
Abstract
Background
Among the causative lesions of lateral elbow pain, atraumatic posterolateral rotatory instability (PLRI) is a rare condition, but it produces pain and disability to the elbow. It still lacks published specific treatment literature. According to the development of arthroscopy, the arthroscopic lateral collateral ligament (LCL) imbrication can possibly be an alternative minimal invasive procedure that can eradicate the atraumatic PLRI.
Level of evidence
Case Series (Level of evidence: 4).
Keywords
Introduction
Chronic lateral elbow pain can be resulted from many pathologies such as lateral epicondylitis, pathological plica, cartilage lesion, posterolateral impingement, and atraumatic posterolateral rotatory instability (PLRI).1,2 Theoretically, the atraumatic PLRI can be caused by repetitive abnormal load onto the lateral collateral ligament (for example, tardy PLRI and chronic use of crutches), 3 steroid injection inducing,1,4 and chronic lateral epicondylitis.4,5 Chronic repetitive abnormal load to the lateral collateral ligament and the steroid injection inducing were commonly reported and concerned in recent practice.1,3,4 The instability symptoms usually occur during pivot activities such as pushing up or rising up from a chair.
In many literature reviews on surgical treatment, the lateral ulnar collateral ligament reconstruction using tendon graft provides excellent results in both traumatic and atraumatic PLRI.1,4–11 However, its disadvantages were invasive procedure, morbidity to donor graft site, and the need for re-training of the joint proprioception, with non-innervated graft.
The arthroscopic imbrication of the lateral collateral ligament can improve the posterolateral rotatory stability by re-tightening the lateral collateral ligament onto its humeral insertion.4,12–15 Despite the development of arthroscopic techniques, there have been very few studies of the arthroscopic technique specific for patients with atraumatic PLRI.
Therefore, we hypothesized the imbrication of lateral collateral ligament complex via arthroscopic technique can restore the posterolateral rotatory stability and improve the pain and function in patients with the atraumatic posterolateral rotatory instability.
Materials and methods
We reviewed the data of 33 patients with chronic atraumatic lateral elbow pain that were referred to our institution at HRH Princess Maha Chakri Sirindhorn Medical Center for surgery from July 2015 to December 2021. Patients with a diagnosis of atraumatic posterolateral rotatory instability of elbow were recruited for this study. The diagnosis was made when a patient had a history of chronic lateral elbow pain and a positive test on at least one of the posterolateral rotatory instability signs such as chair rise test, push-up test, posterolateral drawer test, pivot shift test, pivot shift apprehension test, or varus stress test. Two views of standard plain radiographs and magnetic resonance imaging of operative elbow were done for the evaluation of the lateral collateral ligament lesion and concomitant pathologies such as the pathological plica and lateral epicondylitis. 16 The patients who had varus or valgus malalignment of elbow and patients with follow-up duration of less than 6 months were excluded.
The demographic data of the followings were recorded: age, gender, side of operated elbow, duration of symptoms, frequency of steroid injection, and duration of follow-up. Furthermore, the signs of posterolateral rotatory instability were examined and reported. The diagnostic reports of the magnetic resonance imaging were established by the radiologists from different hospitals that their patients were referred to our institution. Findings from arthroscopy, which were ulnohumeral gap, drive-through sign, and concomitant pathology, were noted. The outcomes for the hypothesis were range of motions (flexion, extension, pronation, and supination), Quick Disabilities of the Arm, Shoulder and Hand (Quick-DASH) score, Mayo Elbow Performance Index (MEPI) and visual analog score (VAS) for pain. These outcomes were recorded preoperatively and at 6 weeks, 3 months, 6 months, and 12 months postoperatively then annually.
The preoperative and postoperative values of the outcomes for the hypothesis were compared and analyzed using the statistic test of paired t-test by SPSS statistic, IBM, version 26. The last follow-up value was used for the postoperative value in the analysis.
Surgical technique
The patient underwent the procedure under general anesthesia in a lateral decubitus position. The pneumatic tourniquet was applied high on the operative arm. The operative arm was laid on an armrest device with the elbow rest at 90° flexion in a resting position that allowed full extension and deep flexion. The entire limb was prepared from the tourniquet end to the fingertip. The standard waterproof drape was used.
The routine arthroscopic examination for the anterior compartment was performed through the proximal anteromedial portal as a viewing portal and the anterolateral portal as a working portal. The concomitant pathological plica was resected by a 3.5-mm motorized shaver, ConMed® Sterling Cuda blade®, and a bipolar arthroscopic radiofrequency cautery, ConMed® Edge®, with a 90-degree probe. For the concomitant lateral epicondylitis, the extensor carpi radialis brevis insertion was debrided and released by the same shaver and cautery.
After the complete examination and management of the anterior compartment, the posterior and posterolateral portals were created. For the posterior compartment pathologies, the direct posterior portal was used as the viewing portal and the posterolateral portal as the working portal.
Looking through the viewing posterior portal, normally, the camera sheath could not be driven through the radiocapitellar joint and the ulnohumeral gap could not be opened more than 2 mm or more than one probe’s tip, even with forceful supination in elbow extension position being applied (Figure 1). If those abnormal appearances were present, lateral collateral ligament complex would be considered insufficient. The posterior plica, lateral olecranon plica, and cartilage lesion were eliminated in this step of the operation. Arthroscopic viewing of the elbow from the posterior (transtriceps) portal. (a) Ulnohumeral gap without forceful forearm supination, (b) ulnohumeral gap with forceful forearm supination, (c) positive drive-through sign, able to push arthroscopic camera sheath through posterolateral gutter via posterior portal.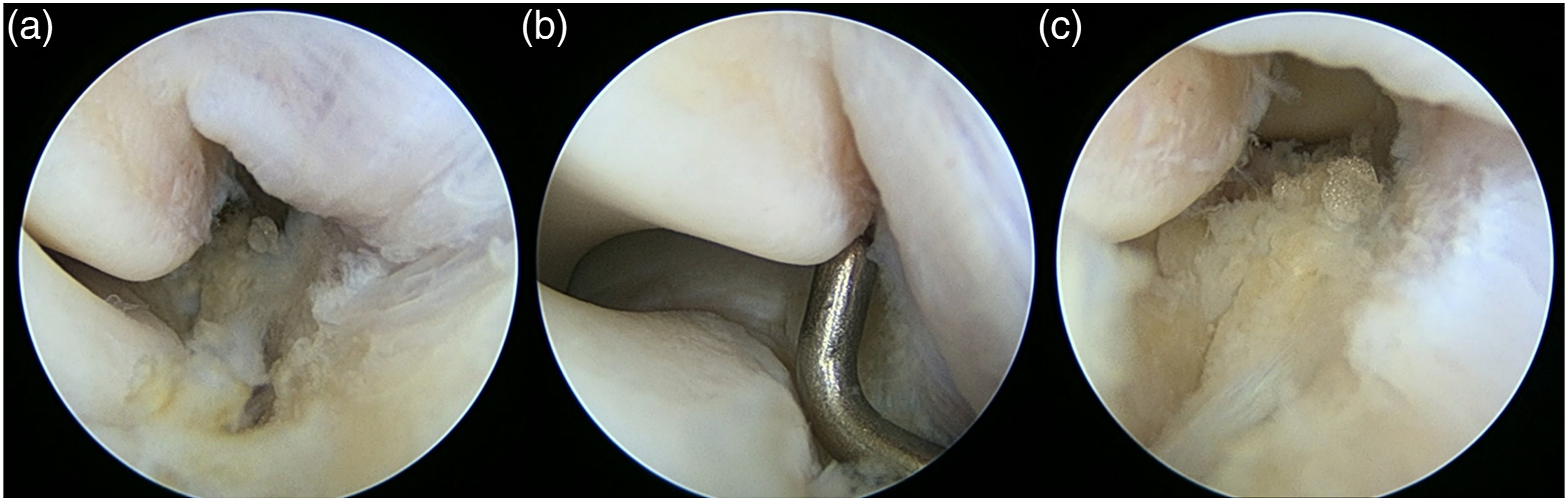
After the management of all concomitant pathologies, the arthroscopic lateral collateral ligament imbrication was performed. While viewing from the posterior portal, the 2.6-mm bioabsorbable suture anchor, Conmed® Press FT®, was inserted posteriorly to the lateral epicondyle after cortical debridement (Figure 2(a)) through the posterolateral portal. A small incision was created posteriorly to the radial head. The Arthrex® Banana SutureLasso® was used to penetrate through the lateral forearm fascia, the anconeus muscle, the lateral collateral ligament, and the capsule for retrieving the suture end one by one. After retrieving all the sutures (Figure 2(b) and (c)), the sutures were tied subcutaneously over the lateral forearm fascia with the elbow in extension and forearm in neutral rotation. The ulnohumeral gap and drive-through sign were examined after this procedure (Figure 2(d)). Arthroscopic viewing of the elbow from the posterior (transtriceps) portal. (a) Lateral cortex of lateral condyle was debrided, (b) double-load suture-anchor was inserted posterior to the lateral epicondyle (star) and Banana SutureLasso was pierced from the fascia to the capsule (arrow), (c) four ends of the suture was retrieved outside before knot tightening, (d) after knot tightening, the gap between bone and soft tissue was closed. (All the suture ends were passed all the way through lateral collateral ligament, anconeus muscle, and forearm fascia then were tied over the fascia).
The operated elbow was protected with a hinged elbow brace for 6 weeks after the operation. The elbow was allowed for full flexion but limited extension at 45°, 30°, and full extension at 0, 2, and 4 weeks postoperatively, respectively. The isometric arm muscle strengthening could be done immediately after the operation. The forearm extensor strengthening exercises were allowed at 6 weeks postoperatively. The pivot activities such as chair rise and push-up were allowed at 12 weeks postoperatively.
Results
Demographic data and results.

Quick-DASH score: quick disabilities of arm, shoulder and hand score; MEPI: mayo elbow performance index; VAS: visual analog scale; OP: operative.
Posterolateral rotatory instability signs.


MRI demonstrated lesions of a patient who had lateral epicondylitis (tear of extensor carpi radialis brevis origin, red arrow), humeral insertional tear of lateral collateral ligament (green arrow), and pathological plica (yellow arrow).
MRI and arthroscopic findings.

RCL: radial collateral ligament; LUCL: lateral ulnar collateral ligament.
Intraoperatively, there was evidence of capsular defect, which was an indirect sign of lateral epicondylitis, in six patients, pathological plica in seven patients, and posterolateral osteophyte impingement in two patients. 1 Some pathological lesions were not noted in the MRI report in some cases. All patients had positive on at least one of the arthroscopic signs for posterolateral rotatory instability. There was one patient (NO. 2) whose suture anchor failed intraoperatively. In this situation, mini-incision was done to remove the failed anchor and a new anchor was inserted. Then the imbrication procedure through arthroscopic technique was proceeded as other cases were done.
Postoperative range of motion from the arthroscopic LCL imbrication had satisfying results in all four directions. Even though the mean flexion arc during early postoperative rehabilitation was about 100°, but it showed to improve after 6 weeks and were fully gained by 12 weeks, postoperatively. In final follow-up, none of the patients had range of motion deficit (Figure 4). The average for postoperative range of motion in flexion, extension, pronation, and supination were 136.88 (130–140), 0, 80 (60–90), and 88.75 (80–90) degrees, respectively. The comparison between the pre- and post-operative range of motion was not statistically significant. The symptoms and signs of the posterolateral rotatory instability disappeared in all patients. There was statistically significant improvement of outcomes between pre- and post-operative Quick-DASH score (mean 55.62 vs 7.62, p = .004, 95%CI = 21.32–74.65), MEPI (mean 50.00 vs 96.87, p = .000, 95%CI = −63.43–−30.31), and VAS for pain (mean 8.14 vs 1.28, p = .000, 95%CI = 5.13–8.58) (Table 1). There was no complication that required a reoperation. Range of motions.
Discussion
Lateral epicondylitis presented with lateral elbow pain has been commonly diagnosed in general practice. However, many other pathologies can mimic and cause chronic lateral elbow pain, such as pathological plica, posterolateral impingement, radiocapitellar joint cartilage lesion, and PLRI.1–4,9,11 The PLRI was described by O’Driscoll in 1991. 11 Insufficiency of lateral ulnar collateral ligament, in both traumatic and atraumatic causes, caused a discomfort or apprehension feeling during pivot activity such as pushing up or rising from a chair.
In the atraumatic causes, local steroid injection inducing, repetitive stress on lateral collateral ligament, and abnormal dynamic strain from ECRB tendinopathy were the common causes reported recently.1,3,4,6,11 Following the previously published literature, we believed the local steroid injection to lateral epicondyle may lead to the PLRI. In our study, all eight patients received the steroid injection with at least one dose of triamcinolone (mean 2.37, range 1–4 times) for treating the lateral elbow pain. Furthermore, not only the toxic effect of the steroid but also the injection technique may be the concerning risk factor that damage the surrounding soft tissue. The peppering injection technique had an evidence of poorer results compared with a single injection. Bellapianta J, et al. concluded peppering technique may damage to already compromised tendon and surrounding soft tissue, which can lead to recurrent pain and poor results. 5
In our study, the varus stress test, posterolateral drawer test, pivot shift test, pivot shift apprehension test, push-up test, and chair rise tests were positive 50% (3/6), 37.5% (3/8), 25% (2/8), 100% (8/8), 87.5% (7/8), and 87.5% (7/8), respectively. The pivot shift apprehension test showed the highest sensitivity. In Chanlalit’s study, 17 98% of patients with non-complicated tennis elbow had a negative result in the pivot shift apprehension test. With the outcome in the aforementioned study combined with the good sensitivity results in this study for this test, we suggest the PLRI must be concerned and can be ruled out by pivot shift apprehension test.
According to the literature in chronic PLRI, the lateral ulnar collateral ligament (LUCL) reconstruction could still be a good surgical option.3,4,6–8,10,11,13,14 According to Chanlalit and Dilokhuttakarn’s report, 1 staged arthroscopy and LUCL reconstruction with harvested graft had established excellent results in atraumatic PLRI. However, the disadvantages of the reconstruction were tendon graft harvesting and open surgery which could cause complications, for example, donor site pain, heterotrophic ossification, or more pain producing. 18 As the arthroscopy and associated instrument had developed, many arthroscopic-based procedures for lateral collateral ligament repair were invented and had resulted with good outcomes.4,10,12,14,15 Moreover, the atraumatic PLRI and concomitants intraarticular lesion can be simultaneously managed. So, we changed the strategy from open reconstruction to the arthroscopic procedure. In our series, there was a statistically significant improvement of outcomes between pre- and post-operative Quick-DASH score (mean 55.62 vs 7.62, p = .004, 95%CI = 21.32–74.65), MEPI (mean 50.00 vs 96.87, p = .000, 95%CI = −63.43 to −30.31), and VAS for pain (mean 8.14 vs 1.28, p = .000, 95%CI = 5.13–8.58) in their last follow-ups (mean 16.12, 9–24 months). None of the patient had range of motion deficit (postoperative range of motion in flexion, extension, pronation, and supination were 136.88 (130–140), 0, 80 (60–90), and 88.75 (80–90) degrees, respectively) or any complication that requires re-operation.
In other arthroscopic management of atraumatic lateral elbow instability, Arrigoni P reported the results of arthroscopic radial lateral collateral ligament (RLCL) plication in 27 patients with symptomatic minor instability of the lateral elbow. 19 This study used anterior compartment approach for application of suture anchor and for plication of RLCL. Post-operative Quick-DASH score was 9.1 (0–25) points. Mean post-operative flexion was 141.1° and extension was 0°. In 96.3% of the patients obtained good or excellent subjective results; however, only 16 patients (59%) gained full elbow motion, seven patients had restricted flexion range of motion and eight patients had restricted extension range of motion. The range of motion result was different when compared with our study. In our study, all motion arcs of elbow were fully gained. Even though patients were less likely to gain full flexion arc during early postoperative rehabilitation, but their flexion arc showed to improve after 6 weeks and were fully gained by 12 weeks, postoperatively. In final follow-up, none of the patients had range of motion deficit. The use of different suture anchor placement (anterior vs posterior), plicated structure (RLCL versus annular ligament and anconeus’s fascia) and tension of plicated soft tissues may be the reason for the different result.
Strength of this study is that it is the novel surgical technique that really can eradicate the problem of atraumatic PLRI with significant satisfying clinical results. Limitation in this study is the small sample size. However, this number of sample is considered a large group for such non-concerning and missed clinical scenario, which actually becomes the strength of this study. Complication was not found in this study but might possibly happen with higher sample size or longer duration of follow-up. Long-term outcomes for this technique and comparison with other techniques still should be further studied.
In conclusion, besides lateral epicondylitis, PLRI and other pathologies should also be concerned in patients with chronic lateral elbow pain. The arthroscopic lateral collateral ligament imbrication and eradication of other elbow pathologies, such as lateral epicondylitis and intra-articular lesions, can be performed in a single operation. Moreover, this minimal invasive technique can avoid the complications of the open surgery and does not need the tendon graft.
Footnotes
Acknowledgements
We feel grateful and give the credits to all of our department’s members for all their helps and supports.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.