
Abstract
Background:
Anconeus compartment syndrome is a rarely reported compartment syndrome in the anconeus muscle compartment of the forearm. It has anatomic and pathophysiological associations with posterolateral rotatory instability (PLRI) of the elbow.
Purpose:
To present the history, management, and outcomes of 4 patients with anconeus compartment syndrome. Secondary aims were to (1) establish normative anconeus pressures and (2) measure the volume of this compartment with and without PLRI in cadavers.
Study Design:
Case series; Level of evidence, 4.
Methods:
Four patients with clinical signs of anconeus compartment syndrome (2 gymnasts, 1 swimmer, and 1 footballer/weightlifter) were identified over a 3-year period (2015-2017 inclusive). Patient history, sporting activity, physical examination, anconeus compartment pressures, and treatment outcomes were recorded. Manometry of the anconeus compartment in 2 healthy male controls was performed to establish normative compartment pressures. Anconeus volumetric anatomy and the effect of creating PLRI on compartment volume was investigated in 4 cadaveric elbows.
Results:
All 4 patients had microtraumatic PLRI, and 2 patients had anconeus hypertrophy. Anconeus compartment pressures at rest and at 2-minutes postexercise were median 28.0 and 67.5 mm Hg, respectively, in the patients and mean 16.5 and 18 mm Hg, respectively, in the controls. Simultaneous fasciotomy and PLRI reconstructive procedures were performed in 2 patients, with outcomes showing full return to competition. Fasciotomy alone was performed in 2 patients to allow return to competition, with both requiring later reconstruction to address PLRI. Cadaver dissection revealed that the anconeus compartment was extremely small and that creation of PLRI reduced the direct volume of the compartment and increased the distance between the anconeus origin and insertion.
Conclusion:
Our case series demonstrated that anconeus compartment syndrome can occur in upper limb-dominant athletes in the presence of PLRI and anconeus hypertrophy. Pain is relieved by fasciotomy, but definitive treatment of the underlying instability prevents further symptomatology.
The anconeus is a small triangular muscle that runs along the posterolateral aspect of the elbow. It originates on the posterior surface of the lateral epicondyle of the humerus and inserts distally on the posterosuperior surface of the ulna and the lateral aspect of the olecranon. The deep aspect of the anconeus adheres closely to the lateral joint capsule, lateral collateral ligament (LCL), and humeroulnar joint.2,30 It is innervated by a branch of the radial nerve. 22
There is ongoing debate on the exact function of anconeus. 3 The penniform architecture of the anconeus (fibers arising obliquely along a tendinous expansion like a feather) indicates that it is more suited for generating force rather than displacement of a joint segment. 11 Consequently, there are suggestions that the anconeus serves primarily as a dynamic stabilizer of the lateral elbow,4,20,30,33 with minimal contribution to elbow extension (15%). 49 Because of its location and orientation, a primary function of the anconeus may be to protect the passive elbow constraints, such as ligaments and joint capsule, by contributing to posterolateral stability.3, 6, A disruption to the common extensor origin (CEO) and LCL results in increased elbow varus and posterolateral elbow instability. 20 Posterolateral rotatory instability (PLRI) of the elbow occurs when the radius and ulna rotate externally in relation to the distal humerus, leading to posterior displacement of the radial head relative to the capitellum. 10 PLRI is often the result of direct trauma and subsequent disruption to the LCL and CEO; however, microtraumatic PLRI may occur due to chronic attenuation of the lateral ligament complex in long-standing cubitus varus. 17 Factors such as repetitive and high loads to the LCL and CEO (such as in gymnastics or with prolonged use of elbow crutches), as well as congenital hyperlaxity may propagate the symptoms of nontraumatic PLRI. 10 Tensioning of the anconeus has been shown to restore the stability of the LCL- and CEO-deficient elbow,3,26 indicating its importance as an active restraint to PLRI. The anconeus may also assist in the screw-home mechanism of the radial head on the capitulum through arcs of motion at the elbow. 21
Compartment syndrome is characterized by pain from an increase in intracompartment pressure within an osteofacial envelope, which may be caused by intrinsic swelling or an external compression. The mechanism of injury may be traumatic or nontraumatic. 29 The upper extremity compartments have typically been divided into the shoulder and arm (brachium), forearm (antebrachium) and hand compartments; however, the anconeus may be an independent compartment.29,30 The triceps extensor expansion is continuous with the anconeus compartment fascia. 25
Chronic exertional compartment syndrome (CECS) is a reversible ischemic state related to an increase in tissue pressure within the confines of a sealed facial space during exercise.23,43 This pathological increase in interstitial tissue pressures can result in pain, local muscle weakness, cramping, and/or fatigue. 23 There are a number of theories on the origin of symptoms, including muscle deoxygenation, a disproportionate oxygen supply versus demand, and stimulation of sensory or intramuscular pressure fibers within the compartment. 43 CECS has been commonly reported in the lower limb,16,46 with infrequent reports in the flexor compartment in the upper limb.8,15,24 In the upper limb, it has been reported secondary to sports such as swimming, rowing, and motorcycling.18,38,47
Anconeus compartment syndrome is a variation of the upper limb compartment syndromes, which, to date, has been reported only in 2 patients, including a carpenter and a typist.2,39,41 In these studies, anconeus compartment pressures were reported in symptomatic patients; however, no published normative pressures for the anconeus compartment exist. Last, there has been no suggested mechanism of injury for anconeus compartment syndrome. In our clinical practice, we have observed exertional lateral elbow pain in the presence of PLRI in athletes performing high repetitions of upper limb weightbearing or high elbow rotational loads.
The primary aim of this study was to present the history, management, and outcomes of 4 patients with anconeus compartment syndrome. The secondary aims were to (1) test anconeus compartment pressures in healthy control volunteers before and after exercise to establish normative values to compare with those with anconeus compartment syndrome and (2) measure the volume of this compartment with and without the creation of PLRI in cadavers to assist in developing a hypothesis surrounding the mechanism of injury of this condition.
Methods
Patients With Anconeus Compartment Syndrome
Ethical approval for this study was granted, and it was conducted by 2 experienced upper limb surgeons (G.H., P.J.) and 1 experienced upper limb sports physician (T.J.). Patients with exercise-induced lateral elbow pain were identified as potential participants for this study over a 3-year period (2015-2017 inclusive). The patient-reported history (including occupation- and sport-related activity) and physical examination tests (particularly for PLRI; including the posterolateral rotatory drawer, pivot-shift, and push-up tests) were recorded in the patient's clinical notes. 9 PLRI was defined as a pathological increase in posterior radial head translation in association with symptom reproduction. Treatment selection was based on the individual patient pathology. Return-to-activity status was recorded.
To measure anconeus compartment pressure, manometry of included participants was performed by an experienced pressure tester (P.J.) using a Stryker STIC pressure monitor and slit catheter system (Figure 1). Ultrasound was used to confirm the positioning of the inserting needle and thus the catheter position within the compartment. Both resting and postexercise pressures (at 2 minutes) were measured. Exercise consisted of resisted elbow extension cycles and elbow weightbearing rotation cycles.

Measurement of compartment pressures in patients with exertional elbow pain.
Normative Anconeus Compartment Pressures
Manometry of 2 healthy male volunteers (G.H. and P.J.; controls) was used to establish normative anconeus compartment pressures using the same testing procedures as described for the patients. Pressure readings were recorded at 5 timepoints: initial measurement, resting, exercise, 1 minute postexercise, and 2 minutes postexercise.
Volumetric and PLRI Assessment in Cadavers
We performed cadaver dissections of the anconeus in 4 elbows of 2 cadavers (obtained from the anonymous donor program at the University of Melbourne). On 1 side of each cadaver, using a Kocher approach, an incision was made centrally over the anconeus compartment. The anatomic boundaries of the anconeus compartment and relationships to the lateral ulnar collateral complex were noted. The length of the origin and insertion of the anconeus muscle was measured at rest and after recreating PLRI (see the following) by sectioning the humeral origin of the capsuloligamentous attachments of the lateral ulnar collateral complex.
The compartment volume was measured both directly (muscle volume) and indirectly by fluid volume replacement. For the direct determination of volume, the anconeus muscle was dissected out of the compartment en bloc without violating the floor of the compartment. The direct volume was measured in a syringe with air expelled. For the indirect measure, after the excision of contents, the compartment was then sealed and injected with saline (Figure 2). No computerized evaluation of soft tissue volume was available when these patients were seen.

Fluid injection in a cadaveric specimen for measurement of compartment volume after muscle excision and fascial closure.
We also sought to determine whether posterolateral instability would affect the volume of the anconeus compartment. After reflecting the anconeus muscle and exploring the floor of the compartment, the elbow capsule was released longitudinally. Second, the undersurface of the extensor carpi radialis brevis (ECRB) fascia was released. Third, the lateral structures were sequentially sectioned, looking at the shape of the compartment and the subsequent compartment volume. The capsule alone was sectioned first, followed by the anterior common extensor origin, and finally the posterior floor (which makes up the “lateral ulnar collateral complex” of O’Driscoll) until the radial head became subluxated and deformed the anconeus compartment in rotation, reducing its volume (see Figure 3 and Supplemental Video). Although we simulated the dynamic process of PLRI passively in cadavers, the use of cadavers to infer human elbow instability mechanisms has been done previously.12,40

Radiocapitellar joint in a cadaveric specimen opened (A) without posterolateral subluxation and (B) with subjective posterolateral subluxation, showing the radial head impinging in the anconeus space.
Data Analysis
Manometry results of the patients and normative controls were reported using descriptive statistics: medians for sample sizes from 3 to 25 and means for sample sizes of 2 or >25 with a normal distribution. 35
Results
The characteristics, anconeus compartment pressures, and results of treatment of the 4 included patients are outlined in Table 1. Three of the patients were elite Olympic-level athletes, and 1 was a local, part-time Australian Football League player. All patients were male. The median age of symptom onset was 23.5 years (range, 21-25 years). The median anconeus compartment pressures at rest and 2 minutes postexercise were 28.0 and 67.5 mm Hg, respectively. All patients had microtraumatic PLRI, and 2 patients demonstrated significant anconeus hypertrophy on the affected compared with the unaffected side.
Patient Characteristics, Compartment Pressures, and Treatment Outcomes a
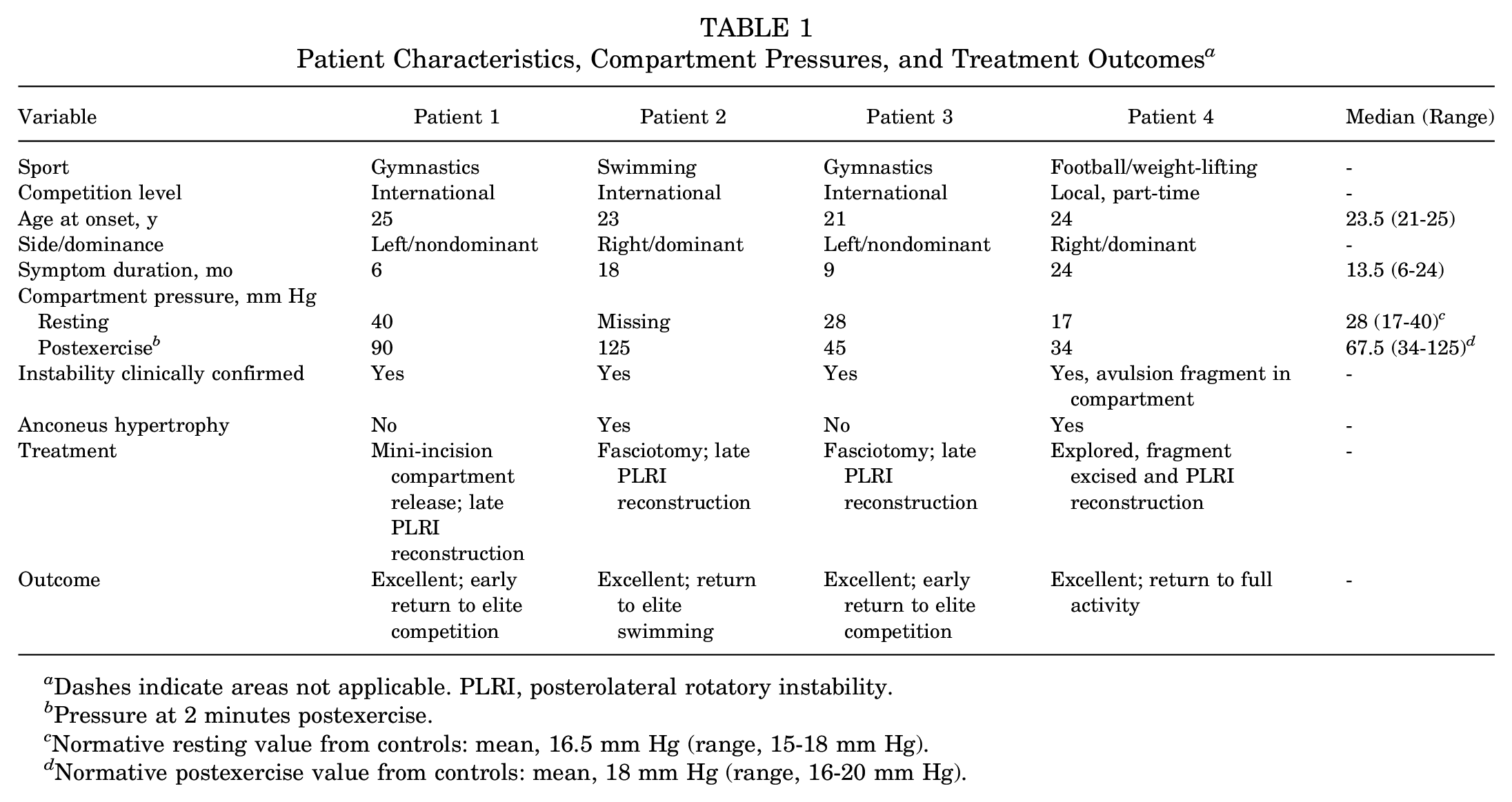
Dashes indicate areas not applicable. PLRI, posterolateral rotatory instability.
Pressure at 2 minutes postexercise.
Normative resting value from controls: mean, 16.5 mm Hg (range, 15-18 mm Hg).
Normative postexercise value from controls: mean, 18 mm Hg (range, 16-20 mm Hg).
Patient 1
A 25-year-old international-level gymnast presented with a 6-month history of increasing posterolateral elbow pain while using the pommel. The patient was participating in a heavy gymnastic training cycle, with a career objective event in a few months’ time. The history of pain developing after commencement of activity and continuing through cooling down suggested the possibility of a compartment syndrome. Examination demonstrated PLRI.
Electromyography (result normal) and pressure studies showed a pre-exercise pressure of 40 mm Hg and a postexercise pressure of 90 mm Hg, confirming the primary diagnosis of anconeus compartment syndrome. A mini-incision compartment release was performed. Immediate relief was obtained, and the patient returned to the near full training schedule within a week of surgery. The patient won the high bar at the next world championship. This specialty event utilizes massive traction and rotation forces on the elbow in 1-armed high-bar loops.
The patient required further follow-up 18 months later because of ongoing stress on the anteromedial coronoid with posterolateral subluxation and eventually underwent a lateral ligament reconstruction of the elbow to address the underlying PLRI, with full return to competition.
Patient 2
A 23-year-old, right-hand dominant, international-level swimmer presented with pain over the posterolateral aspect of both elbows. The pain became worse as the duration of a swim training session or event increased and continued through cooling down. Pain was particularly noticeable during the pull-through of each stroke. The patient had undergone an extensive conservative therapy program, including rest, massage, and corticosteroid injection. Tenderness was demonstrated over both anconeus muscle bellies, especially after swim training.
On examination, the patient demonstrated anconeus hypertrophy as well as PLRI of the elbow, without significant generalized ligamentous laxity. PLRI testing reproduced some (but not all) of symptoms. A magnetic resonance imaging (MRI) scan displayed increased signal in the triceps and biceps distal muscle bellies, without frank anconeus or lateral elbow pathology. Compartment pressures were measured and confirmed the condition, with peak pressures of 125 mm Hg.
The patient underwent surgical decompression of the anconeus muscle. At decompression there was significant bulging of the muscle (Figure 4). The patient underwent a simultaneous lateral ligament reconstruction of the elbow for the PLRI (Figure 5). At 6 weeks, the patient had gained significant confidence and subjective strength in the elbow. Subsequent return to full training showed significant improvements in pain and swimming performance. The patient was able to return to the elite swimming level.

Bulging of the anconeus muscle.

Lateral ligament reconstruction. LCL, lateral collateral ligament; LUCL, lateral ulnar collateral ligament.
Patient 3
A 21-year-old international-level gymnast (all-around rather than individual apparatus) presented with a suggested diagnosis of anconeus compartment syndrome. This patient had a much shorter history of pain, with only a mild increase in compartment pressures (28 mm Hg at rest compared with 20 mm Hg in the unaffected side, increasing to 45 mm Hg after exercise) on testing compared with the other patients. Examination demonstrated PLRI.
To facilitate early return to competition, the patient initially underwent fasciotomy only and returned to win a medal at subsequent world championships. However, 34 months later he was re-evaluated with ongoing posterolateral instability symptoms. The patient eventually underwent a posterolateral reconstruction without complication and with good results.
Patient 4
A 23-year-old patient participating in local football combined with a heavy gymnasium weight program presented with anconeus hypertrophy and pain over an 18-month period. History included a fall on the elbow some years before. Examination revealed tenderness over the humeral epicondyle, PLRI, and exercise-induced pain into the anconeus that settled with rest. MRI scans showed an avulsed fragment of bone from the lateral humeral epicondyle lying in the anconeus compartment.
Surgical exploration allowed fasciotomy, excision of the fragment, and lateral ulnar collateral ligament (LUCL) advancement to reconstruct the LUCL complex. The patient had complete relief and returned to full activity.
Normative Anconeus Compartment Pressures
Anconeus compartment pressures in the controls are demonstrated in Table 2. Resting pressure was extremely variable. The insertion of the required fluid in testing sent the “initial peak” pressure well into what would be called pathological in standard studies, but after 1 minute, the pressure came down to the resting level of a mean 16.5 mm Hg. The mean peak 1-minute postexercise pressure was 35 mm Hg, and the pressure returned to a mean level of 18 mm Hg after 2 minutes, which is considerably longer than when testing lower limb compartment pressures. 7
Normative Anconeus Compartment Pressures in Controls (n = 2)

Initial pressure, anconeus compartment pressure taken soon after the participant entered the examination room; At rest, anconeus compartment pressure taken when the participant was actively resting before exercise.
Anconeus Volume and PLRI Assessment in Cadavers
Anatomic Findings
The anconeus muscle is a pyramidal shape, enveloped by a stout fascial sleeve with an apex at the posterolateral humeral border immediately posterior to the common extensor origin and therefore in direct proximity to the lateral ulnar collateral “complex” (Figure 6). This fascia was confirmed as continuing as an expansion of the lateral triceps tendon. Its anterior border is the raphe at the posterior margin of the common extensors of the forearm. The shape of the anconeus compartment acts like a stretched bag, as lengthening of the ends of the muscle unit decreases the volume of the compartment and increases pressure. 6

Anconeus fascia opened in a cadaveric specimen to show the anconeus muscle and radiocapitellar joint.
Compartment Volume
The direct muscle volume of the anconeus was approximately 8.0 mL in cadaver 1 and 7.0 mL in cadaver 2. The indirect measure (compartment sealed and injected with saline) was again approximately 8.0 mL in cadaver 1 and 7.0 mL in cadaver 2.
Anatomic Response to Posterolateral Instability
Reflecting the anconeus muscle from its compartment did not lead to an appreciable increase in radial head translation with passive supination of the forearm. Releasing the elbow capsule longitudinally, again, did not lead to an appreciable increase in radial head translation. Releasing the undersurface of the ECRB fascia did lead to an appreciable increase in posterolateral translation of the radial head with passive supination (see Supplemental Video). The radial head moved posterior to the capitellum, directly impinging on the floor of the anconeus compartment fascia. Further dissection of lateral structures continued to increase the translation of the radial head until effective PLRI resulted.
The length of the anconeus from the anterior margin of the origin to insertion on the supinator crest of ulna was measured at 9.2 cm at rest in 2 of the elbows. After performing the sectioning at the humeral epicondyle, the rotatory subluxation of the forearm produced a lengthening of the muscle compartment from prefixed markers of 0.6 cm (6.5%) which significantly alters the length-tension ratio of the muscle in that lengthened state. This reduces the effective volume with the intrusion of the radial head into the compartment area.
Discussion
This study revealed the presence of exertional anconeus compartment syndrome in 4 patients who participated in repetitive, upper limb-dominant sporting activities. All 4 athletes had PLRI, and 2 athletes had significant clinical anconeus hypertrophy. The median anconeus compartment pressures at rest and at 2 minutes postexercise were 28.0 and 67.5 mm Hg, respectively. The range of resting and postexercise pressures of the patients was wide; however, this may be due to variations in elbow anatomy, 28 physiological adaptations that occur during different types of training loads, 27 and the severity of the compartment syndrome itself. 23 Pedowitz and colleagues 32 concluded that in the presence of clinical findings, a pre-exercise pressure of ≥15 mm Hg and a 1-minute postexercise pressure of ≥30 mm Hg may be diagnostic of CECS. This criterion was met by all participants in our study. In comparison, the mean anconeus compartment pressures at rest and at 2 minutes postexercise for the controls were 16.5 and 18 mm Hg, respectively. Although the sample size across patients and controls was too small for direct statistical comparison, the obvious difference in resting and postexercise compartment pressures between the 2 groups, in conjunction with the diagnostic criteria for CECS,32,44 supports the likelihood of anconeus compartment syndrome in these athletes. All 4 patients with anconeus compartment syndrome experienced resolution of symptoms and return to sport with fasciotomy and stabilization of their PLRI, supporting the diagnostic accuracy of the condition.
In this study, cadaveric resection further strengthened the biological plausibility of this condition, particularly in association with PLRI. We found that the volume of the anconeus compartment was 7 to 8 mL, which is extremely small when compared with other muscle compartments, 14 leaving it susceptible to large pressure increases with small changes in volume. 34 We confirmed that the anatomy of the anconeus compartment includes borders that are in close proximity to structures affected by elbow instability syndromes. Releasing the undersurface of the ECRB fascia did lead to an appreciable increase in posterolateral translation of the radial head with passive supination. The volume of this compartment was further decreased by intrusion of the radial head into the anconeus with the posterolateral rotation of the radioulnar unit on the humerus, such as occurs with PLRI, suggesting that PLRI may increase anconeus compartment pressures in vivo.
Anconeus compartment syndrome occurs when the volume of this small compartment is reduced, often resulting in a pathophysiological increase in the interstitial pressure. 29 This can result in lateral elbow pain and reduced performance of the distal upper limb.1,39,41 To date, anconeus compartment syndrome has been rarely reported in the literature. Steinmann and Bishop 41 reported on anconeus compartment syndrome in a typist. The patient had a preassessment pressure of 24 mm Hg, with little change pre- and postexercise, and had a good response to surgical release. A lack of confirmed elevation of compartment pressures raises questions over whether the surgery alone alleviated pressure or whether scarring may have contributed some concurrent unrecognized elbow instability. PLRI was only first described by O’Driscoll et al 31 in 1991, and thus Steinmann and Bishop may not have considered the effect of PLRI on the anconeus compartment at the time of their study.
Abrahamsson et al 1 reported anconeus compartment syndrome in the dominant arm of a carpenter in 1987. They demonstrated preoperative pressures ranging from 27 to 236 mm Hg. This is consistent with the labile pressures we noted on pressure testing in healthy controls. The compartment was then exposed under local anesthetic and a wick inserted. The patient exercised with the elbow in extension and experienced unbearable pain after 5 minutes, with the pressure rising to 464 mm Hg in the compartment. A 2 cm-wide fascial resection was performed. The patient's symptoms improved, yet the pressure reached as high as 108 mm Hg on subsequent testing. However, the amount of fluid inserted during testing was not reported, and in the present study, we have shown that small volume changes can result in large pressure changes.
Although this condition is rarely reported in the literature, anconeus compartment syndrome may be more prevalent among certain athletes performing high repetitions of upper limb weightbearing in the presence of PLRI. Traction of the elbow with rotational forces may be the initial mechanism of developing LUCL laxity - a phenomenon typical in gymnasts performing high-bar training and routines.10,17 LUCL laxity may progress to symptomatic PLRI in the presence of microtrauma, such as can occur with high training loads and local muscle fatigue. 5 In addition, subsequent pommel use may lead to hypertrophy of the anconeus in an attempt to aid the “screw-home mechanism” of the elbow in extension for weightbearing. 13 We suspect that the posterolateral laxity compromises the screw-home ability of the elbow so that weightbearing is more difficult in full extension. In swimming, traction of the radial head occurs with a posterolateral force in the recovery phase of the freestyle stroke but with much less force than in a gymnast. It is possible that preexisting intrinsic posterolateral laxity (either congenital or posttraumatic) is required for this process to begin. 5 Full extension and the screw-home mechanism is still required for the commencement of stroke in strenuous training and competition. The floor of the anconeus compartment includes a broad surface of the ulna and over 50% of the radiocapitellar capsule posterior to the midline, thus making the floor of the compartment partially responsible for posterolateral stability. If PLRI occurs on a recurrent basis in vivo, stressing the floor of the anconeus compartment, it may induce an increased pressure in that compartment.
Anconeus hypertrophy may also reduce compartment volume and increase compartment pressures. Anconeus hypertrophy may occur due to high, repetitive upper limb loads42,48 and, we postulate, may even be a secondary response to PLRI. High, repetitive elbow loads in cubitus varus that occur with gymnastic events such as pommel and parallel bars require high eccentric loads from the anconeus as it actively stabilizes the posterolateral elbow in a lengthened position. 36 PLRI may further increase the eccentric demand on the anconeus, as our results suggest that inducing PLRI in cadavers increases the length-tension ratio of the muscle by 6.5%. Repetitive eccentric load has been shown to induce greater muscle hypertrophy compared with concentric loads. 37 Hence, the mechanisms of repetitive and high cubital varus load, as well as PLRI, may result in clinically significant anconeus hypertrophy. Increased muscle volume (ie, hypertrophy) causes an increase in internal pressure in the fascial compartment. 43 Gymnasts who repetitively place full weightbearing loads through the elbow, often on a background of generalized hyperlaxity, may be particularly susceptible to anconeus compartment syndrome. Other sports that use resistance in rotation (eg, swimming freestyle) may also develop this condition.
Overuse injuries as a result of an increase in training intensity and duration may contribute to the development of CECS.19,23,43 Repetitive microtrauma leads to intercellular and extracellular tissue damage, ranging from the development of scar tissue to tissue degeneration. 23 These characteristics of overuse injuries have been observed in athletes when they increase their training intensity and duration. Intercellular and extracellular tissue damage can impair the normal function of the myofascial compartment, particularly during exercise. 50 Therefore, CECS may occur when the physical demands on the athlete increase at a faster rate than the body can adapt. 23 CECS may become more prevalent as previously amateur athletes become professional or as athletes transition from semiprofessional to professional competition. 45 It is possible that other pathogenic mechanisms become apparent in sports with high training loads. In the meantime, measuring compartment pressure in the anconeus compartment will allow diagnosis of more patients with this unusual combination of conditions.
All 4 study patients responded well to fasciotomy. Two had fasciotomy alone but later demonstrated signs of PLRI hinting at the pathogenetic mechanism. Of these 2 patients, 1 also had a bone fragment in the anconeus compartment, adding to the volume restriction. Subsequent surgery to address PLRI and the bone fragment in these 2 patients led to good results, with full return to activity. The 2 other patients underwent fasciotomy combined with posterolateral elbow reconstruction at the first operation, which would release the compartment even if the exertional compartment condition was not recognized. We suspect that some patients with this condition are treated without recognizing the associated condition.
Limitations and Strengths
A limitation of this study was that it is a small case series of 4 patients and 2 controls; however, as anconeus compartment syndrome is rare, reporting on a large case series would be difficult. In addition, controls were not matched for age or athletic activity. Last, the baseline anconeus pressure was missing for patient 2. Given the importance of the overall clinical picture of this rare condition, the decision was made to include this patient despite the missing value. A strength of this study was that it is the first to report on more than 1 patient with anconeus compartment syndrome. All included patients had clinical histories and objective findings that were similar (ie, high upper limb weightbearing loads and PLRI), allowing us to hypothesize on the likely mechanisms responsible for this condition, which has not been done previously. Furthermore, this was the first study to investigate the anatomic and volumetric characteristics of the anconeus compartment along with the creation of PLRI, supporting the biological plausibility of anconeus compartment syndrome as a condition in association with PLRI.
Conclusion
We reported a case series of exertional anconeus compartment syndrome, with all patients demonstrating associated microtraumatic PLRI, which may indicate the underlying pathogenesis of this rare condition. Sports involving high and repetitive upper limb loads and/or rotation forces as well as subsequent anconeus hypertrophy may also contribute to this compartment syndrome. Fasciotomy to relieve the pressure on the anconeus compartment led to good outcomes; however, any PLRI should also be addressed to avoid revision surgery. We postulate that as training loads for athletes continue to rise in different sports, the recognition of this condition is an important differential diagnosis of lateral elbow pain in athletes.
Footnotes
Correction (November 2024):
Article updated online to correct the article type to Original Research.
Final revision submitted December 18, 2023; accepted February 23, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: G.H. has received grant support from Arthrex and Johnson & Johnson, speaking fees from Johnson & Johnson and Smith+Nephew, and hospitality payments from Wright Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Avenue Hospital (project No. 204).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.