26, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded in part by a grant from the Japan Sports Medicine Foundation (2021). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Waseda University (ref No. 2021-218).